Case Report
A 19-year-old female reported to the Department of Conservative Dentistry and Endodontics, with pain in relation to upper right posterior teeth. Clinical examination revealed maxillary right first and second premolars having temporary restoration, which was placed in a private clinic two months back. Both the teeth were tender on percussion. Medical history was non-contributory. Radiographic examination revealed that the temporary restorations were extending into the pulp chamber of the involved teeth. The roots of 14 were doubly curved (Bayonet or ‘S’ shaped) and that of 15 showed a sharp curvature at middle third [Table/Fig-1]. From the clinical and radiographic findings, a diagnosis of previously initiated therapy associated with symptomatic apical periodontitis was made in relation to 14 and 15. Prior to the formulation of endodontic therapy the degree of curvature was determined by using Schneider method and it showed severely curved canals in relation to both the teeth.
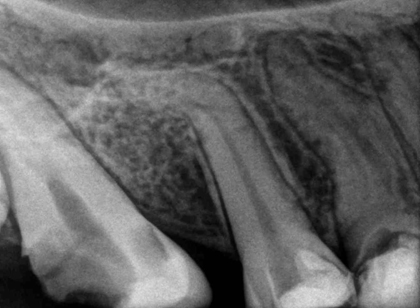
Preoperative radiograph showing dilacerated canal in relation to 15 and Bayonet or S-shaped root canals in relation to 14.
With informed consent, local anesthesia was administered using 2% lignocaine and 1:100000 Adrenaline and Endodontic therapy was initiated under rubber dam isolation. Temporary restoration was removed and the access cavity of 14 and 15 were modified. The pulp chamber was irrigated by following standardized irrigation regimen using 5.25% of sodium hypochlorite (NaOCl), 17% ethylene diamine tetraacetic acid (EDTA) and physiological saline. For verifying the patency of the root canals, No.8 and 10 stainless steel K-files (Mani, Inc, Japan) were used. No.15 K file glide path was ascertained up to the radiographic working length [Table/Fig-2]. The estimated length till the curvature was marked on the engine-driven instrument and coronal flaring was done. Gate-Glidden (GG) drills were used for orifice enlargement up to size No 3. Working length was then confirmed using an apex locator (Root ZX, J. Morita, Japan) in both the teeth. Sequential filing of the curved canals was done using nickel titanium (NiTi) hand files No. 15, 20, and 25 (Mani, Inc, Japan) to the working length. The apical portions of the canals were prepared using short amplitude filing. Special emphasis was placed on frequent irrigation of the root canal and recapitulation was done to avoid blockage by dentinal debris and to remove the necrotic remnants of the pulp tissue. Final cleaning and shaping was carried out using Hyflex CM rotary files up to 4% 40 size of the instrument. Calcium hydroxide was used as an intracanal medicament and closed dressing was given for six days.
Working length radiograph

In the next visit, the canals were flushed with saline and dried with paper points. A master cone radiograph was taken with 40 size 4% gutta percha in both the teeth [Table/Fig-3]. The lateral condensation method of obturation was performed using AH Plus sealer. The post-obturation restoration was done with composite resin to maintain a good coronal seal [Table/Fig-4]. The patient was given postoperative instructions and recalled for further follow up. At three months review, the patient was absolutely asymptomatic and there was no radiographic sign of any periapical disease [Table/Fig-5].

Post obturation radiograph

Three months follow-up radiograph

Discussion
It is uncommon to observe a tooth with a straight root and a straight root canal because most teeth exhibit some curvature of the root canal. In addition, most canals have multiple planes of curvature throughout their length [1]. Endodontic therapy will be successful only when a thorough disinfection of the entire root canal system is achieved. However, the presence of curvatures may pose difficulty in root canal instrumentation and cleaning [2].
The term dilaceration first used by Tomes in 1848, refers to an angulation or a sharp bend or a curve in the root or crown of formed tooth or a deviation or bend in the linear relationship of a crown of a tooth to its root [3]. Tooth is considered to have a dilaceration toward the mesial or distal direction if there is a 90° angle or greater along the axis of the tooth or root. Dilaceration can also be defined as a deviation of the apical part of the root by 20° or more [3]. The condition is believed to be consequent to trauma during the period of tooth formation, when the position of the calcified portion of the tooth is changed and the reminder of the tooth is formed at an angle [3].
