A Rare Presentation of Gallbladder Carcinoma Metastasis
Sheela Chaudhari1, Deepa Hatwal2, Pawan Bhat3
1Associate Professor, Department of Pathology,Government Medical College (VCSGGMC&RI) Srikot,Srinagar Pauri Garhwal, Uttarakhand, India.
2Associate Professor, Department of Pathology,Government Medical College (VCSGGMC&RI) Srikot,Srinagar Pauri Garhwal, Uttarakhand, India.
3Associate Professor, Department of Pathology,Government Medical College (VCSGGMC&RI) Srikot,Srinagar Pauri Garhwal, Uttarakhand, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr Sheela Chaudhari, Associate Professor, Department of Pathology, Government Medical College (VCSGGMC&RI) Srikot, Srinagar Pauri Garhwal, Uttarakhand, India.
Phone: 9412085721,
E-mail: drcnsuk@yahoo.com
Gallbladder carcinoma is the 5th most common gastrointestinal cancer. Gallbladder cancer preferentially metastasizes to regional lymph nodes and liver parenchyma. Bone metastases from gallbladder carcinoma are rare presentation. We report a case of gallbladder carcinoma with solitary metastasis to femur bone with surrounding soft tissue involvement, mimicking as soft tissue tumour involving bone.
Biliary tree, Immunohistochemistry, Skeletal metastasis
Case Report
A 55-year-old male presented in orthopaedic department with pain in left hip joint radiating down up to the knee for last three months. There was no history of weight loss, anorexia & jaundice. History revealed treatment taken three months back for inflammatory lesion after confirmed by FNAC in some other hospital. General examination revealed no significant finding at the primary site. X-ray of the left hip joint was done which showed an osteolytic lesion involving greater trochanter [Table/Fig-1] . CT scan of left hip showed a destructive bone mass of 5×5cms with large soft tissue component breaking the cortex of bone in the greater trochanter and neck of the femur. A diagnosis of bone tumour was made by surgeons. Wide excision of the growth was done and tissue was sent to our pathology department for histopathological examination.
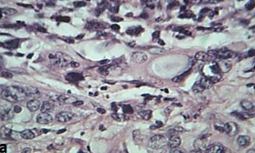
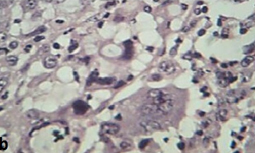
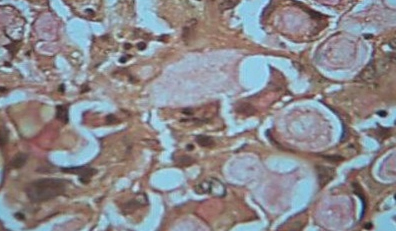
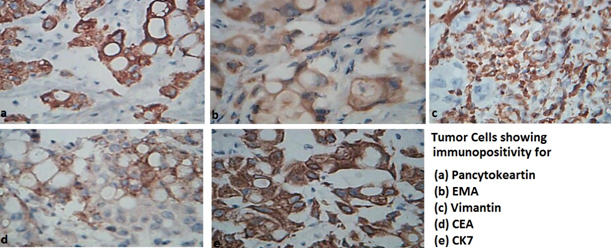
We received four irregular pieces of soft tissue mass. External surface was lobulated and cut section showed grey white area of necrosis and haemorrhage. Histopathological examination of H&E stained slides revealed cohesive sheets of epithelial cells exhibiting glandular differentiation with several signet ring forms. The nuclei show a moderate to marked degree of pleomorphism [Table/Fig-2a ,2b] . Mucicarmine stains show strong luminal and intracytoplasmic positivity [Table/Fig-3] . The tumour cell showed strong immunoreactivity for- Pancytokeratin, EMA, Vimentin, CEA, CK7 [Table/Fig-4] and was immunonegative for CK20, S100 protein, TTF-1, SATB2. Based on the histopathological and immunohistochemical findings a diagnosis of Metastatic adenocarcinoma, consistent with Metastatic adenocarcinoma from the Pancreaticobiliary system was made. Patient was evaluated further and a CT scan of whole abdomen was done. This revealed presence of a large mass in the gallbladder fossa with no identifiable gallbladder [Table/Fig-5] . Laparoscopic biopsy of the mass confirmed the primary site of cancer in gallbladder. Based on this report a diagnosis of carcinoma gallbladder was made and patient was referred to cancer department for the further evaluation and treatment. Patient was kept on chemotherapy. Later he developed metastases in other sites and died in eight months.
