Diagnostic CBCT in Dentigerous Cyst with Ectopic Third Molar in the Maxillary Sinus–A Case Report
Mamatha N.S.1, Bhuvana Krishnamoorthy2, Savitha J K3, Pankaja Bhai4
1Professor, Department of Oral and Maxillofacial Surgery, Rajarajeswari Dental College and Hospital, Kumbalgodu, Ramohalli Cross, Mysore Road, Bangalore, India.
2Associate Professor, Department of Oral Medicine and Radiology, ITS-Centre of Dental Sciences and Research, Delhi-Meerut Road, Muradnagar, Ghaziabad, Uttar Pradesh, India.
3Reader, Department of Oral and Maxillofacial Pathology, Rajarajeswari Dental College and Hospital, Kumbalgodu, Ramohalli Cross, Mysore Road, Bangalore, India.
4Reader, Department of Oral and Maxillofacial Surgery, College of Dental Science and Hospital, Amargad, Bhavnagar, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bhuvana Krishnamoorthy, Associate Professor, Department of Oral Medicine and Radiology, ITS-Centre of Dental Sciences and Research, Delhi-Meerut Road, Muradnagar, Ghaziabad, Uttar Pradesh, India.
Phone: (91) 9999509465, Fax no: (01232) 225382,
E-mail: bhuvanakrishnamoorthy@yahoo.com
Dentigerous cyst is the second most common odontogenic cyst after radicular cyst. This report describes a case of a dentigerous cyst associated with an impacted maxillary third molar. Patient presented with foul smelling discharge through nose and oral cavity. Cone beam computed tomography revealed maxillary third molar displaced to lateral wall of the nose and a unilocular radiolucency obliterating the entire maxillary sinus. A provisional diagnosis of infected dentigerous cyst was made. The cyst was enucleated along with removal of third molar. Histopathological examination confirmed the diagnosis of dentigerous cyst. The patient recovery was uneventful.
Caldwell-Luc procedure, Cone beam computed tomography, Ectopic, Impacted third molar, Maxillary sinus
Case Report
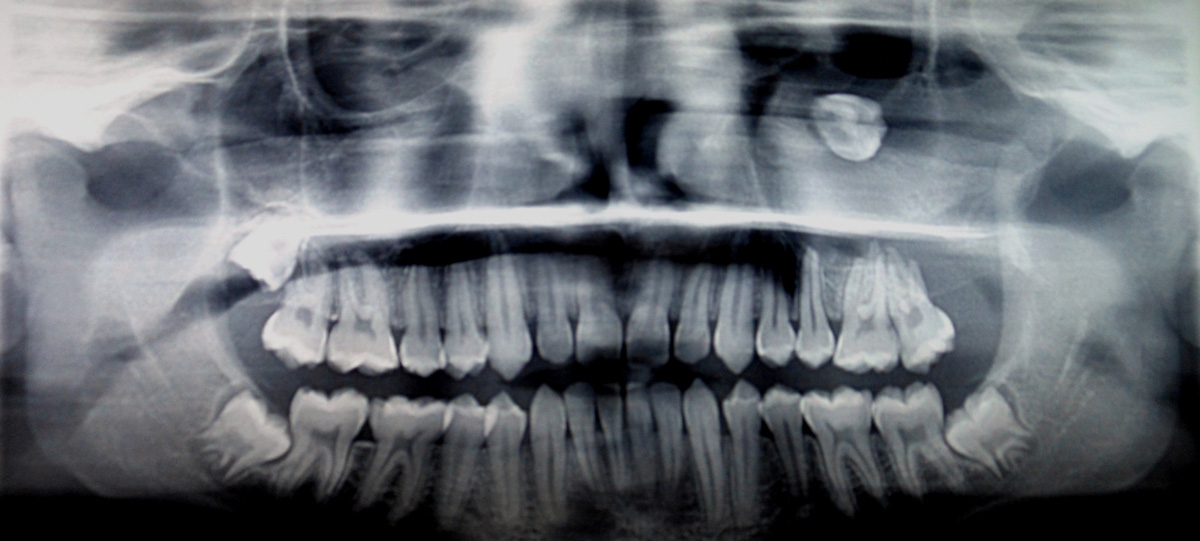
A 17-year-old male reported to a private hospital with the chief complaint of foul smelling discharge through left nostril and salty discharge from behind the upper left back tooth since four months. It started with mild pain and slight swelling on the middle third of the face on the left side. He reported no difficulty in mastication. He had not received any treatment for the same. Past medical and dental history was not contributory. General physical examination revealed no remarkable findings. On extra oral inspection, there was slight facial asymmetry due to a diffuse swelling on left middle third of the face extending from the left infraorbital region to about 1 cm below