For ages Catheter Angiography has been the gold standard of coronary angiography. It also carries risk in patients with coagulation disorders and conditions related to increased vessel fragility. Catheter angiography is contraindicated in some patients [1]. This makes it necessary to have a safe and reliable screening modality for evaluation of coronary arteries [2,3].
MDCT (Multi detector computed tomography) has come a long way in assisting in the diagnosis of coronary heart disease. With the advancement in technology efforts have been made to increase the accuracy in diagnosing coronary heart diseases. Cardiac Imaging by MDCT was first done on 16-slice MDCT, which then progressed to 64-slice, however both of these have their limitations especially in terms of heart rate requirements and temporal resolution. Cardiac Imaging is the challenge of 21st century and it is being answered by 128 slice dual source CT as it has good temporal resolution, high scanning speed as well as low radiation dose.
MDCT analyses the various parameters like calcium score, individual coronary arteries and their branches, myocardial perfusion and left and right ventricular functions.
In a 2 x128-slice dual source CT, two X-ray tubes with different peak kilo-voltages (80 and 140 kVp) are used simultaneously in a dual energy mode to acquire two sets of images of the desired anatomic region. For routine coronary applications both tubes work at same kV (120 kVp) in adaptive and spiral mode. Both X-ray tubes are mounted on the rotating gantry with an angular offset of 90 degrees and cover 180 degrees alternatively at isocenter with 0.6mm collimation. The single gantry rotation time is 0.28 second and its temporal resolution is good (75 milliseconds). This allows a total coverage in z- direction 48mm in single rotation.
The dose values of the dual source Siemens CT scanner thus lie far below that of an intracardiac catheter examination. A scan of the entire heart can be performed in only 250 milliseconds, which is less than half a heartbeat.
The objective of ours study was to evaluate diagnostic accuracy between 128 slice Dual source CT coronary angiography and invasive catheter coronary angiography and to find common arteries involved in coronary vascular disease, so that 128 slice dual source CT can be used as an alternate, safe and reliable screening modality for evaluation of Coronary arteries.
Materials and Methods
This is a prospective comparative study done at Department of Radiodiagnosis, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, UP, India, between Dec 2011 to May 2013.
Inclusion Criteria in our study were both gender patients with mild to intermediate risk of suspected CAD selected from Cardiac OPD on the basis of clinical symptoms, ECG & TMT findings.
Exclusion Criteria were patient with established or suspected acute coronary syndrome, with Atrial Fibrillation or with serum Creatinine > 150 mmol/L (>2 mg/dL (normal range 0.7-1.3 mg/dL (61.9-115 μmol/L). A baseline creatinine of 2mg/dL may indicate a normal kidney function.
In this study 40 patients were evaluated observing the inclusion and exclusion criteria and following full written consent by patients. Each patient received a cardiac CT examination within 1 to 2 days prior to the conventional angiography examination.
Forty patients with suspected CAD were assessed using both 128-slice CT coronary angiography and invasive coronary angiography and results were compared. SIEMENS 128-slice Dual Source Flash Definition CT was used for CT coronary angiography. Prospective ECG gating was used in patients with heart rate of <85bpm with a fluctuation of less than 10bpm and retrospective ECG gating was done in patients with heart rate of >90bpm.
Non-ionic 370 mg/ml Iodinated I.V. contrast was used. Dose was calculated using Test Bolus Technique in which a test bolus of 10ml contrast followed by 20ml of saline chaser was first injected and the Time for Peak Enhancement in Ascending Aorta was calculated. This Peak Enhancement Time was multiplied by Flow Rate of injector i.e. 5ml/sec to know the amount of contrast required for the each patient. Maximum amount of contrast given was 110ml and average amount was 70ml.
Scans were performed from the level of carina, to the level of the hemi diaphragms for coronary arteries study.
