Dermatology Specific Quality of Life in Vitiligo Patients and Its Relation with Various Variables: A Hospital Based Cross-sectional Study
Nitin Mishra1, Madhur K. Rastogi2, Pratik Gahalaut3, Shikha Agrawal4
1 Associate Professor, Department of Dermatology, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, (UP), India.
2 Assistant Professor, Department of Dermatology, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, (UP), India.
3 Professor, Department of Dermatology, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, (UP), India.
4 Junior Resident, Department of Psychiatry, Deva Mental Health Care, Durgakund, Varanasi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nitin Mishra, 353 Sahukara, Near Kila Police Station, Bareilly, (UP)-243006, India.
Phone: +91-9012303662,
E-mail: dermanitin@gmail.com
Introduction: Vitiligo is an acquired, idiopathic skin disease characterized by progressive loss of the inherited skin color. Vitiligo has a special significance to patients in our country because depigmentation is obvious on dark skin and due to the enormous stigma that the disease carries.
Materials and Methods: One hundred vitiligo patients aged more than 18 years were included in our hospital based study depending on inclusion and exclusion criteria. All the patients were asked to fill a validated Hindi version of DLQI questionnaire. DLQI scores and its interpretation were recorded separately. correlation of DLQI Scores with different variables like age, body surface area, duration of disease and socioeconomic status were studied using Pearson’s correlations. Mean DLQI scores were also compared between different groups.
Results: Male and female patient were statistically similar in all variables, like their age, BSA of the involvement and DLQI score. DLQI interpretation showed that out of 100 patients of vitiligo, 16 felt no effect of vitiligo on their quality of life while 84 patients reported small to very large effect on their quality of life. Out of this 84, 37 felt small effects, 21 felt moderate effect and rest 26 felt very large effect on their quality of life. There was no significant difference among the different groups mentioned except very large effect on quality of life seen significantly more in unmarried patients compared to married one.
Conclusion: Vitiligo although a cosmetic disease without any symptoms, it carry a significant social stigma especially in Indian society. Data interpretation in this study indicates that vitiligo affects QOL in majority of vitiligo patients and such patients require more aggressive and empathic attitude from a dermatologist to cure/improve this so called chronic cosmetic disease.
DLQI, Quality of life, India, Vitiligo
Introduction
Vitiligo is an acquired, idiopathic skin disease characterized by progressive loss of the inherited skin color which leads to white patches and in some cases total depigmentation [1]. Vitiligo is an acquired depigmentary disorder of great concern affecting 1-4% of the world population [2,3]. Vitiligo has a special significance to patients in our country because depigmentation is obvious on dark skin and due to the enormous stigma that the disease carries [4]. Studies that measuring health related quality of life (QOL), such as the dermatology life quality index (DLQI), have shown that vitiligo affects QOL [5–7]. Vitiligo patients have a lower self-esteem as compared to the normal population [8]. Infact studies have shown prevalence of psychiatric morbidity (depressive episodes, adjustment disorders, anxiety) in up to 25% of patients with vitiligo [9,10].
The chronic nature of disease, long term treatment, lack of uniform effective therapy and unpredictable course of disease is usually very demoralizing for patients suffering from vitiligo. The impact of such factors is profound; subjecting them to emotional distress, interfering with their employment or lend them use tension- lessoning, oblivision producing substances as alcohol [11]. Severe depression even suicide attempts due to vitiligo itself has been reported [12]. Society greets vitiligo patients differently as they are stared at, subjected to whispered comments, antagonism, insult or isolation.
Quality of life is a multidimentional index of different social, behavioural and cultural factors. Different tools were developed for measuring quality of life focusing on different conditions and diseases. DLQI, developed in 1994, was the first dermatology-specific quality of life instrument. It has been used for more than 40 different skin conditions in over 80 countries and available in over 90 languages. Its use has been described in over 1000 publications including many multinational studies [13].