the the alatragal line superoinferiorly and anteroposteriorly from the nasolabial fold to the line drawn from the outer canthus of the eye. The left nasolabial fold was obliterated. The skin over the swelling appeared normal. On palpation the inspectory findings were confirmed , the swelling was soft in consistency and mildly tender to touch. On intra oral examination, there was obliteration of labial vestibule in relation to left maxillary canine and premolars. There was a draining sinus distal to second molar on the alveolar ridge area of the missing 28. The second molar was slightly tender on percussion. On palpation there was expansion of the buccal cortical plate in the region of 25, 26 and missing 28. Panoramic radiograph showed that 28 was impacted and placed high near the left infraorbital rim [Table/Fig-1]. Cone beam computed tomography was advised which revealed a large expansile unilocular radiolucency in the left maxilla measuring approximately 4.9×4.3×4.4cms. It extended from lesion28 to the lateral wall of the nasal cavity mediolaterally and from the alveolar process to the orbit superoinferiorly. The internal structure was uniformly radiolucent with a thin radio-opaque border. The perforation in the alveolar process in the region of the 28 was clearly visible and there was resorption of the roots of 27. Third molar was displaced into lateral wall of the nose. Also the floor of the orbit was raised superiorly [Table/Fig-2a,Table/Fig-2b,Table/Fig-2c]. A working diagnosis of an infected dentigerous cyst involving the left maxillary sinus was made.
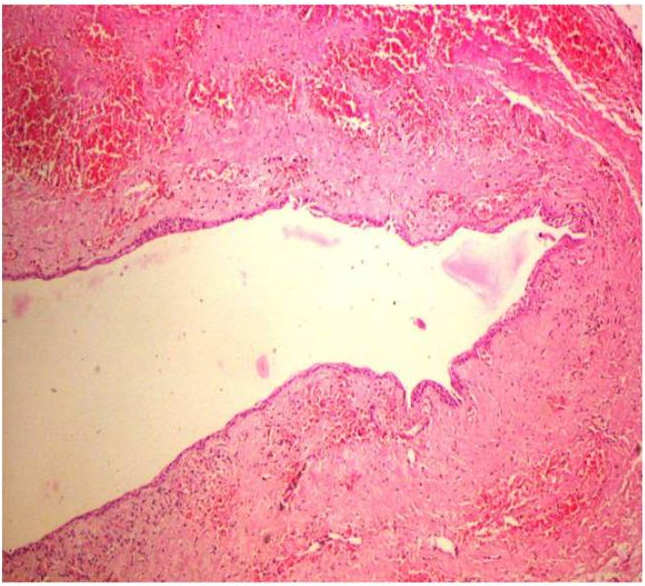
Under general anaesthesia, through Caldwell – Luc approach, a vestibular incision was placed from canine to first molar. A bony window was created [Table/Fig-3] and the tooth was removed along with the enucleation of cyst [Table/Fig-4]. The cyst had occupied the entire maxillary sinus. Root of the third molar was yet to be formed. The cavity was irrigated, haemostasis was achieved and intra nasal antrostomy was done. The cavity was packed with gauze and was brought out through the left nostril and vestibular incision was closed. The specimen was sent to histopathological examination. Histology showed a fibrous cystic wall lined by a 2-3 cell layers thick non-keratinized stratified squamous epithelium lining the lumen [Table/Fig-5]. Flat epithelial connective tissue interface seen. Connective tissue stroma showed inflammatory cell infiltrate. These findings confirmed diagnosis of dentigerous cyst. The gauze pack was removed after three days. Wound healing was uneventful.
