Gastrointestinal Stromal Tumour of Small Intestine Presenting as a Mesenteric Mass
Kishor H Suryawanshi1, Tushar B Patil2, Rajshri P Damle3, N.V Dravid4, Akshay Surana5
1Assistant Professor, Department of Pathology, A.C.P.M. Medical College, Dhule, Maharashtra, India.
2Assistant Professor, Department of Surgery, A.C.P.M. Medical College, Dhule, Maharashtra, India.
3Assistant Professor, Department of Pathology, A.C.P.M. Medical College, Dhule, Maharashtra, India.
4Professor & Head, Department of Pathology, A.C.P.M. Medical College, Dhule, Maharashtra, India.
5Assistant Lecturer, Department of Pathology, A.C.P.M. Medical College, Dhule, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kishor H. Suryawanshi, Assistant Professor, Department of Pathology, A.C.P.M. Medical College, Dhule, Maharashtra, India.
Phone: 09403424244,
E-mail: ompathologylab@gmail.com
Gastrointestinal stromal tumors (GISTs) are uncommon tumors; accounts for 0.1% to 3% of all gastrointestinal neoplasm. Most common site of involvement is stomach (60-70 %), small intestine (20-30 %) and rarely at extra-gastrointestinal sites like omentum and mesentery called as extra-gastrointestinal stromal tumor (EGIST). Diagnosis is based on characteristic histological findings and expression of transmembrane receptor tyrosine kinase protein (CD 117) derived from activated c-kit gene.
Herein, we report a case of GIST of small intestine presented as mesenteric mass in a 35- year-old female and discuss review of literature.
Bowel obstruction, CD117, Extra-gastrointestinal, Small intestine
Case Report
A 35-year-old female presented with complaints of intermittent diffuse abdominal pain since 5-6 months gradually increasing in intensity from last four to five days, mild distension of abdomen since 5-6 days and two episodes of vomiting for one day. Abdominal distension was sudden on onset which started in lower abdomen. There was no history of fever, hematemesis or malaena. Past and family history was insignificant. On general examination patient was vitally stable with mild anaemia. Local examination revealed mild tenderness in right lower abdomen. Other systemic examination revealed no significant abnormality. Routine laboratory investigations were within normal limits except for anaemia and mild neutrophilic leukocytosis. Ultrasonography examination revealed mass lesion with solid and cystic areas in the mesentery attached to small intestine suggestive of mesenteric mass (? mesenteric cyst). Based on clinical and radiological findings a clinical diagnosis of sub-acute intestinal obstruction due to mesenteric mass was made. Patient underwent laparotomy. Intraoperative findings revealed well circumscribed, encapsulated greyish black tumor mass measuring approximately 12 cm in diameter attached to serosal aspect of the wall of ileum. It was free from adjacent structures. The mass was removed “en bloc” with piece of small intestine attached to it; end to end anastomosis was done and mass was sent for histopathological examination.
Grossly, specimen comprised of 8 cm long piece of small intestine with a mass; 12 cms in diameter attached to the serosa of small intestine. External surface–well circumscribed, encapsulated greyish black in appearance [Table/Fig-1]. Cut section showed friable, greyish brown mass with cystic areas [Table/Fig-2]. Few areas of haemorrhage and necrosis were seen. Histopathological examination revealed tumor arising from serosa of small intestine. [Table/Fig-3]. Mucosa and submucosa of ileum was normal. The tumor was composed of plump spindle to oval cells arranged in fascicles, whorls, diffuse sheets and trabeculae. Nuclei were oval to spindle shaped with pleomorphic vesicular nuclei and pale eosinophilic cytoplasm. Focal areas of haemorrhage and necrosis noted. Mitotic activity was 1/50 HPF [Table/Fig-4]. Histopathological diagnosis of GIST was given. Immunohistochemisry (IHC) study showed strong immunopositive staining of tumor cells for CD117, muscle specific actin/ calponin and focal immunoreactivity for smooth muscle actin (SMA) [Table/Fig-5]. The tumor cells revealed immunonegativity for CD34/S100 protein. Based on histomorphology and IHC final diagnosis of GIST of ileum, exhibiting smooth muscle differentiation was given and categorised into high risk group for recurrence and was referred to oncology opinion for adjuvant therapy with Imatinib. Post-operative recovery was uneventful with no recurrence and /or metastasis during the last one year follow-up.
Gross photograph showing 8 cm long piece of small intestine with a tumor mass; 12 cms in diameter attached to the serosa of small intestine. External surface –well circumscribed, encapsulated, greyish black.

Cut section -friable, greyish brown mass with areas of haemorrhage and necrosis.

