Introduction: Orthognathic Le Fort 1 osteotomy, a surgical procedure performed to correct the aesthetics of mid face. Some of the complications of this surgery are hemorrhage, loss of sensation due to facial nerve damage, nasal septum deviation leading to crooked nose and snoring. Nasal septum deviation is the most common complication and one of the most noticeable complications that is developed during the Le Fort 1 osteotomy.
Aim: To ascertain that Submental Intubation in Orthognathic Le Fort 1 Osteotomy combats Nasal septum Deviation.
Materials and Methods: Medical records and clinical data of 32 patients who underwent orthognathic Le Fort 1 Osteotomy under submental orotracheal intubation were analyzed to understand if nasal septum deviation and other complications of Le Fort 1 Osteotomy occurred in such cases based on 6 parameters.
Results: No complications of nasal septum deviation or other complications that’s associated with orthognathic Le Fort 1 Osteotomy were found in the 32 cases that were analyzed.
Discussion: The surgeon needs to have a non-obtrusive nasal canal so as to determine the extent to which the nasal septum needs to be reduced so that it does not cause nasal septum deviation post the procedure. Submental oratracheal intubation provides the surgeon with an excellent view of the operating field, enough space for intra oral manipulation of the bone and septum for intra oral operation and control of dental occlusion.
Conclusion: Submental intubation is a better method of intubation during Le Fort 1 osteotomy as it does not cause nasal septum deviation or other associated complications.
Introduction
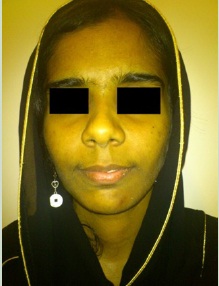
Orthognathic Le Fort 1 osteotomy is done for cosmetic reasons to reduce a gummy smile, to give a solution to maxillary skeletal deficit, to cure sleep apnea due to nasal septum defects [1,2]. A patient who underwent Orthognathic Le Fort 1 osteotomy under nasotracheal intubation for a gummy smile had to endure one of the main anatomical complication- the deviation of the nasal septum, which causes breathing problems and snoring [3,4] [Table/Fig-1,2and3]. This was identified and the nasal septum deviation was rectified [Table/Fig-4]. Post this occurrence of the complication this study was done to better understand the efficacy of using the submental orotracheal intubation method in orthognathic Le Fort 1 osteotomies to see if it will reduce the post surgical complications.

Post-operative – nasal septum deviation due to nasotracheal intubation

Submental orotracheal Intubation

Post nasal septum deviation correction
The Le Fort I osteotomy allows for correction primarily at the occlusal level affecting the upper lip position, nasal tip and alar base region, and the columella labial angle without altering the orbitozygomatic region [3,5].
Orthognathic Le Fot 1 Osteotomy Surgical Technique
Classic procedure of orthognathic Le Fort 1 osteotomy starts with a soft tissues incision bilaterally from the midline of the fornix above the central incisors to first molar region, involving mucosa, muscle and periosteum [1,6]. A subperiosteal dissection made with a periosteal elevator exposes the lateral wall of the maxilla, from the pterygomaxillary junction to the anterior nasal spine. The dissection continues toward the maxillary tuberosity and pterygoid plate, with an inferior angled fold behind the zygomatic buttress. The piriform aperture is exposed, and the mucoperiosteum is elevated along the piriform rim, the nasal floor and the lateral wall under the inferior turbinate, then reflected with a Periosteal elevator to expose the anterior floor of the nose [6]. The septopremaxillary ligament is transected as well as the transverse nasalis muscle to completely free the anterior nasal spine [6]. Careful management of the nasal mucosa, without perforations and cuts, minimizes blood loss and reduces postoperative discomfort [1,6,2]. Once the dissection is completed vertical and horizontal reference landmarks are scratched with a bur and a controlled fracture is performed and the preplanned and measured amount of bone is trimmed or bone grafts are placed in the case of advancement [6,3,2]. Before performing the osteotomy of the lateral wall of the nose, a periosteal elevator is inserted subperiosteally under the inferior turbinate, at the piriform aperture for 2 cm approximately, to protect the nasal mucosa [2]. The nasal septal region is exposed and based on the amount of horizontal and vertical plane movement of the mobilized bone the nasal septum is trimmed [3,5]. The mobilized bone is fixed with titanium screws and the soft tissue is closed and sutured [3,5,7].
