Myofibroblastoma of Female Breast Masquerading as Schirrous Malignancy – A Rare Case Report with Review of Literature
K Bharathi1, VS Ajay Chandrasekar2, G Hemanathan3, S Anuradha4
1Assistant Professor, Department of Pathology,Shri Satya Sai Medical College and Research Institute,Nellikuppam, Tamilnadu, India.
2Associate Professor, Department of Surgery,Shri Satya Sai Medical College and Research Institute,Nellikuppam, Tamilnadu, India.
3Postgraduate, Department of Pathology,Shri Satya Sai Medical College and Research Institute,Nellikuppam, Tamilnadu, India.
4Professor, Department of pathology,Shri Satya Sai Medical College and Research Institute,Nellikuppam, Tamilnadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr.Bharathi, K No 26 A, Gopal nagar Narayanapuram, pallikaranai Chennai 600100, India.
Phone: 9962531082
E-mail: bharathi.pathos@gmail.com
Myofibroblastoma is a rare benign mesenchymal tumour of the breast commonly reported in males. It is a spindle cell neoplasm exhibiting myofibroblastic differentiation with characteristic immunohistochemical staining. Herein, we present a case of myofibroblastoma in a premenopausal female which was mimicking like malignancy clinically. Lump was growing rapidly in size measuring 8 cm x 6 cm and stony hard in consistency. Mammogram showed a large homogeneous hyperdense lump suggestive of fibroadenoma, Hamartoma and fibromatosis. FNAC and trucut biopsy of mass could not be done due to stony hard consistency. Hence excision biopsy was done. Histopathological examination revealed the tumour as myofibroblastoma. Immunohistochemical staining for markers of myofibroblasts like CD-34 and Vimentin showed strong positivity. A negative expression for cytokeratin was noted. This case is presented for its rarity, unusual clinical presentation and stony hard consistency.
Myofibroblastoma Mesenchymal tumours CD 34 Vimentin
Case Report
A 45-year-old premenopausal women came to our surgical Out Patient Department(OPD) with left breast lump of 6-months duration. Lump was non tender, stony hard and freely mobile occupying the lower outer quadrant of left breast. No family history of breast cancer. Differential diagnosis of fibromatosis, myofibroblastoma and scirrhous carcinoma were given due to its stony hard consistency. Swelling was growing rapidly measuring 8 x 6 cm in size without any nipple discharge or retraction. Axillary lymphnodes were not palpable. Mammogram showed a large homogeneous hyperdense lump measuring 8 x 6 cm suggestive of fibroadenoma, Hamartoma and fibromatosis. FNAC and Biopsy could not be done as the hardness of the breast mass did not allow the needle penetration. Hence we proceeded with excision biopsy under general anaesthesia.
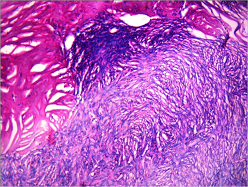
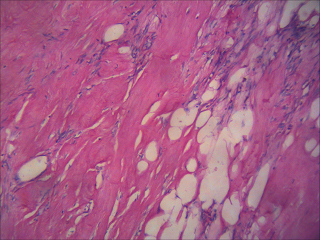
Grossly lump was well circumscribed, unencapsulated lobular hard mass with pushing borders. Cut-surface showed homogeneous lobulated whitish lump [Table/Fig-1]. Microscopic examination showed fascicles of uniform spindle cells forming whorls occasionally [Table/Fig-2]. Cells were separated by bands of hyalinised collagen, infrequent mitotic figures and entrapped adipocytes [Table/Fig-3]. No epithelial elements were seen. A diagnosis of myofibroblastoma was given considering clinical, microscopic and radiological features. Immunohistochemical staining showed diffuse strong positivity for CD34, Vimentin [Table/Fig-4,5]. Cytokeratin immunostaining showed a negative expression. Immunohistochemistry helped us to confirm our diagnosis and in ruling out spindle cell carcinoma(metaplastic carcinoma) of breast.
Patient had an uneventful postoperative period and was discharged on the second postoperative day. She was advised for regular follow up. Two years of follow-up till now showed no recurrence or metastasis.
