Chordoma Cutis – A Diagnosis not to be Missed
Nadeem Tanveer1, Kiran Mishra2
1 Assistant Professor, Department of Pathology, University College of Medical Sciences, Delhi, India.
2 Professor, Department of Pathology, University College of Medical Sciences, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr.Nadeem Tanveer, Assistant Professor, Department of Pathology, University College of Medical Sciences, Delhi-110095, India.
E-mail: ntobh104@yahoo.co.in
Chordomas are rare midline tumors of the bone usually arising from sacrum, skull bones and spine, close to neuraxis. However an extensive involvement of the soft tissues can simulate a soft tissue subcutaneous tumour of the gluteal region –a presentation called chordoma cutis.
Our patient presented with a gluteal mass and a trucut biopsy was done suspecting a soft tissue tumour. The hematoxylin and eosin stained section of the biopsy closely simulated a lipomatous tumour. However, on closer inspection the clear cells were found to have very fine vacuolations.The usual myxoid background and characteristic physaliferous cells seen in chordomas were not seen. Still a differential of chordoma was entertained in view of the site and age of the patient. Immunohistochemistry for cytokeratin and S-100 was performed and both were unambiguously positive. On literature search, we came across a soft tissue tumour called parachordoma which mimics chordoma both morphologically and immunohistochemically and has also been reported in the gluteal region. An MRI was performed which showed the tumour to be arising from the sacrum and secondarily involving the gluteal soft tissues.
This case highlights the importance of considering chordoma in the differential diagnosis of gluteal masses with clear cell morphology even in the absence of physaliferous cells and myxoid background before signing them out as lipomatous tumours.
Chordoma, Clear cell tumour, Gluteal mass
Case Report
A 65-year-old male patient presented with a gluteal swelling slowly increasing in size over the last six months. Suspecting a soft tissue tumour a trucut biopsy was performed.
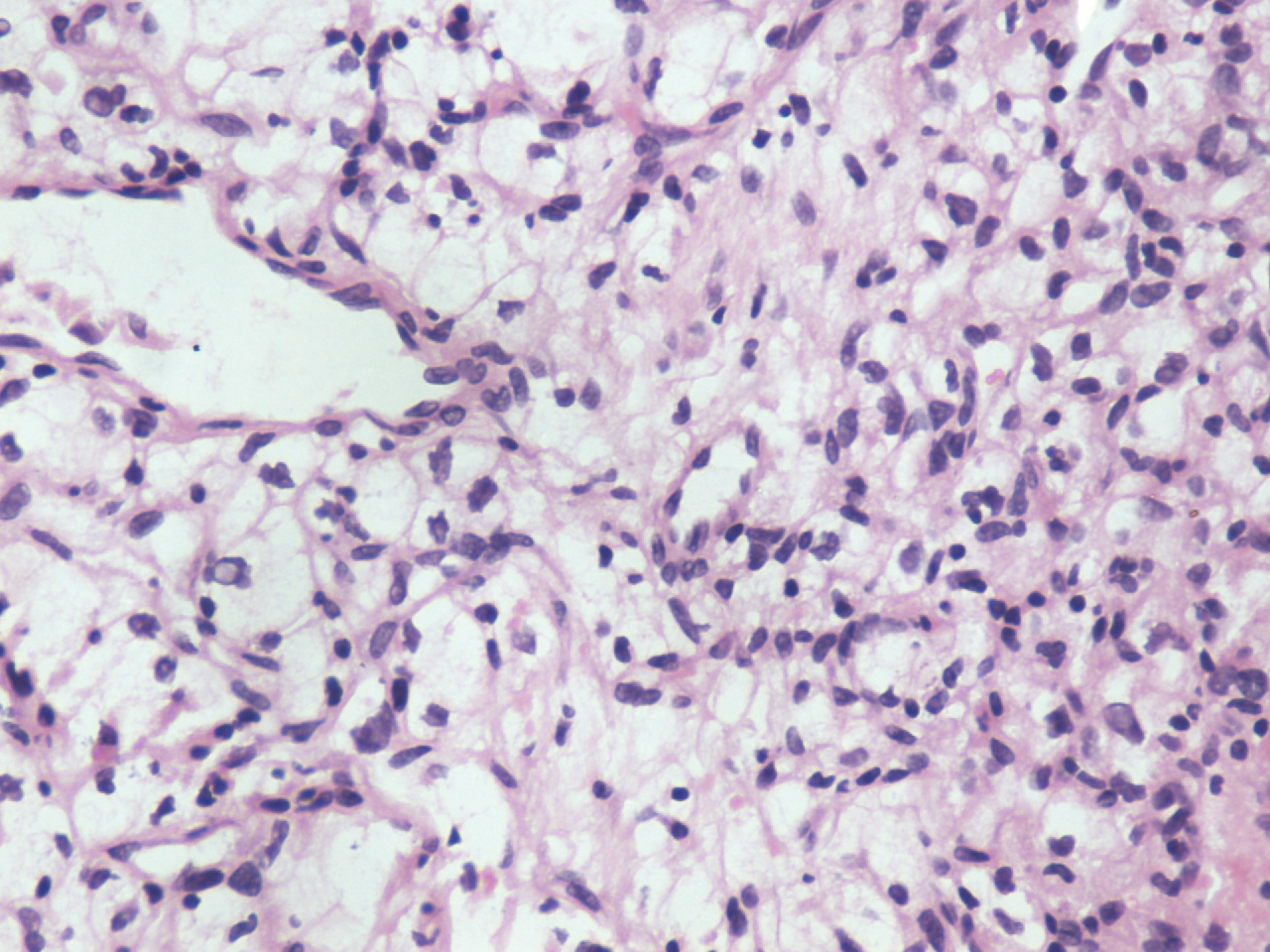
