Sarcomatoid Renal Cell Carcinoma: Case Report and Review of Literature
Maryann Margaret Bukelo1, Srikanth U2, Sharada Rai3
1Assistant Professor, Department of Pathology, Kasturba Medical College, Mangalore, Karnataka, India.
2Lecturer in Anatomical Pathology, Department of Paraclinical Sciences, The University of the West Indies ,Trinidad and Tobago.
3Associate Professor, Department of Pathology, Kasturba Medical College, Mangalore ,Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr Srikanth Umakanthan, Lecturer in Anatomical Pathology, The University of the West Indies, Faculty of Medical Sciences, Department of Para Clinical Sciences, Building 5, Room# 30, EWMSC, Mount Hope. Trinidad and Tobago.
Phone: : +(868) – 473-0728,
E-mail: dr.u.srikanth@gmail.com
Sarcomatoid renal cell carcinoma is a tumour with aggressive behaviour. It is a form of dedifferentiated carcinoma with high incidence of metastases to the lungs. We report a case of 55-year-old male who presented with complaints of loin pain and hematuria. The biopsy confirmed sarcomatoid variant of renal cell carcinoma.
Laparotomy, Sarcomatoid carcinoma
Case Report
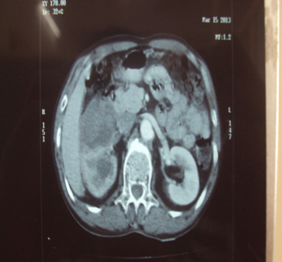
A 55-year-old male presented with history of loin pain and hematuria. The Computerized Tomography (CT scan) showed a renal mass [Table/Fig-1a] and even bilateral lung metastasis. Laparotomy was performed and the nephrectomy specimen was sent for histopathology.
CT scan shows a heterogenous, exophytic, necrotic mass in the mid 1/3rd of the non - excreting right kidney extending into the pelvis and causing lower calyceal dilatation
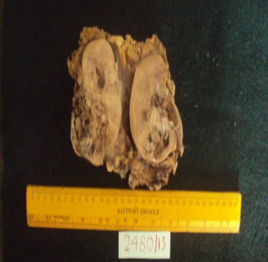
Cut section shows a variegated mass occupying the centre and lower pole with areas of haemorrhage and necrosis
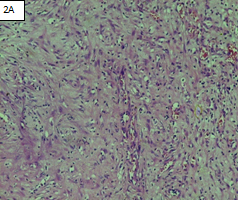
Section shows sheets of spindle cells in whorled pattern (H&E 10X)
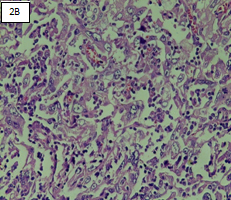
Section shows large polygonal cells with eccentric nuclei and abundant eosinophilic cytoplasm (H&E 10X)
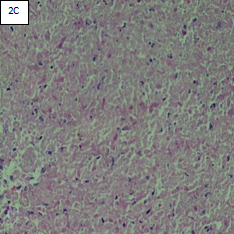
Section shows extensive areas of necrosis and chronic inflammatory infiltrate (H&E 10X)
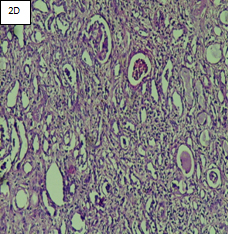
Section show tumor extending into the surrounding renal parenchyma (H&E 10X)
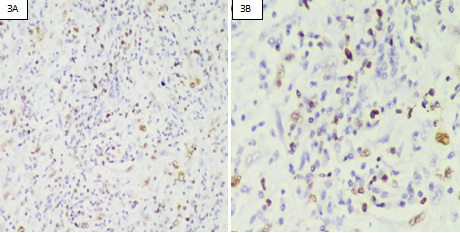
Stain for MIB-1 shows strong immunoreactivity
Gross Examination
A radical nephrectomy specimen [Table/Fig-1b] consisted of right kidney surrounded by perinephric adipose tissue and Gerota fascia (300g), measuring 10.5 X 8 X 7cms. The ureter is dilated and measuring 3 cms in length. A 6 X 5.5 X 4.5 cms poorly defined, variegated mass occupied centre and lower pole with areas of haemorrhage and necrosis. The renal pelvis is dilated. A defect is identified in the renal capsule near the hilus measuring 2 X 1 cms. The surrounding renal parenchyma is thinned out at the lower pole. The renal vein and adrenal gland is normal and free of tumour.
Microscopic Examination
The sections of kidney show a malignant tumour composed predominately of sheets of spindle cells with pleomorphic nuclei and prominent nucleoli[Table/Fig-2a]. This indicates sarcomatoid differentiation. Focally the tumour cells have a polygonal shape with granular eosinophilic cytoplasm and pleomorphic nuclei [Table/Fig-2b]. The Fuhrman nuclear grade was G4. In addition, bizarre tumour giant cells are seen along with extensive areas of necrosis and dense chronic inflammatory infiltrate [Table/Fig-2c]. The tumour is seen extending into the perirenal adipose tissue near the renal pelvis [Table/Fig-2d] and also into the adjacent renal parenchyma along with dilated tubules, few showing luminal cast and chronic inflammatory infiltrate. The ureter, renal artery and adrenal gland are free of tumour.
