Achalasia Cardia: An Interesting Variation as a Large Neck Swelling
Haris Manzoor Qadri1, Arun Y. Dehadaray2, Maitri Kaushik3, Danish Zamir Andrabi4
1Assistant Professor, Department of Otorhinolaryngology, Shrimati Kashibai Navale Medical College and Hospital,, Pune, India.
2Professor, Department of Otorhinolaryngology & Head Neck Surgery, Bharti Vidyapeeth Medical College, Pune, India.
3Professor & HOD, Department of Otorhinolaryngology & Head neck Surgery, Bharti Vidyapeeth Medical College, Pune, India.
4PG Resident, Department of Otorhinolaryngology & Head Neck Surgery, Bharti Vidyapeeth Medical College, Pune, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Danish Zamir Andrabi, Gulshan Jaffery, Reyazat Teng, Khanyar, Srinagar, Jammu & Kashmir-190003, India.
Phone: 8698364949 (pune),
E-mail: danish_andrabi@yahoo.co.in
In this report we present a case of large neck swelling that turned out to be achalasia cardia, not a very common presentation of this disease. An elderly female presented with complain of progressive dysphagia, aspiration and regurgitation of food along with right sided neck swelling measuring 10x5 cm. It was associated with weight loss. X-ray chest depicted an unusually large mass in paramediastinal region parallel to right mediastinal border showing central lucencies. A CT scan of neck revealed a gross dilatation of cervical and thoracic oesophagus. Oesophagus enlargement was enormous to the extent that it could be palpated in the neck compressing airway. This presentation of large neck swelling turning out to be a huge dilatation of esophagus on CT, depicts one of the many interesting variations that this condition can present as.
Benign neck swelling mega oesophagus, Cardiospasm, Dysphagia, Motility disorder
Case Report
An 80-year-old female was brought to otolaryngology of OPD of our tertiary care teaching hospital with chief complains of progressive dysphagia since one year which was more for liquids than solids, right sided swelling of neck since three months. She also gave history suggestive of aspiration, regurgitation of food, weight loss and loss of appetite. There was history of recurrent lower respiratory tract infections and on and off fever ranging from 100-1010F. Endoscopic biopsy taken eight months back turned out to be negative for malignancy.
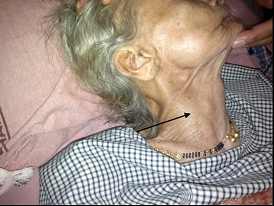
On examination of neck there was a single swelling approximately 10x5 cm [Table/Fig-1], ovoid in shape on right side of neck, extending from mid sternocleidomastoid to clavicle. There were dilated veins over the swelling. Skin over swelling was normal. On palpation swelling was fluctuant, non-tender, reducible with negative trans illumination. No rise of local temperature over swelling. Laryngeal crepitus was present. No bruit auscultated over the swelling.
Provisional diagnosis: Oesophageal malignancy, Cold abscess, Hemangioma, Chagas disease.
Hematological investigations revealed that patient was anaemic (Hb-7.8 g/dl) with TLC 13500/cumm. Blood gas analysis revealed pH : 7.34, pCO2: 38, HCO3- : 24.2, PaO2 : 90, SPO2 : 95%
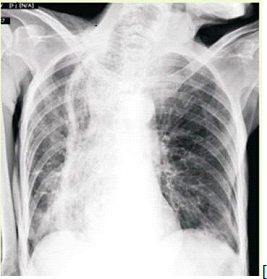
X-ray chest showed large paramediastinal mass running parallel to the right mediastinal border showing central lucencies with a thick wall seen over its lateral aspect. It showed atelectasis both in mid and lower zones of lungs [Table/Fig-2]
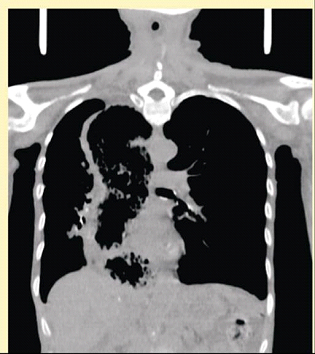
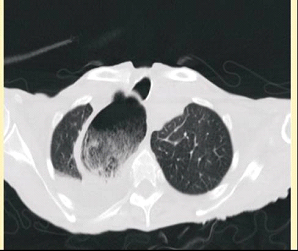
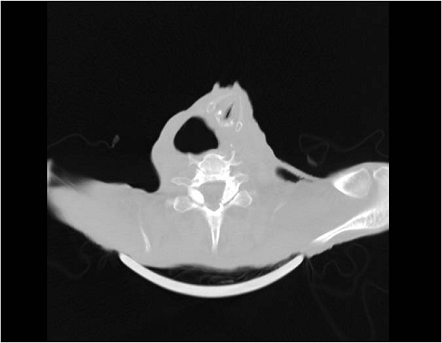
MSCT neck and thorax showed unusually gross dilatation of the cervical and thoracic oesophagus was noted with residual food particles within the dilated oesophagus. A fluid level was seen within the oesophagus at the cervicothoracic junction. The oesophagus was seen in the right paramediastinal region extending from the thoracic inlet at the level of the diaphragm. At the level of the gastro-oesophageal junction it crossed the midline. Smooth tapering of the distal oesophagus was seen at the level of the gastro-oesophageal junction showing a “beak like” appearance. There was a compression and displacement of the laryngeal airway contralaterally by the oesophagus, which was more so at the level of the pyriform sinuses. Volume loss of right lung was noted along with subsegmental collapse of lateral basal segment of right lower lobe was noted. Compensatory emphysema of the left lung was noted. Bilateral pleural effusion was noted moderate on the right and minimal on the left [Table/Fig-3a,3b,3c,3d].