The trucut biopsy showed a tumour composed of clear cells with thin fibrous septae separating the tumour lobules. The tumour cells had vacuolated cytoplasm.There was minimal nuclear pleomorphism and no necrosis or mitosis was observed. No physaliferous cells or mucinous background were identified [Table/Fig-1]. Keeping the site of the tumour in mind, the differential diagnoses included lipomatous tumor, chordoma, parachordoma and metastatic renal cell carcinoma.
Hematoxylin and Eosin section(200 X):The tumour is composed of clear cells with only mild nuclear hyperchromasia.No physaliferous cells or mucoid background is seen
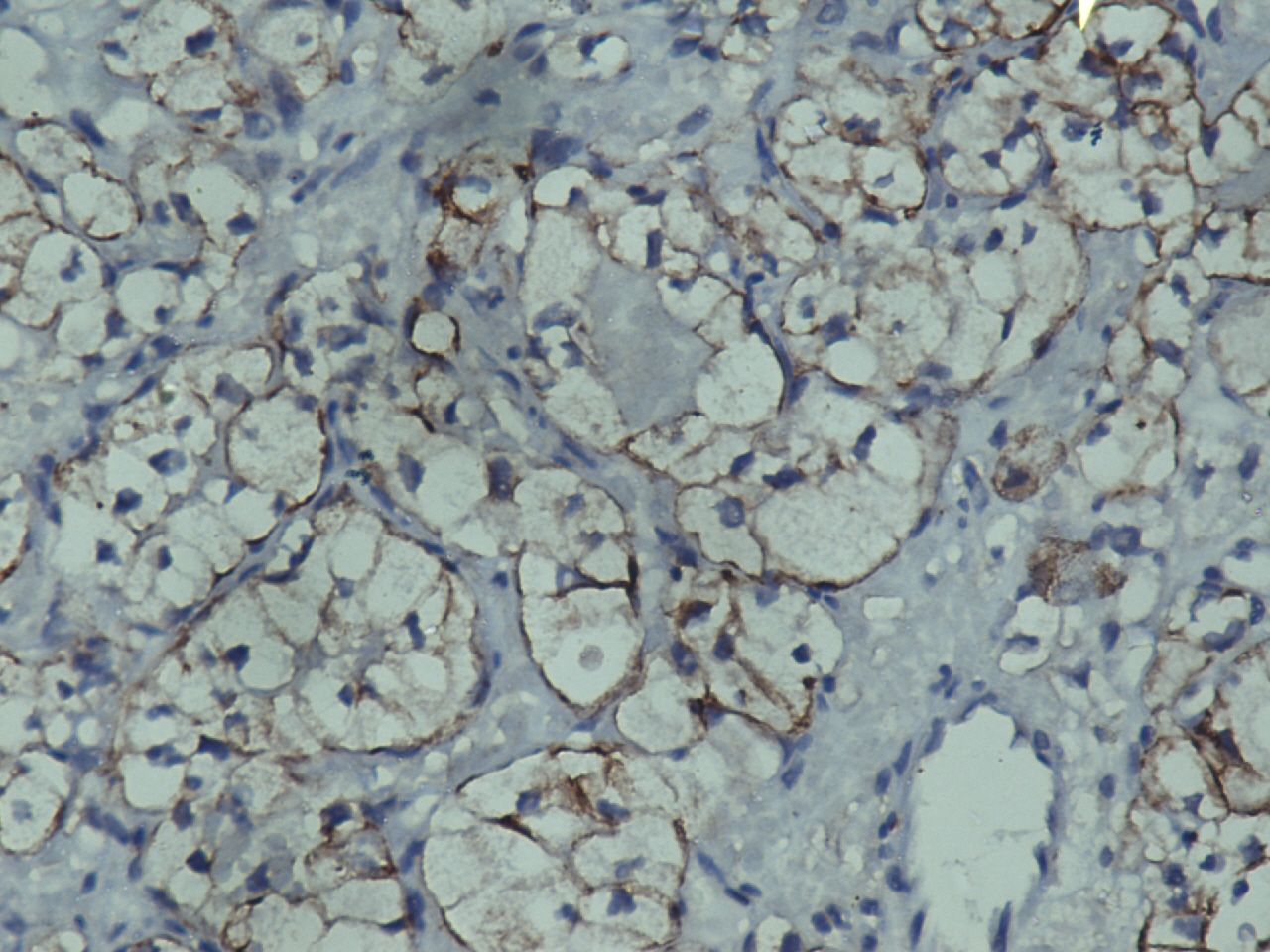
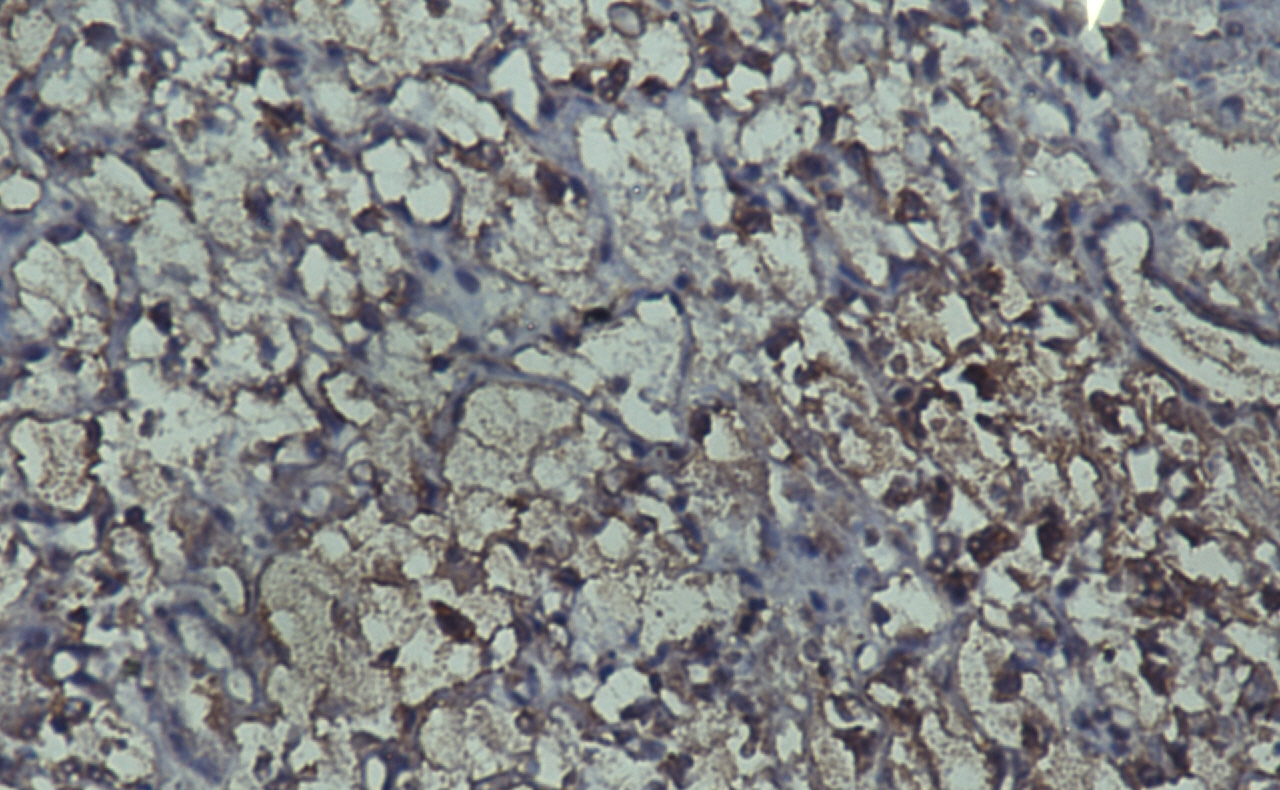
An immunohistochemical panel comprising of pan cytokeratin and S-100 was put up. Both cytokeratin and S-100 were positive [Table/Fig-2,3], hence only two differential diagnoses were left in contention-chordoma and parachordoma. An MRI scan was then performed which clearly showed that the tumour was arising from the sacrum and infiltrating the soft tissues and reaching the gluteal region [Table/Fig-4].
