Isolated Splenic Hydatidosis
Raghavendra Sawarappa1, Aditya Kanoi2, Madhumita Gupta3, Ashwin Pai4, S I S Khadri5
1Faculty, Department of General Surgery, SSKM and IPGMER Hospital, Kolkata, India.
2Faculty, Department of General Surgery, SSKM and IPGMER Hospital, Kolkata, India.
3Faculty, Department of Plastic Surgery, SSKM and IPGMER Hospital, Kolkata, India.
4Faculty, Department of General Surgery, SSKM and IPGMER Hospital, Kolkata, India.
5Faculty, Department of General Surgery, Bangalore Medical College and Research Centre, Bangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Aditya Kanoi, 2D Singhi Park, 48/3 Gariahat Road, Kolkata -700019, West Bengal, India.
Phone: +91 9830377341, Fax: +91 033 24617306
E-mail: aditya.kanoi@gmail.com
A 27-year-old female presented with pain in the left hypochondrium for the past six months. An abdominal examination revealed mild splenomegaly. An abdominal ultrasonography showed two cystic lesions at the superior pole of the spleen. Contrast enhanced CT scan abdomen confirmed the USG findings, demonstrating splenomegaly with nonenhancing cystic lesions having internal septations and suspicious daughter cysts within it, strongly suggestive of hydatid cysts. On serological testing, the patient was positive for IgG Antibodies against Eccinococcus. Following Pneumococcal vaccination, splenectomy was performed taking precautions to prevent accidental rupture or spillage of contents into the peritoneum. The postoperative period was uneventful with the patient making a swift recovery. Histopathological examination revealed extensive necrosis within the cysts. In the midst of the necrotic material, hooklets were seen. These features were consistent with a diagnosis of an infected Hydatid cyst. It is of utmost importance that a correct preop diagnosis is made since all precautions must be taken to prevent dissemination or seeding of the surgical field. Death has been reported due to anaphylactic shock resulting from spillage during excision or biopsy. The most important factor in diagnosing splenic hydatid cyst is the awareness of its possibility.
Hydatid cyst, Infected hydatid cyst, Nonspecific abdominal symptoms, Spleen, Zoonosis
Case Report
A 27-year-old female presented with complaints of pain in the left hypochondrium for the past six months. Pain was dull aching, continuous, without aggravating or relieving factors. No diurnal variations or associated fever reported. The patient belonged to a non-farming family, however, having a pet dog at home. Abdominal examination revealed mild splenomegaly. Laboratory tests, CBC, LFT & biochemistry were all within normal limits. Plain X-ray abdomen was unremarkable [Table/Fig-1] .
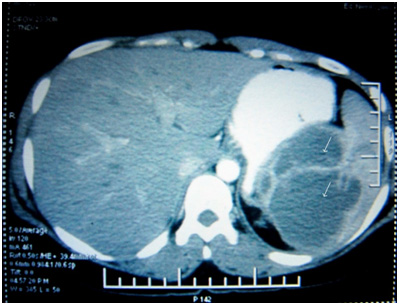
An abdominal ultrasonography was carried out which showed two cystic lesions with multiple septations at the superior pole of the spleen. Contrast enhanced CT scan abdomen confirmed the USG findings [Table/Fig-2] , demonstrating splenomegaly with non enhancing cystic lesions having internal septations and suspicious daughter cysts within it, strongly suggestive of hydatid cysts.
There was no involvement of liver or other abdominal organs. A chest X ray and CT brain failed to show any lung or brain involvement, respectively. On serological testing, the patient was positive for IgG Antibodies against Eccinococcus.
Following Pneumococcal vaccination, splenectomy was performed taking precautions to prevent accidental rupture or spillage of contents into the peritoneum. The postoperative period was uneventful with the patient making a swift recovery.
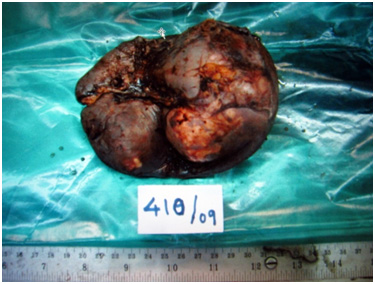
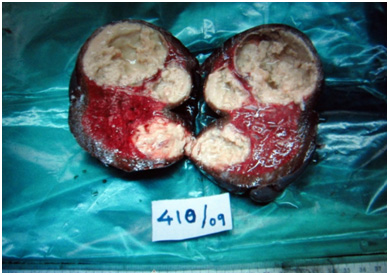
Histopathological examination revealed extensive necrosis with in the cysts [Table/Fig-3,4] , with the cyst wall being infiltrated by mononuclear inflammatory cells. In the midst of the necrotic material, hooklets were seen. No evidence of granuloma or malignant deposits was found. These features were consistent with a diagnosis of an infected Hydatid cyst.