Root canal curvatures may be apical, gradual, sickle-shaped, severe-moderate-straight curve, bayonet / S-shaped curve and dilacerated curve [4]. Curved root canals exhibit great difficulty in cleaning, shaping and obturation of the root canal system [5]. The final results of the instrumentation of curved root canals may be influenced by several factors such as the flexibility and diameter of the endodontic instruments, instrumentation techniques followed during the management, location of the foramina opening, and the hardness of dentin [6,7]. Ledge formation, blockages, perforations and apical transportation are undesirable occurrences that have been observed after the preparation of curved root canals [8]. Therefore determining the degree of curvature of root canal before starting the endodontic treatment is mandatory.
Several methods have been advocated to determine root canal curvature using periapical radiographs. Schneider proposed a method to calculate the curvature based on the angle that is obtained by two straight lines. Schneider’s method involves firstly drawing a line parallel to the long axis of canal in the coronal third of root canal. A second line is drawn from the apical foramina to intersect the first line. The Schneider’s angle is measured with the intersection of these lines on a hard copy of the diagnostic radiographic printout [9]. Accordingly, the degree of root canal curvature is categorized as: [10]
Straight: 5° or less
Moderate: 10-20° and
Severe: 25-70°.
Schneider angle, when used in combination with the radius and length of the curve, may provide a more precise method for describing the apical geometry of canal curvature. Gunday et al., introduced the term “canal access angle” (CAA) and its related parameters which provide more information about the coronal geometry of canal curvature [11]. Determining the curvature of the root will permit the maintenance of the curves during root canal preparation and prevents structural deformations of endodontic instruments. Thus, diagnosis of root dilacerations before endodontic treatment has a critical importance in either preventing complications during treatment or ensuring a good treatment result [10].
The success of root canal treatment depends largely on complete biomechanical debridement of the canals and the elimination of microorganisms from the root canal system. Preparation of curved canals presents one of the greatest challenges in endodontics and is fraught with difficulties. The shortcoming of periapical radiographs is that only the curvatures in mesio-distal plane is visible, although curvatures in the bucco-lingual plane are also evident in many teeth. In dilacerated teeth, it is often difficult to explore and negotiate the root canals. This inability to continuously follow the root canal curvature might result in blocking of the canal, ledging, apical cavitation such as transportation and/or zipping, perforation, and instrument separation [4].
According to Vertucci [12] maxillary premolars are the teeth with the maximum anatomic variations. One such variation that occurs often in the maxillary premolars is the ‘S’ shaped or bayonet shaped root canal. The S-shaped canal has two curves, with the apical curve being very difficult to negotiate. The chances of strip perforation are very high in these root canals. Guttman [13] suggested preflaring the coronal 1/3rd of the canal (at the expense of the tooth structure) to reduce the angle of curvature. Once this procedure is completed, it is easy to negotiate the remainder of the root canal. It is important to formulate a customized treatment plan for the management of curved canals. Prior to initiation of treatment, the degree of curvature has to be ascertained. In the case presented we have followed Schneider method of curvature determination, because of its simplicity and wide acceptance [9,10].The roots of 14 were doubly curved (Bayonet or ‘S’ shaped) and the root of 15 showed a sharp curvature at middle third, with severely curved root canals in relation to both the teeth. After determining the degree of curvature, we have followed various techniques for the management of curved canals [14,15].
Endodontic file has the tendency to straighten up in the canal, and hence it is difficult to control removal of dentine along the entire length of file in push pull motion. The incidence of procedural errors can be reduced by:
Decreasing the restoring force by means of which straight file has to bend against the curved dentine surface and
Decreasing the length of the file which is aggressively cutting at a given span.
Decreasing the force can be done by the following-
(a) Precurving the file: A precurved file traverses the curve better than a straight file. Precurving is done in two ways:
Placing a gradual curve for the entire length of the file
Placing a sharp curve of nearly 45° near the apical end of the instrument
(b) Extravagant use of smaller number files as they can follow canal curvature, because of their flexibility. The smaller size files should be made super loose in the canal before using larger files to negotiate the canal without force.
(c) Use of intermediate size of files: It allows smoother transition of the instrument sizes to cause smoother cutting in curved canals, e.g. cutting 1 mm of No. 15 file makes it No. 17 file as there is an increase of 0.02 mm of diameter per mm of length.