Some of the immediate complications that were noticed in patients who had undergone orthognathic Le Fort 1 osteotomy were hemorrhage in the palatal region, temporary nasal airway block, swelling of the operation site. Once the inflammation had reduced one of the noticeable complications is the nasal septum deviation, this, most often occurred in cases where nasotracheal intubation was done [1,3,5,2].
When anesthesia is given nasotracheally the endotracheal tube obstructs the field of operation in the nasal cavity region which in turn hinders the proper reduction of the nasal septum and repositioning of the oro-cranial base, thus leading to a deviated nasal septum. The traditional alternative was tracheostomy which required a longer recuperating period post surgery. An alternate method was proposed by Altemir FM in 1986 this method was the submental orotracheal intubation method which was quick and efficient way of maintaining a clear nasal passage for the correct assessment and alignment of the Oro-cranial base and the exact amount of reduction that needed to be done on the nasal septum so that it did not cause any septal deviation post surgery [1].
Submental Orotracheal intubation technique
After a normal orotracheal intubation was performed with 7.5 or 8.5 mm diameter tube, a 2–cm skin incision was made in the paramedian region, about 1 cm from the lower mandibular margin and parallel to it on the midline [8]. Using a curved hemostat, a passage was created by blunt dissection near the lingual surface of the mandible. While the tongue was pushed backward, the tip of the hemostat was visible just below the mucosa of the floor of the mouth, anterior to Wharton’s duct papillae [9,8]. A mucosal incision was made parallel with the gingival margin on top of the tips. A passage for the tube was created from the mouth, through the mylohyoid muscle to the submental incision [8]. The orotracheal tube was secured in the mouth to avoid accidental extubation [10,11,9]. The end was grasped with the hemostat and withdrawn through the submental tunnel and connected with the orotracheal tube [8]. When capnography and lungs auscultation confirm the correct tracheal position of the tube, the tube is fixed at the submental level with 2–0 silk suture, in a similar fashion as a drainage tube [12,13]. At the end of the procedure, anesthesia is discontinued and the patient is extubated in the operating room [8,13].
The use of submental intubation has been modified over the years to suit the needs of the surgery that is to be performed [14–16]. Comparison of the risks and disadvantages of tracheostomy and submental intubation for the treatment of craniomaxillary trauma have been done widely [4,15–18]. The Submental orotracheal intubation technique has not been adequately discussed and studied, especially in relation to its advantages in Le Fort 1 Osteotomies and its post surgical complications.
Clinical Material and Methods
Medical records and clinical data of 32 patients who underwent orthognathic Le Fort 1 osteotomy under submental orotracheal intubation at the Oral and Maxillofacial surgery department of Sree Balaji Dental College and Hospital, Chennai, Tamil Nadu between April 2007 to December 2012 were reviewed. Orthognathic Le Fort 1 Osteotomies done under normal orotracheal or naso tracheal intubation methods were excluded from the study.
Assessment and analysis parameters and procedure
Post-operative swelling of the surgical site- Post-operative swelling was classified into two categories based on the patient’s complaints of being able to breathe via the nostrils. If they were able to breathe normally then it was considered normal or expected swelling which was required for healing and if the patient complained of inability to breath via the nostrils then it was considered excessive swelling.
Post-operative hemorrhage that required intervention: Case history was checked to see if any type of post surgical intervention by the surgeon was required for Post-operative hemorrhaging.
Any injury to the sublingual glands, Wharton’s duct or lingual nerve due to submental intubation technique, the Anatomical structures such as the Sublingual gland, Wharton’s duct and lingual nerve were tested and noted in the case history by the anesthetist post extubation.