Discussion
Hydatid disease (aka: echinococcosis), is a zoonosis that occurs primarily in sheep-grazing areas of the world, but is nevertheless common worldwide. Man is an accidental host in the life cycle of Echinococcus granulosus. Human infestation occurs due to ingestion of eggs. Larva liberated from eggs penetrates the bowel mucosa to enter the portal system thereby spreading to various organs [1]. Although Hydatid disease can affect any part of the body, the cysts are by and large found in the liver (55.6%) and lungs (30%) [2,3]. The incidence of splenic involvement by hydatid cysts in relation to the rest of the abdominal viscera is extremely low, constituting 0.5 to 4% of all cases of hydatidosis [4].
According to Gupta et al., cysts are found in the liver (55%-60%), lungs (30%), kidney (2.5%), heart (2.5%), bones (2%), muscles (1%), brain (0.5%) and spleen (1.5%) [4].
Cangiotti et al reported cases with rare localization of Hydatid cysts during a period of 18-years and in only 8 patients (14%), organs other than liver were involved of which one case was a Hydatid cyst of spleen [5].
Reviewing the reported incidences by different authors, it is clear that splenic hydatid disease is a rare entity.
The first clinical indication of the presence of hydatid disease of spleen frequently is an accidentally discovered splenomegaly [6]. Symptoms are few and nonspecific, consisting of a left hypochondrial mass, dull aching pain, dyspepsia, constipation (consequential to the cysts causing compression of the colon) and dyspnoea (as a result of the left diaphragm being pushed up). The likely complications can be infection, rupture in the abdominal cavity or fistulization to the colon. The major challenge in the diagnosis of splenic hydatidosis is in differentiating it from other splenic cystic lesions, such as epidermoid cyst, pseudocyst, abscess, hematoma, and cystic neoplasms of the spleen. Hydatidosis should always be suspected, particularly in endemic areas.
Definitive diagnosis is based on abdominal ultrasound and CT scan which have good sensitivity and specificity. Ultrasound is universally used for the diagnosis of Echinococcosis because of its availability, affordability, and accuracy. On ultrasound of abdomen, splenic hydatid cyst may present as a solitary unilocular or rarely multiple well defined anechoic spherical cystic lesions or may demonstrate an anechoic spherical cystic lesion with hyperechoic marginal calcification, as seen in this case. CT abdomen confirms the cystic lesion with or without daughter cysts within the spleen with attenuation value near that of water that does not enhance after intravenous contrast administration. It is more sensitive than ultrasonography in depicting subtle wall calcification. Various serological tests are being carried out for diagnosis, screening and postoperative follow-up for recurrence. These include hydatid immunoelectrophoresis, enzyme linked immunoabsorbent assay (ELISA), latex agglutination and indirect hemagglutination test.
Splenectomy has been the conventional treatment of choice for splenic hydatidosis. It is of utmost importance that a correct preop diagnosis is made since all precautions must be taken to prevent dissemination or seeding of the surgical field[7,8]. Death has been reported due to anaphylactic shock resulting from spillage during excision or biopsy.
This case report, although an isolated event, demonstrates, what we think is the correct way to approach suspected hydatid disease of the spleen. The most important factor in diagnosing splenic hydatid cyst is the awareness of its possibility. By keeping an open mind, especially in endemic areas, a major catastrophe can be avoided.
Chest X-ray film showing a normal study
CECT abdomen showing splenic hydatid cysts (white arrows), liver being normal
Gross specimen of the spleen following its removal
Cut section of the spleen revealing multiple cysts
[1]. N Sekar, KK Madhavan, RV Yadav, RN Katara, Primary Retroperitoneal Hydatid cyst. A case report and review of literature. J PostGraduate Med. 1982 28:112-48. [Google Scholar]
[2]. C Dziri, Hydatid disease: Continuing serious public health problem.Introduction.World J Surg. 2001 25:1-3. [Google Scholar]
[3]. DP McManus, W Zhang, J Li, Echinococcosis.Lancet. 2003 362:1295-304. [Google Scholar]
[4]. A Gupta, A Kakkar, M Chadda, A Primary intrapelvic Hydatid cyst presenting with foot drop and a gluteal swelling.British Journal Bone Joint Surgery. 1998 808:1037-8. [Google Scholar]
[5]. L Congiotti, P Mueisan, A Begni, Unusual localisation of hydatid disease.Giornale di Chiturgid. 1994 15(3):836 [Google Scholar]
[6]. CE Davis, JM Montero, CN VanHorn, Large splenic cysts.Ann Surg. 1971 173:686-92. [Google Scholar]
[7]. I Seymour, Schwartz Ellis Harold, Maingot’s Abdominal Operations.1226Ninth edition [Google Scholar]
[8]. I Seymour, Schwartz Ellis Harold, Maingot’s Abdominal Operations.Ninth edition:1535-45. [Google Scholar]