Role of CT Imaging with Volume Reconstruction in Hemi Facial Hypertrophy: A Pediatric Case Report
Gurubharath I1, Lakshmi Sudha Prasanna Karanam2, Ramesh P3
1Consultant, Department of Radiolgy,Guru Raghavendra Trust Hospital, Kk Nagar, Chennai, India.
2Consultant, Department of Radiolgy,Guru Raghavendra Trust Hospital, Kk Nagar, Chennai, India.
3Consultant, Department of Radiolgy,Guru Raghavendra Trust Hospital, Kk Nagar, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr.Gurubharath, Consultant, Department of Radiolgy, Guru Raghavendra Trust Hospital, Kk Nagar, Chennai, India.
E-mail: kavinilangovan@yahoo.co.in
Hemifacial hypertrophy is a rare congenital disorder more common in males.It involves the soft tissue, hard bones and teeth of the face.Its etiology is unknown and multiple theories have been postulated.
We present a 6-year-old male with hemifacial hypertrophy and describes the importance of CT volume reconstruction in this condition.
CT, Hemifacial Hypertrophy, Volume Rendering
Case Report
A 6-year-old male child was presented with facial asymmetry. The mother states the deformity was present from birth which consequently increased with age and became more noticeable as the child had grown. He was born to non-consanguineous parents at full term by caesarian section. Apart from the facial deformity there are no other associated clinical conditions or medical problems. Hormonal assays and karyotyping showed no biochemical or chromosomal abnormalities. Serial axial sections and coronal sections of the orbital floor, maxilla and mandible were taken on mutidetector CT scanner (64 SLICE PHILIPS SCANNER) without administration of contrast agent. There is abundant fat in left side of face including left frontal and temporal extra-cranial soft tissue, periorbital soft tissue, cheek and chin. Also there is thickening of left frontal, parietal and temporal bones, enlarged left orbit, left maxillary sinus and left mandible [Table/Fig-1,2]. Pterygoid, temporalis and masetter muscles show decreased bulk. There is evidence of thickening of pterygoid plates on left side. Deviation of nasal septum is seen to left side with bilateral concho bullosa. Volume reconstruction [Table/Fig-3] was done for the same and the importance of the reconstruction protocol in showing the extent of the lesion is well depicted. These reconstructed images give more clear information to the surgeon and aid in further planning the treatment.
Discussion
Hemifacial hypertrophy was first described by Meckel in 1822 [1].It usually gets accentuated around puberty and is more common in males than in females.
Various theories have been proposed postulating the underlying etiology of Hemifacial Hypertrophy (HFH). These include hyperplasia of the neural crest cells, vascular lymphatic, hormonal and asssymetrical development of the neural fold [2].
Isolated HFH is a diagnosis of exclusion. In our present case we did not find any other syndromic association. The known clinical conditions that can cause the facial asymmetry reported in the viewsliterature include Beckwith-Wiedemann syndrome (BWS), Proteus syndrome, Schimmelpenning syndrome, Neurofibromatosis and Klippel-Trenaunay syndrome [3].
The associated hemihypertrophy in BWS is due to the mosaic form of macrosomia [4]. HFH may be associated with other skeletal deformities and Central nervous system abnormalities. Skeletal system involvement can be in the form of polydactyly, syndactyly and clubfoot. CNS manifestations include epilepsy, strabismus and mental retardation. Such associations are not seen in the present case.
Rowe classified HFH into total and partial types. In the first type there was involvement of all the viscerocranial structures involving the frontal bone, mandible, midline and the ear. In partial types all the structures will not be involved as in our patient [5]. This condition usually has good prognosis.Other findings that can also be seen in HFH will be enlarged tongue, lips with widening of the palate [3]. Because of the absence of myohyperplasia in the present case, nasal deviation is seen to the opposite normal side. Myohyperplasia in HFH is reported as the dominant feature by Urban and Roland in their case report [6]. However, in our present case we did not find any muscle hyperplasia.
The combination of spiral CT and 3D reconstruction with Volume Rendering (VR) allows rapid and detailed examination of the musculoskeletal system as in our present case. Both the surface rendering and volume rendering techniques helps in 3D reformation. Volume rendering incorporates all the data and gives the realistic image; hence VR is more valuable in giving the information in the musculoskeletal disorders. 3D-CT volume rendering technique can distinguish craniofacial anatomy accurately in bone and soft tissue protocols as shown in our present case [7]. The 3D images helps the clinician in better understanding of the extent of the lesion and helps in planning the reconstructive procedures such as ostectomy, orthognathic surgical procedures.
CT sagittal reformatted image(a,b) showing the increased soft tissues in the left frontal, temporal extracranial region and increased muscle density

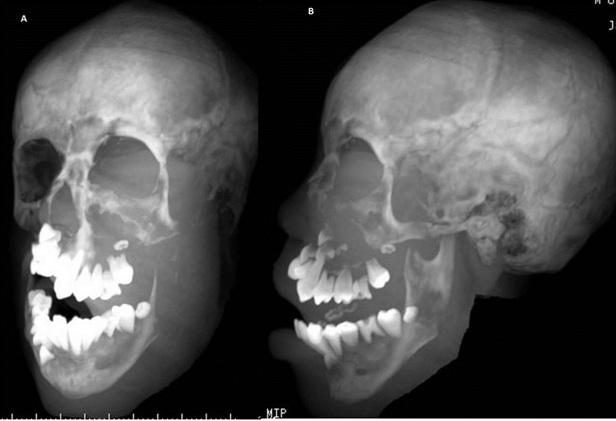
Maximum intensity projection image (a,b) showing the 3D image with hypertrophied soft issue and bone on the left side in the oblique and lateral viewsliterature
Volume reconstructed images(a,b,c) showing the hypertrophied bone and the asymmetry with a clear depiction as compared to the right side

Conclusion
The present case report is a case of partial hemi facial hypertrophy with the features as above and role of imaging with special emphasis on volume rendering in 3D reformation is described.
[1]. RJ Gorlin, LH Meskin, Congenital hemihypertrophy: review of the literature and report of a case with special emphasis on oral manifestations.J Paediatr. 1962 61:870-9. [Google Scholar]
[2]. S Lee, R Sze, C Murakami, Hemifacial myohyperplasia: description of a new syndrome.Am J Med Genet. 2001 103:326-33. [Google Scholar]
[3]. JO Lawoyin, JO Daramola, DO Lawoyin, EH Kass, Congenital hemifacial hypertrophy: report of two cases.Oral Surg Oral Med Oral Pathol. 1989 68:27-30. [Google Scholar]
[4]. MR DeBaun, EL Niemitz, DE McNeil, Epigenetic alterations of H19 and LIT1 distinguish patients with Beckwith-Wiedemann syndrome with cancer and birth defects. Am J Hum Genet. 2002 70:604-11. [Google Scholar]
[5]. NH Rowe, Hemifacial hypertrophy: review of the literature and addition of four cases.Oral Surg Oral Med Oral Pathol. 1962 15:572-87. [Google Scholar]
[6]. PP Urban, B Roland, R Kalra, Congenital isolated hemifacial hyperplasia.J Neurol. 2009 256:1566-9. [Google Scholar]
[7]. MG Cavalcanti, SS Rocha, MW Vannier, Craniofacial measurements based on 3D-CT volume rendering: implications for clinical applications.Dentomaxillofac Radiol. 2004 533(3):170-6. [Google Scholar]