Recurrent Angiofibroma of Ethmoid Region – A Rare Variant
M. Sudhakara Rao1, Chintamaneni Raja Lakshmi2, P.E Sonylal3, V. Kalyan Chakravarthy4, P.S.N Murthy5
1 Associate Professor, Department of Otorhinolaryngology and Head and Neck Surgery, Dr Pinnamaneni Siddhartha Institute of Medical Sciences and Research Foundation, Chinnaoutpalli,Gannavaram Mandal, Krishna District, Andhra Pradesh, India.
2 Assistant Professor, Department of Oral Medicine and Radiology, Drs Sudha and Nageswara Rao Siddhartha Institute of Dental Sciences, Chinnaoutpalli, Gannavaram Mandal, Krishna District, Andhra Pradesh, India.
3 Associate Professor, Department of Neurosurgery, Associate Professor, Dr Pinnamaneni Siddhartha Institute of Medical Sciences and Research Foundation, Chinnaoutpalli, Gannavaram Mandal, Krishna District, Andhra Pradesh, India.
4 Associate Professor, Department of General Pathology, Dr Pinnamaneni Siddhartha Institute of Medical Sciences and Research Foundation, Chinnaoutpalli, Gannavaram Mandal, Krishna District, Andhra Pradesh, India.
5 Professor & Head of the Department, Department of Otorhinolaryngology and Head and Neck Surgery, Dr Pinnamaneni Siddhartha Institute of Medical Sciences and Research Foundation, Chinnaoutpalli, Gannavaram Mandal, Krishna District, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. M. Sudhakara Rao, MS ENT Associate Professor, Department of Otorhinolaryngology and Head and Neck Surgery, Dr Pinnamaneni Siddhartha Institute of Medical Sciences and Research Foundation, Chinnaoutpalli, Gannavaram Mandal, Krishna District, Andhra Pradesh-521286, India.
Phone: 949065800
E-mail: sudhakarentvijayawada@yahoo.com
The common variant of angiofibromas of head and neck region is juvenile nasopharyngeal angiofibroma (JNA). However extranasopharyngeal angiofibromas (ENAF) occurs very rarely at any age in either sex, and they differ from classical JNA in incidence, clinical and radiological presentation. They form the differential diagnosis for any mass nose or nasal polyp. We present a case of recurrent angiofibroma of ethmoid region presented with recurrent lesion with bilateral proptosis and bossing of forehead. MRI showed involvement of bilateral nasal cavities, ethmoids and frontal sinuses with erosions of ethmoid roof and posterior table of frontal sinuses. Entire mass was excised by craniofacial resection which was histopathologically confirmed as Angiofibroma.
Extra nasopharyngeal angiofibroma (ENAF), Juvenile Nasopharyngeal Angiofibromas (JNA), frontoethmoid region recurrent craniofacial resection
Case Report
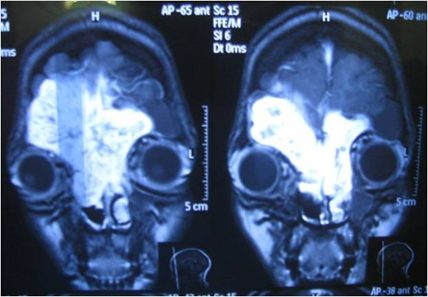
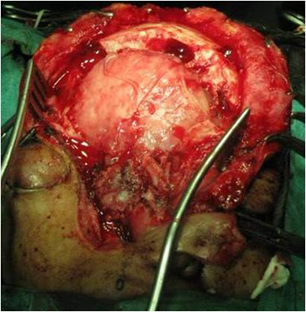
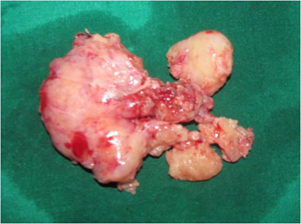
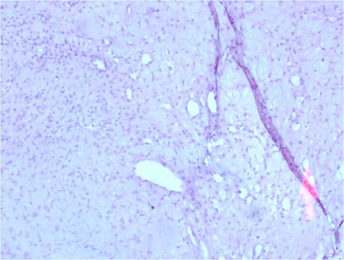
A 27-year-old female presented with frontal bossing and widening of intercanthal distance with bilateral extra-axial proptosis [Table/Fig-1]. History revealed that she was operated about eight years back for right medial canthal swelling, which was confirmed histopathologically as angiofibroma. At present on clinical examination lateral rhinotomy scar was noticed and nasal cavity was filled with mass on either side, with nasal patency only on left side. MRI revealed contrast enhancement of the lesion involving bilateral nasal cavities, ethmoids, frontal sinuses eroding posterior table of frontal sinus and ethmoid roof [Table/Fig-2]. Planned for craniofacial resection in association with neurosurgeon. Previous lateral rhinotomy scar was reopened and the incision extended onto the forehead and scalp upto coronal suture. Thinned out anterior table of frontal sinus was elevated on either side as a single unit. Similarly nasal and ethmoid tumour was exposed by tilting the nasal pyramid onto the opposite side by fracturing the opposite nasal bone vertically [Table/Fig-3]. Dissection started from frontal region and tumour was carefully separated from anterior fossa dura especially in midline where it was firmly adherent. Dissection was proceeded down separating the tumour from cribriform plate where the bone was partially dehiscent, and then entire tumour was removed from both nasal cavities and ethmoids [Table/Fig-4]. Frontal sinus area was obliterated with fat, inferiorly supported with fascia-lata and covered with the free bony flap of anterior table of frontal sinus. Recovery and immediate postoperative period were uneventful. There was no CSF leak. Excised specimen was subjected for histopathological examination which revealed fascicles of fibrous tissue with round, oval to spindle shaped cells with vesicular nucleus, there are hypocellular areas and myxoid areas. Tissue is interspersed with endothelial lined vascular spaces suggestive of angiofibroma [Table/Fig-5].