For better evaluation of the anatomy and disease process, advanced off-line post-processing techniques, including (multiplanar reconstruction; maximal intensity projections; curved reconstructions; and volume rendering) were performed [Table/Fig-1]. A calcium score was performed using Agatston-Janowitz method in all cases. Oral/ intravenous Beta-blockers were used wherever required. After the scan the system generates best systolic, diastolic and 0 to 100% of cardiac cycle for ejection fraction. This data was transferred to Syngovia workstation for PostProcessing. Coronary arteries were assessed as per 17- segment AHA model{–RCA proximal (1); mid (2); distal (3); PDA (4a); PLV (4b); LM (5); LAD proximal (6); mid (7); distal (8); D1 (9); D2 (10); LCX proximal (11); OM1 (12); LCX mid (13); OM2 (14); LCX distal (15); RI (16)}. Significant disease of the coronary arteries was defined as 50% or more diameter stenosis whereas non-significant disease was defined as diameter stenosis less than 50% [4]. As per Lipinski M et al., study,It appears that the best cut-point for defining significant angiographic disease when evaluating diagnostic tests of ischemia is 75% or greater coronary luminal stenosis [5].
Automated SYNGOVIA software used for evaluation of CT coronary angiography.coronary arteries were assessed as per 17-segment AHA model – RCA proximal (1); mid (2); distal (3); PDA (4a); PLV (4b); LM (5); LAD proximal (6); mid (7); distal (8); D1 (9); D2 (10); LCX proximal (11); OM1 (12); LCX mid (13); OM2 (14); LCX distal (15); RI (16)

Results
Total 40 patients including male & female (36 male & 06 female) were evaluated. The youngest patient was 32 years old & oldest was 73 years old. The mean age of the study group was 54.30 years. The highest number of the patients were in the age group of 51-60 years (44%).
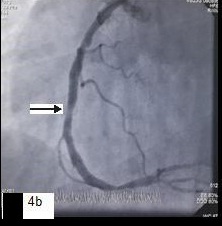
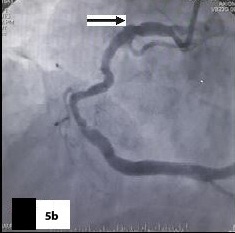
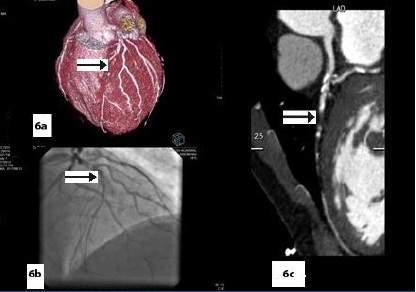
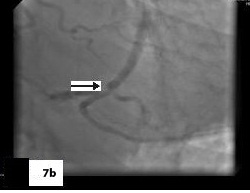
Five patients (12.5 %) had normal angiograms [Table/Fig-2,2b,3,3b], six (15%) had non-significant disease [Table/Fig-4,4b,5a,5b] and 29 patients (72.5%, 26 male & 3 female) had significant disease [Table/Fig-6a,6b],[7a,7band8] on CT coronary angiography, which was also proved on invasive angiography [Table/Fig-9]. The incidence of significant coronary detected was highest in age group of 41-60 years [Table/Fig-10].
Curved reformatted image showing patent stent in RCA;
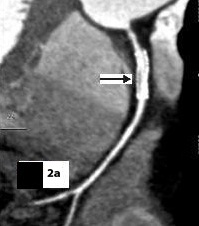
Image showing patent stent in RCA (arrow)
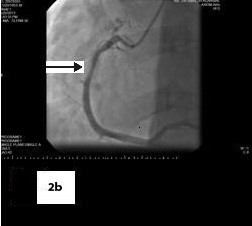
Catheter angiography image showing a normal angiogram

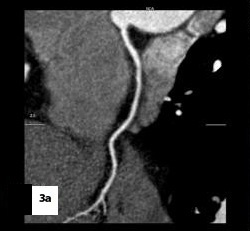
Curved reformatted image,
Catheter angiography image showing non-significant stenosis in mid RCA
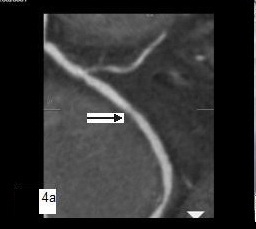
Curved reformatted image with mixed palque

Catheter angiography image showing focal non-significant stenosis in RCA
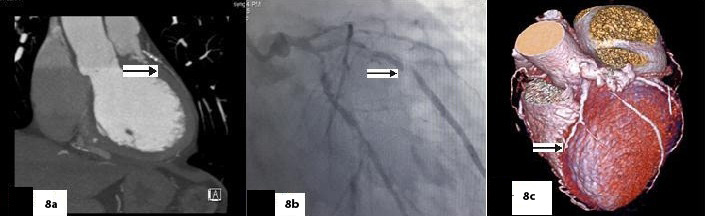
(VRT) & (MPR) images show near complete stenosis of proximal LAD on CT coronary angiography (arrow)
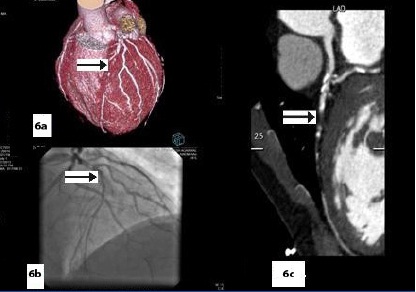
Catheter angiography image showing complete occlusion of LAD in \ proximal segment (arrow)
Curved reformatted image shows non- calcific plaque near origin of OM1 causing significant stenosis,