X-ray of hip joint showing osteolytic lesion in greater trochenter

Tumor cells showing glandular pattern (H&E 40x)
H&E stain slide showing signet cell and tumor giant cells
Tumor cells showing positivity for Mucicarmine
Tumor cells showing immunopositivity
CT scan showing mass in gallbladder fossa

Discussion
Gallbladder cancer is a common biliary tree malignancy presenting in advanced stage of the disease [1] . It is difficult to diagnose gallbladder carcinoma in early stage because symptoms are similar to those of benign disease. They are mostly found incidentally on removal of gallbladder for benign disease like chronic cholecystitis & gallstone [2] . Gallbladder malignancy commonly spread by direct extension to liver and adjacent organs of gastrointestinal tract, followed by regional lymph node. Metastases from Gallbladder carcinoma have been reported from almost every organ of the body including skin, orbit, breast but only a few isolated cases of distant metastases to bone have been reported in live patient [3-5] . However one series described high incidence of distant metastases in autopsy patients [6] . The case described here is unusual in that, femur bone metastastatic mass was the only presenting complain of the patient that lead to the diagnosis of asymptomatic gallbladder carcinoma. Our patient was not having any complain regarding the primary site of cancer which makes it a rare presentation of Gallbladder carcinoma. Only one similar case of femur metastases has been reported in the past by Kohli et al., [7] . In our case bony metastases was osteolytic which is commonly seen in gallbladder bone metastases. Some of the literature do show the presence of osteoblastic metastases [1,3] . Bone metastases from gallbladder cancer is rare at the time of diagnosis. There are only few case reports of gallbladder carcinoma with bone as only metastatic site [3-5] . These cancers commonly spread to the surrounding structures. Presentation of gallbladder cancer metastases to bone without the noticeable symptoms of primary site is extremely rare. Because of this reason bone scanning is not done routinely in carcinoma gallbladder. But as seen in our case report and in Kohli et al.,[7] case, it was the only present symptom. Present case report and reports of some others [3-5] shows bone as the only distant metastatic site. This indicates toward the need of CT and bone scanning in accurately staging gallbladder carcinoma.
Keeping this in mind we conclude that though bone is the rare site of gallbladder metastases but one should keep vigilance for bony metastases in case there is any symptoms in order to improve the survival period.
[1]. N Kalra, S Suri, R Gupta, MDCT in the staging of gallbladder carcinoma.AJR Am J Roentgenol. 2006 186:758-62.Doi:10.2214/AJR.04.1342.PMid: 16498103. [Google Scholar]
[2]. SY Kwon, HL Chang, A clinicopathological study of unsuspected carcinoma of gallbladderJ Korean Med Sci 1997 12:519-22. [Google Scholar]
[3]. A Kumar, K Bhargava S, L Upreti, J Kumar, Disseminated osteoblastic skeletal metastases from carcinoma of gallbladder - a case reportIndian J Radiol Imaging 2003 13:37-9.[serial online]. [Google Scholar]
[4]. S Singh, R Bhojwani, S Singh, A Bhatnagar, RK Saran, AK Agarwal, Skeletal Metastasis in Gallbladder CancerHPB (Oxford). 2007 9(1):71-2. [Google Scholar]
[5]. Prakash Mahesh, Aiyappan Senthil Kumar, Kumar Ajay, Sreenivasan Radhika, Solitary skeletal metastasis in carcinoma gallbladder: two case reportsCancer Imaging. 2010 10:121-3. [Google Scholar]
[6]. HU Sons, F Borchard, BS Joel, Carcinoma of the gallbladder. Autopsy finding in 287 cases and review of the literature.Journal of Surgical oncology 1985 28:199-206. [Google Scholar]
[7]. A Kohli, RS Chib, BK Parihar, Secondary involvement of femur in carcinoma of gallbladder.Indian Journal of Cancer. 1994 31(4):257-9. [Google Scholar]