Healing of the intra oral and submental scars was checked in each patient. The notes from day 2, the day of discharge and 3rd Post-operative visit were taken into account to understand the healing of the intra oral and submental incision region.
Post surgical nasal septal deviation was assessed from the surgeon’s notes on the 5th Post-operative visit along with the post surgical photograph was used.
Was snoring a complaint post surgery, case history was checked to see if the patient or close relatives complained of snoring as a new complaint during the post surgical visits.
Results
On analysis of the surgeon’s notes and the Post-operative photographs that were available it was noted that in the 32 cases there was no case of infection and that there was minimal scaring in the sub mental region. There was no nasal septum deviation in patients who chose to have anesthesia submentally or complaint of snoring.
Discussion
Orthognathic surgery of Le Fort 1 osteotomy of the maxilla is by far one of the more complex surgeries as the maxilla can be moved in all different planes and vectors which causes various anatomical landmarks that are present to also be adjusted as per the skeletal changes that are made in that region [6,3,5,2]. This leads to complications, of which one of the main anatomical complications that are noticed few days post surgery and after the swelling subsides is the nasal septum deviation [1,6]. When analyzed it is usually due to the lack of clear field of vision and good range of movement of the orocranial base during surgery due to the nasotracheal intubation [4,14–16]. This type of intubation causes discrepancy in calculation of the amount of nasal septum to be reduced thus was causing the nasal septum deviation [1,2].
Tracheostomy was first proposed in place of nasotracheal intubation in order to reduce the chance of nasal septum deviation, but that had higher chance of infection and extubation, and a longer period of healing post surgery. Not to mention the fact that Tracheostomy leaves a larger scar in a very prominent and visible region of the body [11,9,8].
An alternative to nasotracheal intubation and tracheostomy was proposed during the treatment of craniofacial traumas and cranial base approaches [4,14,16]. In this technique, called retromolar intubation, a semilunar osteotomy is made in the retromolar space [17]. The orotracheal tube is then placed in the retromolar area, lying below the occlusal plane [4]. This intubation technique offers an unobstructed intraoral surgical field with secure airway management, and maxillomandibular fixation can be performed without any impediments [1]. However bone anatomy must be destroyed to make space for the tube [4] and the procedure requires a mean of 25 minutes to perform [12]. Besides, evaluation of the restoration of an individual occlusion can be partially impaired by the presence of the tube in the oral vestibule [16,19].
The submental orotracheal intubation technique is the most simple and efficient method in which to intubate a patient with low morbidity, to reduce Nasal septal deviation in Le Fort 1 osteotomy cases [1,12] [Table/Fig-3]. This technique has low risk of damaging any anatomical structures such as the lingual nerve, the Wharton’s duct or the submaxillary glands. This method of intubation has the least complications as the surgical field is free of the endotracheal tubes. It also gives the surgeon who is performing this complex orthognathic Le Fort 1 osteotomy a clear field view, wide range of movement and access to anatomical structures that needs attention during the surgery [5,7,17,2].
Conclusion
After the review of 32 orthognathic Le Fort 1 oseotomies that were performed under submental orotracheal intubation by the Oral and Maxillo Facial Surgery Department of Balaji Dental College and Hospital, we can conclude that this method of intubation reduces the common complications that arise from nasotracheal intubation and that the nasal septum deviation can be combated successfully. More prospective studies with bigger sample size are needed before we can say submental orotracheal intubation is the most efficient method to avoid the nasal septum deviation.