Discussion
Pathologies such as cyst or tumor in relation to a developing tooth is one of the three main causes of ectopic eruption of the tooth, the others being-developmental disturbance and iatrogenic activity [1]. Ectopic eruption of teeth into a nondental location like the maxillary sinus is rare. Dentigerous cyst associated with the maxillary third molar is a rare clinical entity (1%), with very few such reports in literature [2,3].
Most dentigerous cysts are completely asymptomatic and remain dormant until infected, when they are painful or until they have enlarged substantially, when they produce expansion and swelling of the jaw [4]. This holds good even in cases where the maxillary antrum is invaded. Failure to intervene may result in the enchroachment of the cyst into nasal septum, orbit, it may cause chronic maxillary sinusitis or very rarely malignant transformation [3]. The cyst may be discovered during routine radiographic examination. Conventional radiographs are useful in identifying and establishing a provisional diagnosis of the lesion. But specialized imaging modalities like computed tomography (CT) and cone beam computed tomography (CBCT) are of utmost importance in the management of these cysts involving the maxillary sinus. CBCT is especially valuable in demarcating the hard tissue periphery from the soft tissue invlovemnt of the lesion. The major advantages of CBCT are they provide multiplanar reformation with volume reconstructions and 3D images with a much lower radiation dose when compared to computed tomography.They enable the surgeon to accurately assess the extent of the lesion as well as its proximity to the contiguous vital structures [4]. The CBCT of our patient showed the entire extent of the enormous lesion. We could visualize the complete obliteration of the left maxillary sinus and the raised floor of the left orbit. Post operatively too CBCT is useful as it aids to visualize changes in the endosteum during the healing at the site of surgery.
Irrespective of the location, dentigerous cysts are treated surgically, either by enucleation or marsupialisation [4]. In paediatric patients, 8marsulpialisation is preferred since it promotes the natural eruption of the affected tooth [5]. Caldwell-Luc procedure is excellent for approaching the maxillary sinus. It is fenestration of anterior wall of the maxillary sinus and surgical drainage of the sinus into the nose via antrostomy. It is used for removal of tumors, cysts, polyps or foreign bodies, chronic sinusitis, reduction of facial fractures, orbital floor decompression, closure of oroantral fistula, as a route to ethmoid and sphenoid sinuses, access to pterygomaxillary fossa for internal maxillary artery ligation and for an approach to sphenopalatine ganglion. The most common complications associated with Caldwell-Luc procedure are facial swelling, infra orbital paraesthesia, numbness of the teeth. Some of the rare complications are post operative epistaxis, oro antral fistula, epiphora and tooth discolouration [6]. Sometimes during Caldwell–Luc procedure, when the osteomeatal complex is not patent, an inferior meatal antrostomy is done for passive drainage. This however, has certain disadvantages like it requires additional time, can cause injury to nasolacrimal duct, epistaxis or alteration in normal sinus physiology [7]. With a introduction of endoscopic sinus surgery, Caldwell-Luc procedure is now more selectively used.