The Dermatology Life Quality Index questionnaire [14–16] is designed for use in patients of age more than 16. It is self explanatory and can be simply handed to the patient who is asked to fill it without the need for detailed explanation.
Aim
The aim of this study was to assess the Dermatology specific quality of life and its relation with various variables in vitiligo patients.
Materials and Methods
One hundred vitiligo patients aged more than 18 years who attended the Department of Dermatology S.R.M.S.I.M.S Bareilly, India from october 2011 to November 2013 were included in our cross-sectional hospital based study depending on inclusion and exclusion criterias. All the patients included in this study were literate and able to read and write. Patients with other chronic cutaneous or systemic diseases and illiterate were excluded from the study. Socio-economic classification of the patients enrolled in this study was done using recent kuppuswamy classification [17]. We noted demographic profile of the patients in a specially designed proforma. Affected body surface area (BSA) was calculated by rule of nine [18]. Patients with appearance of new lesions or increase in size of existing lesions in last six months duration were classified as progressive vitiligo and otherwise taken as having stable vitiligo. All the patients were asked to fill a validated Hindi version of DLQI questionnaire. DLQI scores and its interpretation were recorded separately. It is usually completed in one to two minutes.
DLQI questionnaire is classified into 10 questions and each question with 4 possible answers scored from 0 to 3. The DLQI score is calculated by summing the scores of all the questions, resulting in a maximum of 30 and a minimum of 0. The higher the score, the more quality of life is impaired. DLQI score [14–16] interpretation is done as follow:
DLQI score Interpretation
0-1 No effect at all on patient’s life
2-5 Small effect on patient’s life
6-10 Moderate effect on patient’s life
11-20 Very large effect on patient’s life
21-31 Extremely large effect on patient’s life
DLQI scores were correlated with different variables like age, body surface area, duration of disease and socio-economic status using Pearsons correlations. Mean DLQI scores were also compared between males/females, patients with localized/generalized vitiligo, stable/progressive vitiligo and married/unmarried patients with the help of independent sample t-test. All Statistical analysis was done using SPSS Version 22.
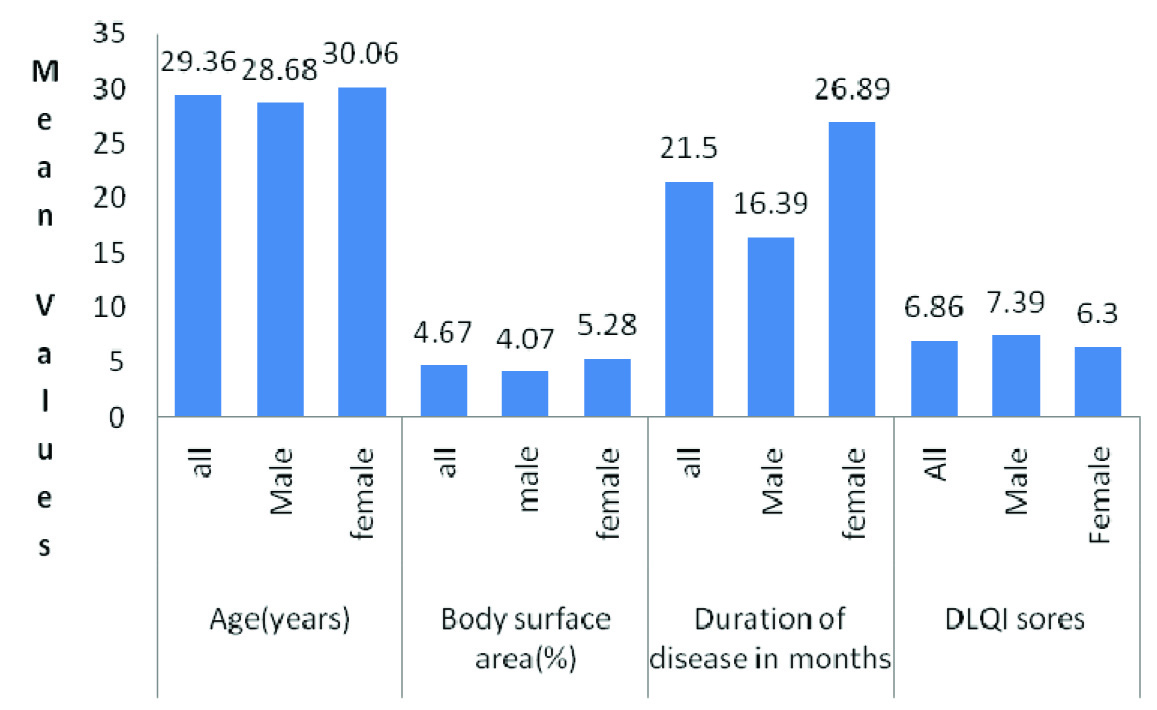
Out of 100 patients included in the study, 51 were male and 49 were female with the mean age of 29.36 ± 12.94 years.