Gross photograph shows lobulated homogeneous neoplasm with pushing borders.

Photomicrograph shows benign spindle cells arranged in whorls and fascicles. (H & E, 100)
Shows dense collagen and entrapped adipocytes. ( H & E, 100).
Photomicrograph shows diffuse Vimentin positivity of spindle cells. (H & E, 100). [
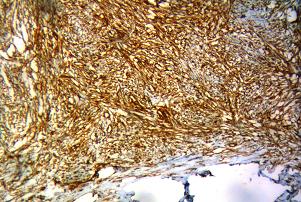
Photomicrograph shows CD 34 positivity of spindle cells. (H & E, 100)

Discussion
Myofibroblastoma is a rare benign spindle cell neoplasm of breast. About 80 cases have been reported in literature [1]. Though commonly reported in males, incidence is now found to be equal in both the sexes. It is essential to diagnose and distinguish myofibroblastoma from other spindle cell tumours for deciding the exact line of management.
The term ‘myofibroblastoma’ was first described by Wargotz in 1987 [2] . It is an uncommon tumour composed of bland looking spindle cells showing myofibroblastic differentiation. It presents often as a solitary mobile painless mass with a well circumscribed margins. Average size of the tumour is 1 to 4 cm but can reach larger dimensions [3,4] .Incidence of mammary myofibroblastoma is found to be more in elderly age group of both the sexes. Other common sites of occurence are skin, soft tissue and lymphnode.
Myofibroblastoma appears as a solid homogeneous well circumscribed hypoechoic mass devoid of calcification in mammogram [5] . Grossly lump is homogeneous solid well circumscribed with foci of mucoid and lipomatous changes. Cystic change, hemorrhage and necrosis are rarely seen. Fine needle aspiration cytology is often helpful in giving a preoperative diagnosis [6] .
Diagnostic histopathological and cytological features of myofibroblastoma are fascicles and whorls of spindle cells with benign oval nucleus. Hyalinised collagen bundles with interspersed spindle cells, adipocytes and mast cells is seen predominantly. Neoplasm may not show epithelial elements, atypical mitosis or necrosis. Foci of cartilaginous, osseous, myomatous and lipomatous change can also be seen. Mast cells can be seen in the stroma. Histomorphological variants are epitheloid, fibrous, deciduoid, cellular, collagenised, lipomatous, myxoid, infilterative myofibroblastoma [7] . It is necessary to recognize and pinpoint these variants to avoid diagnostic dilemma. An infiltrating myofibroblastoma has a invasive growth pattern with entrapped fat and glands and it mimics a malignancy and fibromatosis [7] . In our case FNAC and trucut biopsy could not be done due to stony hard consistency. Large cellular myofibroblastoma with epitheloid appearance can mimic metaplastic carcinoma and has to be confirmed by immunohisto chemistry [8] .
Our closest differential diagnosis is fibromatosis which resembles myofibroblastoma clinically and histologically. Fibromatosis is solid, locally aggressive, locally recurrent mass and is negative for CD34. Other differential diagnosis to be considered are phyllodes tumour, nodular fasciitis, leomyoma, schwannoma, spindle cell lipoma, sarcoma, pseudo angiomatous stromal hyperplasia, solitary fibrous tumour, Dermato Fibrosarcoma Protruberans [9] . Myofibroblastoma should be distinguished from Spindle cell carcinoma, malignant fibrous histiocytoma and metaplastic carcinoma with the help of ancilliary techniques.
Myofibroblastomas are strongly immunoreactive for Vimentin, CD34, Desmin, Smooth Muscle Actin, fibronectin, type IV collagen. Weakly reactive for S-100, estrogen receptor, progesterone receptor and negative for Cytokeratin, Ki- 67 [10-12] .
Cytogenetic studies revealed a specific chromosomal rearrangement 13q14 in myofibroblastoma. Similar genetic change is also reported in solitary fibrous tumour and spindle cell lipoma showing a relationship between these tumours [13,14] .
Surgical excision of lump is the treatment of choice. Taccagni et al reported the recurrence of myofibroblastoma along with pleura pulmonary metastasis after one month and diagnosed it as myofibrosarcoma of breast [15] . Close follow-up is advised in such cases [15] . In our case recurrence or metastasis is not seen after two years of follow up.