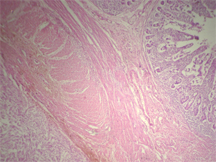
Photomicrograph showing tumor arising from serosa of small intestine.(H& E, x 100)
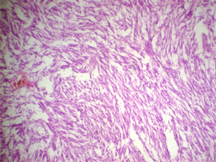
The tumor was composed of plump spindle cells arranged in fascicles, whorls, trabeculae with pleomorphic vesicular nuclei and pale eosinophilic cytoplasm. Mitotic activity was 1/50 HPF. (H&E, x 400)
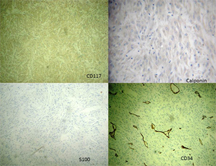
Immunohistochemistry study showed strong positive staining of tumor cells for CD117, calponin and immunonegativity for CD34/S100 protein
Discussion
Gastrointestinal stromal tumors are defined as spindle, epithelioid or occasionally pleomorphic mesenchymal tumors of gastrointestinal tract expressing the kit protein detected at immunohistochemistry [1]. GISTs are uncommon tumors; accounts for 0.1% to 3% of all gastrointestinal neoplasm [2]. They are predominantly found in stomach (60-70%) followed by small intestine (20-25 %), colorectal (5%) and oesophagus(<5 %) [3]. In upto 10% of cases GIST arises from outside bowel wall (e.g. - omentum, mesentery, peritoneum, gall bladder, liver etc) so called as EGIST [4]. Histopathological and immunohistochemical characteristics of EGIST are similar to GISTs. These tumors originate from interstitial cells of Cajal (GI pacemaker) or more primitive stem cells from which both Cajal cells and smooth muscle cells arise [5]. GIST is a distinct entity previously not differentiated from other non-epithelial neoplasms such as leiomyoma, leiomyosarcoma and leiomyoblastoma. In 1983, Mazar and Clark, first used the term GIST to include gastrointestinal non-epithelial neoplasm that lacked the immunohistochemical features of schwann cells and ultra-structural characteristics of smooth muscle [6]. GIST show broad spectrum of differentiation ranging from myoid, neural, dual differentiation to undifferentiated tumor [7]. Peak incidence of GIST is in adulthood with median age of 60 with no clear cut sex predilection.
Clinical presentation of GIST is variable depending on tumor size and anatomical sites. GISTs less than 2 cm in size are generally asymptomatic but larger GISTs present with symptoms related to mass effect like upper abdominal pain, fullness, gastrointestinal bleeding and palpable mass. In endophytic growth, tumor arising from muscularis mucosa or muscularis propria of small intestine presents with intestinal obstruction or bleeding.Exophytic tumors presents as a mass lesion or intestinal perforation [8].
GIST presenting as a small bowel obstruction is reported in less than 10% of cases [9]. Review of literature from India revealed four case reports of jejunal GIST; all presented with small bowel perforation and exophytic growth was seen in three cases [10,11]. One case report of malignant GIST of sigmoid colon with perforation and peritonitis is reported [12]. In our case, GIST presented as mesenteric mass attached to the wall of ileum and presented as a case of sub-acute intestinal obstruction due to exophytic growth which is a rare presentation of intestinal GIST. On ultrasonography GISTs are seen as well-defined masses with varying echogenicity depending on size, solid and cystic components of tumor. In our case due to necrotic and cystic areas in the tumor mass radiological diagnosis offered as mesenteric mass (suspected Mesenteric cyst) and operated accordingly.
GISTs are usually between 0.5 and 8 cm with a range from few mm to larger than 30 cm; usually well circumscribed and may have pseudocapsule.The prominent histological pattern is spindle cell type (70%) appearing as fusiform cells in intersecting whorls. Other patterns seen are epithelioid type (20%) appearing as rounded cells in a nested pattern and rarely mixed pattern is also seen [13]. On histomorphological features differential diagnosis of GIST include leiomyoma, schwannomas, intra-abdominal fibromatosis, paragangliomas etc. IHC plays a key role in the final diagnosis of GIST. Immunohistochemically GISTs are commonly positive for CD117(95%), CD 34(70%) and SMA (30-40%). 5% of tumors are positive for PDGFR mutation [13]. In our case tumor show immunopositivity for CD117, muscle specific actin and focal immunopositivity for SMA exhibiting smooth muscle differentiation.
The prognostic factors indicating malignant potential of GIST include mitotic rate, tumor size and location. No correlation between prognosis and histological type has been reported. Currently tumor less than or equal to 2 cm or with less than 5 mitosis per 50 HPF are thought to have lower malignant and metastatic potential. GIST with larger size (>10 cm in diameter) or with mitotic count >10/ 50 HPF and GIST with diameter > 5 cm and 5 mitotic figure/ 50 HPF are considered at high risk for recurrence [14]. In our case tumor was 12 cm in diameter with 1 mitotic figure per 50 HPF; so it was categorised under high risk category for recurrence and was given adjuvant therapy with Imatinib.