Catheter angiography image showing significant stenosis of OM1 at origin Significant disease in the absence of calcification
(Sagittal), (Axial), (VRT) images & catheter angiography image showing significant stenosis in mid LAD
Distribution of the severity of coronary artery disease cases on coronary CT angiograms. n (n=40) represents total number of patients in study
| Coronary Angiograms | Number of patients | Percentage |
|---|
| Normal Angiograms | 05 | 12.5 |
| Non significant disease | 06 | 15 |
| Significant disease | 29 | 72.5 |
| Total | 40 | 100 |
Age distribution of the coronary disease cases. N(40) represents total number of patients in study
| Age (years) | Total (Total%) | Normal (Normal%) | Non significant (Non significant%) | Significant (Significant%) |
|---|
| 31-40 | 05 (12.5 %) | 01 (02.5 %) | 01 (02.5 %) | 03 (07.5 %) |
| 41-50 | 09 (22.5 %) | 02 (05 %) | 00 (00 %) | 07 (17.5 %) |
| 51-60 | 17 (42.5 %) | 01 (02.5 %) | 04 (10 %) | 12 (30 %) |
| 61-70 | 06 (15 %) | 01 (02.5 %) | 01 (02.5 %) | 04 (10 %) |
| 71-80 | 03 (7.5 %) | 00 (00 %) | 00 (00 %) | 03 (07.5 %) |
| Total | 40 (100 %) | 05 (12.5 %) | 06 (15 %) | 29 (72.5 %) |
Majority of patient (16/40,40%) had calcium score of zero. Only three patients had a calcium score of more than 400. The mean CT coronary calcium score was 162.3 Agatston units. All 5/16(31.25%) patients who had normal coronary angiograms had a calcium score of zero, All 8/16 (50%) had significant disease and rest 3/16 (18.75%) had non-significant disease. In 40 patients a total of 609 segments were present, out of which 600 segments were evaluable and a total of 184 lesions were used for comparison with invasive angiography of the total 184 lesions detected on both CT and invasive coronary angiography [Table/Fig-11], eight significant lesions were missed on CT coronary angiography. These lesions were involving the branch arteries. The most common location for the presence of significant coronary artery disease was found to be left anterior descending artery, followed by right coronary and left circumflex artery. No significant lesion was missed in these arteries on CT coronary angiography.A lesion is defined as discrete when its length is less than 10 mm, tubular when its length is 10-20 mm and diffuse when length is more than 20 mm [6]. Majority of non-significant lesions were discrete.The right-sided dominance of coronary circulation was most commonly seen [Table/Fig-12].
Artery wise distribution of lesions detected on CT coronary angiography in patients with suspected coronary artery disease N (187) represents total number of lesions detected in study
| Artery | Total number of Non Significant lesions | Total number of Significant lesions |
|---|
| RCA | 25 | 19 |
| PDA/ PLV | 00 | 03 |
| LM | 08 | 03 |
| LAD | 17 | 43 |
| LCX | 23 | 17 |
| Diagonals | 03 | 05 |
| OMs | 08 | 04 |
| RI | 04 | 02 |
| Total | 88 | 96 |
Dominance pattern of coronary arteries on CT angiography. N (40) represents total number of patients in study
| Dominance | Number of patients | Percentage |
|---|
| Right | 25 | 62.5 |
| Left | 10 | 25 |
| Codominant | 05 | 12.5 |
128- Slice dual source CT angiography had an overall sensitivity of 95.26%, specificity of 95.12%, and positive predictive value of 88.46% and negative predictive value of 98.08% with invasive catheter angiography as the gold standard.