Conclusion
Myofibroblastoma is a rare benign stromal tumour of breast. It is essential to diagnose myofibroblastoma as it behaves in a benign fashion and excision biopsy is usually adequate. In some cases it may mimic a malignant stromal tumour and has to be confirmed using immunohistochemistry. Myofibroblastoma show strong positivity for Vimentin, CD34 & Desmin whereas spindle cell carcinoma (metaplastic carcinoma) show positivity for cytokeratin and Ki 67. Close follow is advised to look for any recurrence. Breast lumps with spindle cell morphology should be diagnosed with the help of clinical, radiological, cytological findings and should be correlated with immunohistochemical features for confirmation.
[1]. NS Salemis, NS Salemis, E Tsiambas, V Tsantilas, C Seretis, Rapidly growing myofibroblastoma of the breast diagnosed in a premenopausal woman: Management and review of the literatureBreast Dis. 2003 34(1):29-4. [Google Scholar]
[2]. ES Wargotz, SW Weiss, Myofibroblastoma of the breast: sixteen cases of a distinctive benign mesenchymal tumourAm J Surg Pathol 1987 11(7):493-2. [Google Scholar]
[3]. M Mele, V Jensen, A Wronecki, G Lelkaitis, Myofibroblastoma of the breast: case report and literature reviewInternational journal of surgery case reports 2011 2(6):93-6. [Google Scholar]
[4]. MC Abeywarda, Abeysekara Priyantha HP Siriwardana, KF Abbas, P Tanner, An unusually large myofibroblastoma in a male breast; a case report.J Med Case Rep. 2008 :2-151. [Google Scholar]
[5]. YS Lee, M Gilcrease, Y Wu, WT Yang, Myofibroblastoma of the breast: Imaging featuresEur J Radiol Extra 2009 73:13-5. [Google Scholar]
[6]. M Powari, R Srinivasan, BD Radotra, Myofibroblastoma of the male breast: a diagnostic problem on fine-needle aspiration cytologyDiagn Cytopathol 2002 26:290-3. [Google Scholar]
[7]. G Magro, Mammary MyofibroblastomaArch Pathol Lab Med 2008 132:1813-0. [Google Scholar]
[8]. B Shivali, S Kataria, K Chandramouleeswari, S Anita, Myofibroblastoma Breast with Unusual Morphological Features. Cytohistopathological Diagnostic Pitfalls And Role Of Immunohistochemistry - Review Of LiteratureJ Clin Diagn Res 2013 7(10):2323-5. [Google Scholar]
[9]. SN Shah, Giant myofibroblastoma of breast: a case report.Indian Journal of Pathol Microbiol. 2007 50(3):583-5. [Google Scholar]
[10]. A Qureshi, N Kayani, Myofibroblastoma of breastIndian Journal of Pathol Microbiol. 2008 51(3):395-6. [Google Scholar]
[11]. P Das, A Sharma, R Arora, MK Singh, Myofibroblastoma of breast.Indian Journal of Med Paediatr Oncol 2008 29:16-9. [Google Scholar]
[12]. A Sharma, AK Sen, NK Chaturvedi, R Yadav, Myofibroblastoma of male breast: a case reportIndian Journal of Pathol Microbiol 2008 50:326-8. [Google Scholar]
[13]. U Flucke, JM Han, Kurken Van, T Mentzel, Cellular angiofibroma: analysis of 25 cases emphasizing its relationship to spindle cell lipoma and mammary type myofibroblastoma.Mod patho 2011 24:82-9. [Google Scholar]
[14]. ME McMenamin, CDM Fletcher, Mammary myofibroblastoma type of soft tissue: A tumour closely related to spindle cell lipomaAm J surg pathol. 2001 25(8):1022-9. [Google Scholar]
[15]. G Taccagni, E Rovere, M Masullo, L Christensen, B Eyden, Myofibrosarcoma of breast : Review of Literature on Myofibroblastic tumours and criteria for defining Myofibroblastic Differentiation.Am J Surg pathol 1997 21(4):489-6. [Google Scholar]