Surgical resection is the gold standard treatment for non-metastatic GIST. It is important to completely remove the mass “enbloc” with the contiguous tissues with avoidance of tumor rupture and spillage. The prognosis for patients who have been diagnosed with GIST has changed with the identification of the KIT mutation’s association with tumor growth. Specific therapy targeting the kit receptor with Imatinib has resulted in improved prognosis for patients with unresectable, metastatic and recurrent disease [15].
To conclude, herein we reported this case as a rare presentation of GIST causing small bowel obstruction due to exophytic growth and should be included in the differential diagnosis of mesenteric mass to reduce morbidity and mortality.
[1]. JC Burkill G, M Badran, OA Muderis, JM Thomas, Malignant Gastrointestinal Stromal Tumor: Distribution, Imaging Features and Pattern of Metastatic spread.Radiology. 2003 226:527-32. [Google Scholar]
[2]. M Miettinen, J Lasota, Gastrointestinal Stromal tumors – definition, clinical, histological, immunohistochemical and molecular genetic features & differential diagnosis.Virchows Arch 2001 438:1-12. [Google Scholar]
[3]. A Agaimy, PH Wünsch, Gastrointestinal stromal tumours: a regular origin in the muscularis propria, but an extremely diverse gross presentation. A review of 200 cases to critically re-evaluate the concept of so-called extra-gastrointestinal stromal tumours.Langenbecks Arch Surg 2006 391:322-29. [Google Scholar]
[4]. RP Dematteo, JJ Lewis, D Leung, SS Mudan, JM Woodruff, Two hundred gastrointestinal tumors: recurrence patterns and prognostic factors for survival.Ann Surg. 2000 231:51-8. [Google Scholar]
[5]. Y Hwangbo, H Clark, Gastric stromal tumors. Reappraisal of histogenesisAm J Surg Pathol 2011 41(8):1085-90. [Google Scholar]
[6]. M Mazur, H Clark, Gastric stromal tumors. Reappraisal of histogenesisAm J Surg Pathol 1983 7:507-19. [Google Scholar]
[7]. F Farinati, R Cardain, M De Giorgio, New approaches to management of gastrointestinal stromal tumours. Basic mechanism of digestive diseases. M.J.G. Farthing, P. Malfertheiner, 2002 ParisJohn Liebbey Eurotext:75-92. [Google Scholar]
[8]. H Kimura, T Yoshida, S Kinoshita, I Takahashi, Pedunculated giant gastrointestinal stromal tumor of the stomach showing extra gastric growth: report of a case.Surg Today 2004 34:159-62. [Google Scholar]
[9]. M Miettinen, JM Monihan, RM Sarlomo, AJ Kovatich, NJ Carr, TS Emory, Gastrointestinal stromal tumors/smooth muscle tumors (GISTs) primary in the omentum and mesentery: clinicopathologic and immunohistochemical study of 26 cases.Am J Surg Pathol. 1999 23(9):1109-18. [Google Scholar]
[10]. C Chatterjee, D Khan, U De, A rare presentation of gastrointestinal stromal tumors as a small bowel perforation: A single institution based clinical experience of three cases.J Dr NTR Univ Health Sci 2013 2:118-21. [Google Scholar]
[11]. M Usha, Kumar Vijay, R Rau Aarathi, Kamath Sulatha, Perforated GIST in Jejunum-A rare cause of Abdominal Cocoon.Journal of Clinical and Diagnostic Research. 2014 8(3):132-33. [Google Scholar]
[12]. SV Jagtap, DB Nikumbh, AY Kshirsagar, A Bohra, W Khatib, Malignant Gastrointestinal Stromal tumor of the Sigmoid Colon with Perforation and Peritonitis - an Unusual PresentationInternational Journal of Health Sciences & Research. 2012 2(3):105-09. [Google Scholar]
[13]. Laperouse Patrick, Raines Daniel, Diamond Karen, Rivera Sammy, Newman William, Hew Alfred Y, Gastrointestinal Stromal Tumors:A Case Report and Review of the Literature.J La State Med Soc. 2008 160:128-33. [Google Scholar]
[14]. CD Fletcher, JJ Berman, C Corless, F Gorstein, J Lasota, BJ Longley, Diagnosis of gastrointestinal stromal tumors: A consensus approachHum Pathol 2002 33:459-65. [Google Scholar]
[15]. L Schubert M, R moghimi, Gastrointestinal stromal tumor (GIST).Curr Treat Options Gastroenterol 2006 9(2):181-8. [Google Scholar]