A nasogastric tube was inserted, the major part of nasogastric tube remained in the grossly dilated esophagus. The mega - esophagus was filled with undigested food particles which was aspirated twice daily and patient was kept nil by mouth. The neck swelling which was due to gross dilatation of esophagus used to get decompressed with aspiration. A diagnosis of achalasia cardia was made and patient was offered treatment of either pneumatic dilatation or Botox injection. Patient and relatives opted for treatment with Botox injection.
Follow up of the patient: patient was followed up for three months. Symptoms were relieved partially with improvement in oral intake. Swelling was reduced completely post-treatment.
10X5 cm swelling on right side of neck
X-ray chest showing paramediastinal mass and lung atelectasis
MSCT neck & thorax: coronal section showing dilated cervical and thoracic oesophagus
Axial cut: thoracic oesophagus with residual food particles
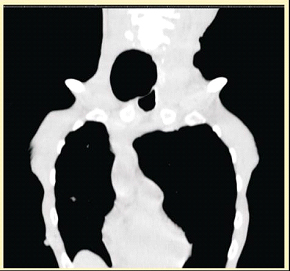
Axial cut: cervical oesophagus compressing and displacing laryngeal airway contralaterally
Discussion
Primary achalasia has absent peristalsis with incomplete relaxation of the lower oesophageal sphincter due to loss of ganglion cells in the oesophageal myentric plexus [1] . The result is impaired oesophageal emptying and resistance to antegrade flow, leading to dilated and elongated oesophagus. If untreated, achalsia cardia can attain mega sizes. Dysphagia is the most cardinal symptom in such patients and present in 90% of the cases [2] . Other common symptoms are regurgitation, gastroesophageal reflux, weight loss and chest discomfort or pain. Some patients present with features of recurrent respiratory infections due to the aspiration of regurgitated contents of the esophagus. Average incidence of this disease is 1 per 100,000 persons [3] .
Radiograph in form of X-ray chest and Ba Swallow reveals dilated esophagus with retention of barium. A homogeneous mediastinal widening, air-fluid levels, absence of gastric air bubble and complications such as pneumonia due to recurrent aspirations. CT scan helps to differentiate a primary from secondary causes of achalasia [4] .
In a report by Dr. Suresh Chandran et al., a mega oesophagus was incidentally found during a routine health checkup in an asymptomatic patient but did not present as a neck swelling [5] . This patient’s presentation was unique since the oesophagus was such mega size that it could be externally seen as a neck swelling. As per Elis FG, Achalasia cardia can be mild, moderate or severe based on severity of enlargement [6] . He has classified the mega esophagus when size is 6cm or more. In the present case it was huge esophagus as the size was more than 10 cm. A recent update on achalasia cardia, in journal of neurogastroenterology and motility, in 2010 also does not describe severe achalasia cardia having a prominent neck swelling [7] .
Conclusion
Rare presentation of severe achalasia cardia with a palpable neck swelling has been presented in this case report.
[1]. Woodfeild CA, Levine MS, Rubesin SE, Langlotz, CP, Laufer I, Diagnosis of primary versus secondary achalasia, reassessment of clinical and radiographic criteria.AJR. 2000 175:727-31. [Google Scholar]
[2]. DO Castell, Achalasia and diffuse esophageal spasmArch Intern Med 1976 136(5):571-79. [Google Scholar]
[3]. DL Francis, DA Katzka, Achalasia: update on the disease and its treatment.Gastroenterology. 2010 139:369-74. [Google Scholar]
[4]. M Carter, RC Deckmann, RC Smith, MI Burell, M Traube, Differentiation of achalasia from pseudoachalasia by computed tomographyAm J Gastroenterol. 1997 92:622-24. [Google Scholar]
[5]. Chandran Dr. Sursh R, Mega esophagus an atypical presentationKMJ 2009 4:181-83. [Google Scholar]
[6]. FG Ellis, The natural history of achalasia of the cardiaProc. Roy. Soc. Med 1960 53:663-66. [Google Scholar]
[7]. richter Joel E, Achalasia – an updateJ Neurogastroenterol Motil. 2010 16(3):232-42. [Google Scholar]