Discussion
Many authors have compared the diagnostic accuracy between MDCT coronary angiography and invasive coronary angiography.
Raff et al., [7] reported sensitivity, specificity, positive predictive value, negative predictive value of 64- slice CT as 86%, 95%, 66% and 98% respectively whereas Nikolaou et al., [8] reported in their study a value of 82%, 95%, 72% and 97%. In their study on 64- slice CT coronary angiography to detect significant stenosis, Mollenbruch et al., [9] reported a sensitivity of 87%, specificity of 95%, PPV of 75% and NPV of 98%.
Similarly in our study we found out an overall sensitivity of 95.26%, specificity of 95.12%, positive predictive value of 88.46% and negative predictive value of 98.08%. The false negative cases either had small vessel size, tortuous course, poor opacification or motion blur. All these missed significant stenosis were located in the branch arteries.
Agreement between CT coronary angiography and invasive angiography on a per-segment level was very good and all coronary segments irrespective of their diameter were evaluated. Unlike previous studies [10] where vessels with diameter < 1.5mm were excluded from the study, the present study evaluated all coronary segments irrespective of their diameter. However, the accuracy was better in few branch vessels could be attributed to small vessel size.
Our results are either in accordance with or have a slightly higher value compared to these studies. This result suggests high potential of 128-slice MDCT coronary angiography to detect significant coronary artery stenosis. The present study showed overall high sensitivity, specificity, positive predictive value and negative predictive value. The specificity and the negative predictive value were particularly higher suggesting the ability of modality to correctly identify those individuals who do not have the disease, that is, true negatives.
We also compared the diagnostic accuracy of 128- slice MDCT coronary angiography in subgroup of patients with varying calcium score. We divided the patients into two groups: those with coronary calcium score <100 and >_100 Agatston unit. Twenty Six patients had a calcium score of less than 100. The specificity and positive predictive value were 98.34% and 85.71% respectively. The negative predictive value was 99.16% and the sensitivity was 92.30%. Only 14 patients had a calcium score more than 100. Most (15/21) of the false positive segments belong to patients with calcium score more than 100. In these patients the sensitivity and specificity were 96.10% and 78.20% respectively. The positive predictive value was 89.28% but negative predictive value was 91.00%. The accuracy was better in patients with calcium score <_100 Agatston units. Extensive arterial wall calcification impairs vessel assessment and CT coronary angiography should be avoided in patients with very high coronary calcium score [11]. The presence of coronary calcium induced overestimation of the severity of these lesions on the CT scan. Severe coronary calcification obscures the coronary lumen and can lead to overestimation of lesion severity, resulting in a lower specificity in patients with high calcium scores. Brodoefel et al., in his study [12] also found that image quality was significantly degraded in the presence of Agatston score higher than 400. At the same time, the number of non-diagnostic segments was significantly higher in subgroups of elevated calcium score.
CT angiography is able to visualize in innumerable planes, not only the lumen of coronary arteries but also their walls, the neighboring myocardium, and the cardiac chambers and extra cardiac structures. Van Ooijen et al., [13] also reported that for detection of plaques and stenosis, optimal results were achieved by using VR, MPR, or MIP. For evaluation of aberrant anatomy, VRT is the preferred technique because it provides a good insight into the 3D relationships and course of the coronary artery tree. Disadvantages of CT coronary angiography remain its sensitivity to arrhythmia, high heart rate and vessel wall calcification.
Conclusion
We would like to conclude by saying that the high negative predictive value observed in this study (98.08%) suggests that 128- slice MDCT coronary angiography is a good screening modality for evaluation of patients with equivocal stress test results who might otherwise require invasive angiography. It may also be used to evaluate the coronary artery anomalies or early detection of atherosclerosis in mild to intermediate risk individuals or in coronary evaluation in patients undergoing major non- cardiac surgery.