As per [Table/Fig-1] male and female patient were statistically similar in all variables, like their age, BSA of the involvement and DLQI score. Duration of disease was significantly more in females (p-value.042).
Characteristics of the patients
The Socio-economic grading of study patients was done using kuppuswamy scale. Of them 60% of the patients were from middle class while 38% were from lower class, thus majority of patients were from the lower and middle Socio-economic class. Different Socio-economic classes failed to show any significant correlation of DLQI score with age, involved body surface area or duration of disease. Incidentally the Socio-economic scale of the female patients were significantly lower than males (p-value.002 using Mann-Whitney Test).
There was no statistically significant difference seen in mean DLQI scores between different groups as mentioned in [Table/Fig-2].
Comparison of mean DLQI scores in different group of patients
| Demographic variable | No of patients | Mean dlqi ± SD | p-value |
|---|
| Sex | Males | 51 | 7.39 ± 5.74 | 0.324 |
| Females | 49 | 6.30 ± 5.18 |
| Stability of vitiligo | Stable vitiligo | 28 | 5.71 ± 4.43 | 0.194 |
| Progressive vitiligo | 72 | 7.30 ± 5.79 |
| Marital status | Married | 48 | 6.00 ± 4.89 | 0.132 |
| Unmarried | 52 | 7.65 ± 5.90 |
| Localization of vitiligo | Localized vitiligo | 89 | 6.58 ± 5.26 | 0.263 |
| Generalized vitiligo | 11 | 9.09 ± 6.81 |
*p-value determined by independent sample t- test
As mentioned in [Table/Fig-3], the DLQI scores were significantly and negatively correlated with education. Correlation of DLQI score with age, BSA and Socio-economic class was not significant.
Correlations of DLQI scores with different variables
| Variables | Age | BSA | Education | Socio-economic Class | Duration of disease |
|---|
| PearsonCorrelation With DLQI score | –.045 | .004 | –.252(*) | .173 | –.066 |
| Sig. (2-tailed) | .655 | .967 | .011 | .084 | .516 |
| Number of patients | 100 | 100 | 100 | 100 | 100 |
As mentioned in [Table/Fig-4], the DLQI interpretation showed that out of 100 patients of vitiligo, 16 felt no effect of vitiligo on their quality of life while 84 patients reported small to very large effect on their quality of life. Out of this 84, 37 felt small effects, 21 felt moderate effect and rest 26 felt very large effect. There was no significant difference among the different groups mentioned in [Table/Fig-4] except very large effect on quality of life seen significantly more in unmarried patients compared to married one (p= .04 using Fisher exact test).