Widening of intercanthal distance with bilateral extra-axial proptosis with extended lateral rhinotomy scar.

Pre operative MRI revealed enhanced tumour mass involving bilateral nasal cavities encroaching ethmoid and frontal sinuses bilaterally.
Tumour was exposed by tilting the nasal pyramid onto the opposite side
Excisional specimen of recurrent lesion
Histopathological picture demonstrating fascicles of fibrous tissue with ovoid to spindle shaped cells interspersed with endothelial lined vascular spaces suggestive of angiofibroma
Patient was followed at monthly intervals for 18 months with nasal endoscopy on each visit and follow-up. MRI scan taken at intervals of 3 months and 18 months post-operative period. Recent MRI revealed no recurrence. Patient was advised strict regular long term follow-up [Table/Fig-6].

Discussion
Angiofibromas in head and neck region commonly arises from nasopharynx almost exclusively in adolescent boys (JNA) and they account for 0.05–0.5% of all head and neck neoplasms [1] Occasional case reports are found regarding extranasopharyngeal angiofibromas from the sites like maxillary and ethmoid sinuses, nasal septum and sphenoid sinus [2]. In fact, these rare benign neoplasms are characterized by a different biological history and clinical features with respect to nasophayngeal tumours and, for these reasons, they should be regarded as a separate clinical entity. Compared to nasopharyngeal angiofibromas, ENAF patients affected are older, females can also be involved, symptoms develop more quickly, and hypervascularity is less common [3]. In the present illustrated case patient is 27-year-old female. JNA usually presents with frank unprovoked epistaxis, whereas our patient has no such history both initially and on recurrence which is similar to other case reports of extranasopharyngeal angiofibromas (ENAF). Diagnosis of JNA is by the classical site and growth pattern from CT PNS and biopsy is avoided for fear of uncontrollable bleeding, whereas clinical diagnosis of ENAF is not straight forward and that will be a differential diagnosis of either nasal polyp or mass nose and enough care should be taken when attempting for biopsy of such lesions [4]. Infact most of the ENAFs are diagnosed postoperatively when the excised nasal masses are subjected to histopathology. Our case has presented initially with mass above the right medial canthus which was histopathology confirmed as angiofibroma.
Treatment of choice for JNA is surgical excision and the approach depends on the stage and direction of spread of the tumour, certainly with preoperative embolization.
There was a recent trend of endoscopic resection of early JNA which reduces morbidity to a great extent [5,6]. None of the case reports of ENAFs suggested preoperative embolization. We dealt the recurrent pathology with lateral rhinotomy incision extended onto forehead for combined craniofacial resection without preoperative embolization. We have not experienced a typical peroperative bleeding of JNA in the surgical procedure may be because of excess fibrous component of the tumour and this finding is similar to some of the other case reports about ENAFs. No reports found about recurrence of ENAFs after initial surgery, whereas studies about recurrent JNA revealed 39.2% recurrence after initial surgery and the predictors of recurrence were age at diagnosis and stage of the tumour [7]. Though various modalities for the treatment of angiofibromas include surgery, hormonal therapy, radiation, and systemic chemotherapy. However, surgery remains the primary course of treatment [8]. The present case is an exclusive report of recurrent ENAF and its management. The recurrence may be from microscopic remnants at initial surgery and improper followup for many years, later she presented with an extensive recurrence. After the surgical treatment of recurrent lesion regular follow up is being done with nasal endoscopies and MRI was done twice which revealed no evidence of recurrence till date.
Conclusion
ENAFs should be considered in differential diagnosis for evaluation of mass nose in either sex at any age. Bleeding from the nose may be a rare finding. Surgical options depends on the site and size of the tumour and by surgeon’s preference. Team approach may be useful especially when it encroaches or invades cranial cavity. Needs long term follow up to rule out recurrence.
[1]. Windfuhr JP, Remmert S, Extranaso pharyngeal angiofibroma: etiology, incidence and managementActa otolaryngo 2004 1248:880-9. [Google Scholar]
[2]. Lerra S, Nazir T, Khan N, A case of extranasopharyngeal angiofibroma of the ethmoid sinus: a distinct clinical entity at an unusual siteEar Nose Throat J 2012 912:E15-7. [Google Scholar]
[3]. Akbas Y, Anadolu Y, Extranasopharyngeal angiofibroma of the head and neck in womenAm J Otolaryngo 2003 24(4):13-6. [Google Scholar]
[4]. Durko M, Murlewska A, Angiofibroma of the nasal cavity and anterior ethmoid cells – problems in differential diagnosisOtolaryngol pol 2007 6(15):736-9. [Google Scholar]
[5]. Wormald PJ, Van A, Hasselt Endoscopic removal of juvenile angiofibromasOtolaryngol Head Neck Surg 2003 1296:684-91. [Google Scholar]
[6]. Hackman T, Snyderman CH, Juvenile R Carrau, Nasopharyngeal Angiofibroma: The expanded endoscopic approachAm J Rhinol Allergy 2009 231:95-9. [Google Scholar]
[7]. Sun XC, Wang DH, Yu HP, Wang F, Analysis of risk factors associated with recurrence of nasopharyngeal angiofibromaJ Otolaryngol Head Neck Surg 2010 391:56-61. [Google Scholar]
[8]. Ravishankar M, Amit G, Juhi B, Mahesh K, Virupaksha S, Sachin C, Suresh An, Unusual Location of Juvenile Angiofibroma: A Case Report and Review of the LiteratureCase Reports in Otolaryngology 2013 Article ID 175326 [Google Scholar]