Imaging
CT scan showed a heterogenous, exophytic, necrotic mass (5.7 x 6.1 x 5.5 cms) in the middle 1/3rd of the non - excreting right kidney extending into the pelvis and causing lower calyceal dilatation. The visualized lung bases showed multiple rounded lesions suggestive of multiple lung metastases.
Immunohistochemistry
MIB -1 immunohistochemical stain was done for confirmation which showed strong immunoreactivity [Table/Fig-3a,b].
After histological diagnosis, the patient was referred to oncology treatment for post chemotherapy and further management. The patient lost to further follow up.
Discussion
Renal cell carcinoma (RCC) is the most common malignancy of the kidney and consists of multiple subtypes [1]. RCC with sarcomatoid differentiation is a tumour with aggressive behaviour [2]. They have a high incidence of metastases to the lung and bone at presentation [3]. On immunohistochemistry they are positive for MIB-1, AE1/AE3, vimentin, EMA which supports epithelial origin [4]. Sarcomatoid RCC was initially felt to represent a primary renal sarcoma, however now it is considered a form of dedifferentiated carcinoma and is therefore not a distinct histologic entity. It is defined as any subtype containing foci of pleomorphic spindle cells and is seen in high grade RCC, at the end stages of disease progression. Sarcomatoid differentiation is reported to occur in approximately 1-8 % of RCC’s. Heterologous sarcomatoid transformation has been reported in other histologic subtypes of sarcomatoid RCC, and conventional RCC is the main type of tumour to undergo heterologous transformation [5]. On microscopic examination, two main histologic subtypes of sarcomatoid component have been described. A fibrosarcoma like appearance and malignant fibrous histocytoma characterized by a greater degree of nuclear pleomorphism and occasional multinucleated osteoclast like giant cell. Rare cases show hemanigopericytoma like pattern. Some tumours’ can represent as undifferentiated sarcoma. In our case it had a fibrosarcoma like appearance. Distant metastases were most frequent to the lungs as present in our case [6].
Investigation into the imaging features of sarcomatoid RCC has been limited. The current trend is to report any sarcomatoid component seen at pathologic analysis, regardless of what percentage of he total lesion comprises, as treatment and follow up protocols may be affected. Therefore, it would be beneficial if the presence of sarcomatoid dedifferentiation could be suggested based on imaging characteristics, potentially with MRI. On MRI, sarcomatoid RCC have an irregular or infiltrative morphology and demonstrate heterogeneous T2 signal intensity and enhancement. Internal necrosis and evidence of aggressive local or distant behaviour was frequently observed [7].
Sarcomatoid chromophobe RCC frequently have multiple gains (polysomy) of chromosomes 1, 2, 6, 10 and 17 [8,9]. Mutations of p53 tumour suppressor gene and frequent complex desmosomal junctions confirm the epithelial nature of the neoplasm [10].
[1]. Reiter Michael, Schwope Ryan, Clarkson Arthur, Sarcomatid renal cell carcinoma: A case report and literature review.J Radiol Case Rep 2012 6(4):11-6. [Google Scholar]
[2]. Dall’oglio Marcos F, Liberknecht Marco, ValterGouveia Anna Alexandre C Sant, Leita Katia R, Sarcomatoid differentiation in renal cell carcinoma: Prognostic implication.International Braz J Urol 2005 31(1):10-116. [Google Scholar]
[3]. Roohi Mahera, Tanvir Imrana, Qazi Sumera, Sarcomatoid renal cell carcinomaInt J Pathol 2012 10(1):39-40. [Google Scholar]
[4]. N Kuroda, M Toi, M Hiroi, Review of sarcomatoid renal cell carcinoma with focus on clinical and pathobiological aspectsHistopathol. 2003 18:551-55. [Google Scholar]
[5]. M De Peralta – Venturina, H Moch, M Amin, Sarcomatoid differentiation in renal cell carcinoma: A study of 101 casesAm J Surg Pathol 2001 25(3):275-84. [Google Scholar]
[6]. JC Cheville, CM Lohse, H Zincke, Sarcomatoid renal cell carcinoma: An examination of underlying histologic subtype and an analysis of associations with patient outcome.Am J Surg Pathol 2004 28(4):435-41. [Google Scholar]
[7]. AB Rosenkrantz, H Chandarana, J Melamed, MRI findings of sarcomatoid renal cell carcinoma in nine patientsClin Imaging 2011 35(6):459-64. [Google Scholar]
[8]. Quironga Gabriela, HemaKhurana Shen Steven, Sarcomatoidchromophobe renal cell carcinoma with heterologous sarcomatoid elements: A case report and review of literature.Archives of pathology and laboratory medicine 2009 133(11):1857-60. [Google Scholar]
[9]. M Brunelli, S Gobbo, P Cossu – Rocca, L Cheng, O Hes, Chromosomal gains in the sarcomatoid transformation of chromophobe renal cell carcinomaMod Pathol 2007 20(3):303-09. [Google Scholar]
[10]. Y Morikawa, K Tohya, Y Kusuyama, M Masui, C Wakasugi, Sarcomatoid renal cell carcinoma. An immunohistochemical and ultrastructural studyIntUrolNephrol 1993 25(1):51-8. [Google Scholar]