Interpretation of DLQI score
| Variables | DLQI Interpretation | No effect n=16 | Small effect n=37 | Moderate effect n=21 | Very large effect n=26 | Extremely large effect n=0 | Total n=100 |
|---|
| Sex | Male | 5 | 20 | 13 | 13 | 0 | 51 |
| Female | 11 | 17 | 8 | 13 | 0 | 49 |
| Type of vitiligo | Localized | 14 | 35 | 18 | 22 | 0 | 89 |
| Generalized | 2 | 2 | 3 | 4 | 0 | 11 |
| Marital status | Married | 13 | 21 | 12 | 10 | 0 | 56 |
| Unmarried | 3 | 16 | 9 | 16 | 0 | 44 |
| Stability of vitiligo | Stable | 3 | 14 | 7 | 4 | 0 | 28 |
| Progressive | 13 | 23 | 14 | 22 | 0 | 72 |
Discussion
Mean age of the patients in the present study was 29.36 years which is almost to other similar studies done in past [19,20]. More of the male patients (31.4%) were either graduate or post graduate compared to females (16.4%); this difference may a reflection of gender discrimination and male dominant society in India.
Majority of the patients were from the lower and middle (98%) Socio-economic class. This may have occurred because the study was done in medical college located at relatively remote location where majority of patients come from rural areas. Socio-economic classes of females were low because most females were unemployed. There was no significant correlation between DLQI score and Socio-economic status of the patients therefore; it seems that vitiligo similarly affects quality of life in different Socio-economic classes.
DLQI score interpretation can give the idea about the extent of quality of life affected in vitiligo patients [5–7]. DLQI score interpretation in the present study showed that 84% of the vitiligo patients have at least some effect on their quality of life while 47% have moderate to very large effect on their the quality of life. Earlier reports from the India have not studied DLQI interpretation in vitiligo patients.
Duration of disease at time of presentation to us was significantly more in females compared to males which may be because of their tendency to continue the treatment as compared to males who may be least bother and leave the treatment if there is no response.
Mean DLQI score in our study was 6.86 which is higher than that of some of previous studies [5–7] but lower than some other studies [20–22]. There was no statistically significant difference noted in mean DLQI score between male and female patients as reported by a previous study [7].
There was no statistically significant difference in mean DLQI scores between localized and generalized vitiligo patients, progressive and stable vitiligo patients. These findings may have occurred because of uneven distribution of patients in both groups.
Though there is no significant difference in mean DLQI score between married and unmarried vitiligo patients but very large effect on quality of life was seen significantly in unmarried patients. This may be because unmarried patients anticipate or face more difficulties in getting married. Past study reported that disease was usually not revealed to their partners by vitiligo patients at the time of marriage due to embarrassment or fear of rejection [4].
DLQI scores were not significantly correlated with BSA, age, duration of disease and Socio-economic class but education level had significant negative correlation with DLQI score. These findings suggest higher education can decrease the burden of vitiligo on quality of life or higher education empower patients with rational thinking about vitiligo. This relationship has not been reported in previous studies.
Conclusion
Although vitiligo is a cosmetic disease without any symptoms, but it carries a significant social stigma especially in Indian society. Data interpretation in this study indicates that vitiligo affects QOL in majority of vitiligo patients irrespective of extension of involvement (Generalized/localized vitiligo), so patients having localized vitiligo also has significant effect on quality of life. Hence patients of vitiligo require more aggressive and empathic attitude from a dermatologist to cure/improve this so called chronic cosmetic disease. The severity assessment of vitiligo as a disease should be based not only on the disease per se but also on its affect on quality of life.