(d)Use of flexible files (NiTi files, Flex R files): As these files help in maintaining shape of the curve and avoid procedural errors like ledge, elbow or zipping of the canal.
Decreasing the length of actively cutting files is achieved by the following:
(a) Anti-curvature filing.
(b) Modifying the cutting edges of the instrument by dulling the flute on outer surface of apical third and inner portion of middle third, which can be done by a diamond file.
(c) Changing the canal preparation techniques, i.e. use of coronal pre-flaring and crown down technique.
Tendency to create narrow canal shapes minimizing access of irrigants and creating potential to allow debris to be pushed apically. Attempts at overcoming the deficiencies of these instruments resulted in a number of preparation techniques that aimed to reduce iatrogenic defects and produce canals with a more flared shape.
A significant advancement in root canal preparation with hand instruments was made with the introduction of balanced force movements of files. The balanced force movements of the file are [14]:–clockwise 60°, so that it binds against the wall and advances apically – anticlockwise 120° with apical pressure, so as to crush and break off the engaged dentinal wall.
-clockwise 60° without apical advancement, allows flutes to be loaded with debris and removed from the canal.
The balanced force technique is less prone to cause iatrogenic damage, decreases the extrusion of debris apically and maintains the instruments centrally within the root canal [14].
Conclusion
Severe root curvature may pose substantial difficulty in cleaning and shaping as well as obturation of the root canal. A thorough knowledge about internal anatomy of the tooth, appropriate instrumentation techniques and customized treatment planning depending upon the degree of curvature will help manage curved canals, prevent complications and enhance the quality of the treatment.
[1]. Cohen S, Burns RC, Pathways of the pulp 2002 948th edSt LouisMosby:243-74.:325-31.:644-45. [Google Scholar]
[2]. Ingle JI, Root canal preparationIn: PDQ Endodontics 2005 Hamilton, OntarioBC Decker:129 [Google Scholar]
[3]. Jafarzadeh H, Abbott PV, Dilaceration: review of an endodontic challengeJ Endod 2007 33:1025-30. [Google Scholar]
[4]. Jain N, Tushar S, Curved canals: ancestral files revisitedIndian J Dent Res 2008 19:267-71. [Google Scholar]
[5]. Gupta S, Endodontic Miscellany: Conventional Endodontics for Complex root-canal morphologyEndodontology 2002 14(1):28-9. [Google Scholar]
[6]. Curtis ML, 100’s of Pearls on Endodontics. Chapter 5: Tips and Tricks for Common Endo 2005 Hundreds of Pearls, LLCMichael L. Curtis, Publisher:93-5. [Google Scholar]
[7]. Mounce R, Negotiating challenging mid root curvatures: rounding the bendDentistry Today 2007 26(2):108 [Google Scholar]
[8]. Hamasha AA, Al-Khateeb T, Darwazeh A, Prevalence of dilaceration in Jordanian adultsInt Endod J 2002 35:910-2. [Google Scholar]
[9]. Schneider SW, A comparison of canal preparations in straight and curved root canalsOral Surg Oral Med Oral Pathol 1971 32:271-75. [Google Scholar]
[10]. Estrela C, Bueno MR, Sousa-Neto MD, Pecora JD, Method for Determination of Root Curvature Radius Using Cone-Beam Computed Tomography ImagesBraz Dent J 2008 19(2):114-18. [Google Scholar]
[11]. Gunday M, Sazak H, Garip Y, A comparative study of three different root canal curvature measurement techniques and measuring the canal access angle in curved canalsJ Endod 2005 31:796-98. [Google Scholar]
[12]. Vertucci FJ, Root canal anatomy of the human permanent teethOral Surg Oral Med Oral Path Oral Radiol Endod 1984 58:589-99. [Google Scholar]
[13]. Guttman JL, Problem solving in endodontics 1997 3rd edMissouriMosby - Year book Inc:116 [Google Scholar]
[14]. Ansari I, Maria R, Managing curved canalsContemp Clin Dent 2012 3(2):237-41. [Google Scholar]
[15]. Gufran Ali S, Mulay S, Negotiating challenging root curvatures: Review & case reportsNJDSR 2012 1(1):56-59. [Google Scholar]