[1]. Kramer FJ, Intra- and perioperative complications of the LeFort I osteotomy: a prospective evaluation of 1000 patientsJ Craniofac Surg 2004 15:971-7.[PubMed] [Google Scholar]
[2]. Antonio Cortese (2012). Le Fort I Osteotomy for Maxillary Repositioning and Distraction Techniques, The Role of Osteotomy in the Correction of Congenital and Acquired Disorders of the Skeleton, Prof. James Waddell (Ed.), ISBN: 978-953-51-0495-7, InTech, Available from: http://www.intechopen.com/books/the-role-ofosteotomy-in-the-correction-of-congenital-and-acquired-disorders-of-the-skeleton/le-fort-i-osteotomy-formaxillary-repositioning-and-distraction [Google Scholar]
[3]. Lehotay Erbe M, Göde M, Wigand U, Neukam ME, FW, (2001). Nasal airway changes after Le Fort I–impaction and advancement: anatomical and functional findingsInt J Oral Maxillofac Surg 2011 30(2):123-9.[PubMed] [Google Scholar]
[4]. Haarmann A, Budihardja, AS. Wolff, KD. Wangerin, K. (2009). Changes in acoustic airway profiles and nasal airway resistance after Le Fort I osteotomy and functional rhinosurgery: a prospective studyInt J Oral Maxillofac Surg 2009 38(4):321-5. [Google Scholar]
[5]. Altemir FH, The submental route for endotracheal intubationJ Maxillofac. Surg 1986 14:64-5.[PubMed] [Google Scholar]
[6]. Acebal-Bianco F, Vuylsteke PL, Mommaerts MY, (2000). Perioperative complicationsin corrective facial orthopedic surgery: A 5-year retrospective studyJ OralMaxillofac Surg Jul2000 58(7):754-60.[PubMed] [Google Scholar]
[7]. Ghoreishian M, Gheisari R, (2009). The effect of maxillary multidirectional movement on nasal respirationJ Oral Maxillofac Surg 2009 67(10):2283-6. [Google Scholar]
[8]. Biglioli F, Mortini P, Goisis M, Bardazzi A, Boari N, Submental orotracheal intubation: An alternative to tracheotomy in transfacial cranial base surgerySkull Base 2003 13:189-95.[PMC free article] [PubMed] [Google Scholar]
[9]. Johnson TR, Submental versus tracheostomyBr J Anaesth 2002 89:344-5.[PubMed] [Google Scholar]
[10]. Schade K, Borzotta A, Michaels A, Intracranial malposition of nasopharyngeal airwayJ Trauma 2000 49:967-8.[PubMed] [Google Scholar]
[11]. Amin M, Dill-Russel P, Manisali M, Lee R, Sinton I, Facial fractures and submental intubationAnaesthesia 2002 57:1195-212.[PubMed] [Google Scholar]
[12]. Arya VK, Kumar A, Makkar SS, Sharma RK, Retrograde submental intubation by pharyngeal loop technique in a patient with faciomaxillary trauma and restricted mouth openingAnesth Analg 2005 100:534-7.[PubMed] [Google Scholar]
[13]. Davis C, Submental intubation in complex craniomaxillofacial traumaANZ J Surg 2004 74:379-81.[PubMed] [Google Scholar]
[14]. Paetkau Donald J, Submental orotracheal intubation for maxillofacial surgeryAnesthesiology 2000 92:912[PubMed] [Google Scholar]
[15]. Drolet P, Girard M, Poirier J, Grenier Y, Facilitating submental endotracheal intubation with an endotracheal tube exchangerAnesth Analg 2000 90:222-3.[PubMed] [Google Scholar]
[16]. Altemir FH, Montero SH, The submental route revisited using the laryngeal mask airway: A technical noteJ Craniomaxillofac Surg 2000 28:343-4.[PubMed] [Google Scholar]
[17]. MacInnis E, Baig M, A modified submental approach for oral endotracheal intubationInt J Oral Maxillofacsurg 1999 28:344-6.[PubMed] [Google Scholar]
[18]. Bale DR, Clark M, Jefferson P, Stewart T, Improved submental intubationAnaesthesia 2003 58:189[PubMed] [Google Scholar]
[19]. Malhotra SK, Malhotra N, Sharma RK, Submental intubation: Another problem and its solutionAnesth Analg 2002 95:1127[PubMed] [Google Scholar]