*p-value determined by independent sample t- test
[1]. Kruger C, Schallreuter KU, Cumulative life course impairment in vitiligoCurr Probl Dermatol 2013 44:47-51. [Google Scholar]
[2]. Lerner AB, Vitiligo:J Dermatol 1959 32:285-310. [Google Scholar]
[3]. Handa S, Dogra S, Epidemiology of childhood vitiligo: a study of 625 patients from North IndiaPed Dermatol 2003 20:207-10. [Google Scholar]
[4]. Pahwa P, Mehta M, Khaitan BK, Sharma VK, Ramam M, The psychosocial impact of vitiligo in Indian patientsIndian J Dermatol Venereol Leprol 2013 79:679-85. [Google Scholar]
[5]. Kent G, Al Abadie M, Factors affecting responses on Dermatology Life Quality Index items among vitiligo sufferersClin Exp Dermatol 1996 21:330-33. [Google Scholar]
[6]. Belhadjali H, Amri M, Mecheri A, Doarika A, Khorchani H, Youssef M, Vitiligo and quality of life: A case-control studyAnn Dermatol Venereol 2007 134:233-36. [Google Scholar]
[7]. Ongenae K, Van Geel N, De Schepper S, Naeyaert JM, Effect of vitiligo on self-reported health-related quality of lifeBr J Dermatol 2005 152:1165-72. [Google Scholar]
[8]. Porter JR, Beuf AH, Lerner A, Nordlund J, Psychosocial effect of vitiligo: A comparison of vitiligo patients with “normal” control subjects, with psoriasis patients, and with patients with other pigmentary disordersJ Am Acad Dermatol 1986 15:220-24. [Google Scholar]
[9]. Mattoo SK, Handa S, Kaur I, Gupta N, Malhotra R, Psychiatric morbidity in vitiligo: Prevalence and correlates in IndiaJ Eur Acad Dermatol Venereol 2002 16:573-78. [Google Scholar]
[10]. Mattoo SK, Handa S, Kaur I, Gupta N, Malhotra R, Psychiatric morbidity in vitiligo and psoriasis: A comparative study from IndiaJ Dermatol 2001 28:424-32. [Google Scholar]
[11]. Ginsburg IH, The psychological impact of skin diseases:An overviewClin 1996 14:473-84. [Google Scholar]
[12]. Ctterill JA, Cunliffe WJ, Suicide in dermatological patientsBr J Dermatol 1997 137(2):24 [Google Scholar]
[13]. Basra MKA, Fenech R, Gatt RM, Salek MS, Finlay A.Y, The Dermatology Life Quality Index 1994-2007: A comprehensive review of validation data and clinical resultsBritish Journal of Dermatology 2008 159:997-1035. [Google Scholar]
[14]. Finlay AY, Khan GK, Dermatology Life Quality Index (DLQI): A simple practical measure for routine clinical useClinical and Experimental Dermatology 1994 19:210-16. [Google Scholar]
[15]. Lewis V L, Finlay A Y, Ten years experience of the Dermatology Life Quality Index (DLQI)J Investig Dermatol Symp Proc 2004 9(2):169-80. [Google Scholar]
[16]. Hongbo Y, Thomas CL, Harrison MA, Salek MS, Finlay AY, Translating the Science of Quality of Life into Practice: What Do Dermatology Life Quality Index Scores Mean?J Invest Dermatol 2005 (in press) [Google Scholar]
[17]. Kumar BPR, Dudala S R, Rao AR, Kuppuswamy’s socio-economic status scale –a revision of economic parameter for 2012International Journal of Research & development of Health 2013 1(1):2-4. [Google Scholar]
[18]. Lund C, Browder N, The estimation of areas of burnsSurg Gynecol obstet 1994 79:352-58. [Google Scholar]
[19]. Ongenae K, Van Geel N, De Schepper S, Naeyaert JM, Effect of vitiligo on self-reported health-related quality of lifeBr J Dermatol 2005 152:1165-72. [Google Scholar]
[20]. Aghaei S, Sodaifi M, Jafari P, Mazharinia N, Finlay AY, DLQI scores in vitiligo: Reliability and validity of the Persian versionBMC Dermatol 2004 4:8 [Google Scholar]
[21]. Dolatshahi M, Ghazi P, Feizy V, Hemami MR, Life quality assessment among patients with vitiligo: Comparison of married and single patients in IranIndian J Dermatol Venereol Leprol 2008 74:700 [Google Scholar]
[22]. Parsad D, Pandhi R, Dogra S, Kanwar AJ, Kumar B, Dermatology life quality index score in vitiligo and its impact on the treatment outcomeBr J Dermatol 2003 148:373-74. [Google Scholar]