Immunohistochemistry for pan cytokeratin (200 X): Tumour cells show membranous positivity for cytokeratin
Immunohistochemistry for S-100 (200X): Tumour cells show both nuclear and cytoplasmic positivity for S-100
MRI: On T1 weighted image, the tumour is homogenous low intensity lesion arising from the sacrum and infiltrating the surrounding soft tissues reaching upto the gluteal region

This ruled out the possibility of parachordoma and a diagnosis of chordoma was made.
Discussion
Chordomas are rare tumours usually restricted to the midline. As many as 50 % of the chordomas arise in the sacrococcygeal region [1].
The usual histologic hallmarks of chordoma are physaliferous cells and a metachromatic mucinous or myxoid stroma The tumour cells are arranged in cords, nests and trabeculae embedded in the stroma [1]. However, due to variability in sampling, these characteristic features may be absent in trucut biopsies. A high index of suspicion is warranted to not to miss out on this diagnosis in such cases. An inadequate clinical history and lack of radiological investigations done prior to the trucut biopsy also add to the confusion.
In the gluteal location therefore the differential diagnoses of a subcutaneous tumour with clear cell morphology would include lipomatous tumor chordoma, parachordoma and metastatic renal cell carcinoma.
Tumours resembling chordoma on morphology and immunohistochemistry have been described in soft tissues and given the name parachordoma. Though there is some evidence that it may be linked to soft tissue myoepithelioma, its histogenesis still remains an enigma. Interestingly a case of parachordoma of the gluteal region has also been reported [2]. In view of the morphological and immunohistochemical overlap between chordoma and parachordoma, it becomes important to rule out a metastatic chordoma by imaging techniques before a diagnosis of parachordoma of soft tissue is made.
In cases where the physaliferous cells and myxoid or mucoid background are not evident, metastatic clear cell carcinoma kidney and lipomatous tumors also come in the differential diagnosis. However, co-expression of S-100 and cytokeratin would rule out both of them. Other markers which are reported to be positive in chordoma include brachyury, glial fibrillary acid protein, CK8,CK19 and 5’-nucleotidase [3].
Su WP et al., published the largest series of chordoma involving the subcutaneous tissues. They also coined the term chordoma cutis for this rare presentation of chordoma [4].
As in our case chordoma cutis can also be the first sign of chordoma [5]. All the other reports of chordoma cutis are metastasis from chordoma at different sites or tumor recurrences [6–8]. All these case reports have been published in dermatology or dermatopathology journals, hence there is a need for creating awareness about this entity amongst the general surgical pathologists.
This case highlights the importance of keeping chordoma cutis in the differential diagnosis of suspected soft tissue tumours of the gluteal region with clear cell morphology even when the classical features like physaliferous cells and mucoid background are missing.
[1]. Kaiser TE, Pritchard DJ, Unni KK, Clinicopathologic study of sacrococcygeal chordomaCancer 1984 54:2574-78. [Google Scholar]
[2]. Hirokawa M, Manabe T, Sugihara K, Parachordoma of the buttock: an immunohistochemical case study and reviewJpn J Clin Oncol 1994 24(6):336-9. [Google Scholar]
[3]. Rutherford GS, Davies AG, Chordomas–ultrastructure and immunohistochemistry. A report based on the examination of six casesHistopathology 1987 11:775-87. [Google Scholar]
[4]. Su WP, Louback JB, Gagne EJ, Scheithauer BW, Chordoma cutis: a report of nineteen patients with cutaneous involvement of chordomaJ Am Acad Dermatol 1993 29(1):63-6. [Google Scholar]
[5]. Boneschi V, Tourlaki A, Parafioriti A, Berti E, Brambati M, Brambilla L, Chordoma cutisEur J Dermatol 2003 13(6):593-5. [Google Scholar]
[6]. Dubroff RP, Maki RG, Busam KJ, Sachs DL, Bluish papule in a middle-aged manArch Dermatol 2005 141(12):1595-1600. [Google Scholar]
[7]. Rubin AI, Bagel J, Niedt G, Chordoma cutisJ Am Acad Dermatol 2005 52(5)(Suppl 1):S105-8. [Google Scholar]
[8]. Persichetti G, Walling HW, Rosen L, Cronin T, Ceilley RI, Chordoma cutisDermatologic Surgery 2007 33:1520-24. [Google Scholar]