Panoramic radiograph showing impacted 28. Obliteration of the maxillary sinus on the left side can be well appreciated. The impacted third molar has been displaced to the infraorbital rim by the enormous lesion
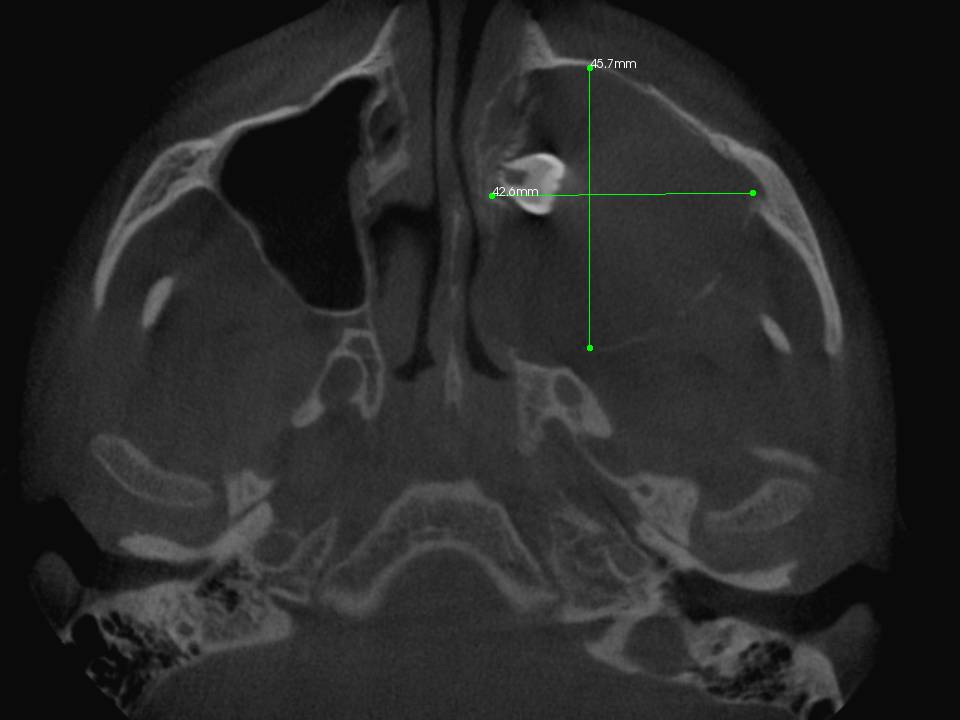
Axial section of CBCT shows the enormous lesion that has caused displacement of the maxillary third molar to the lateral surface of nasal cavity
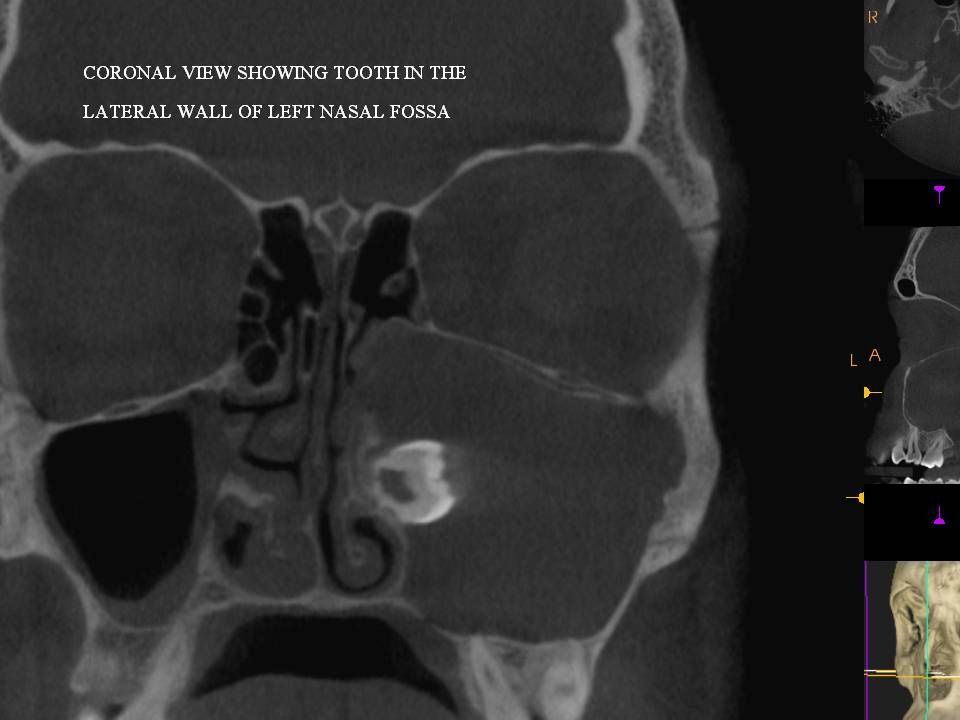
Coronal view of CBCT showing the exact position of the tooth and the lesion
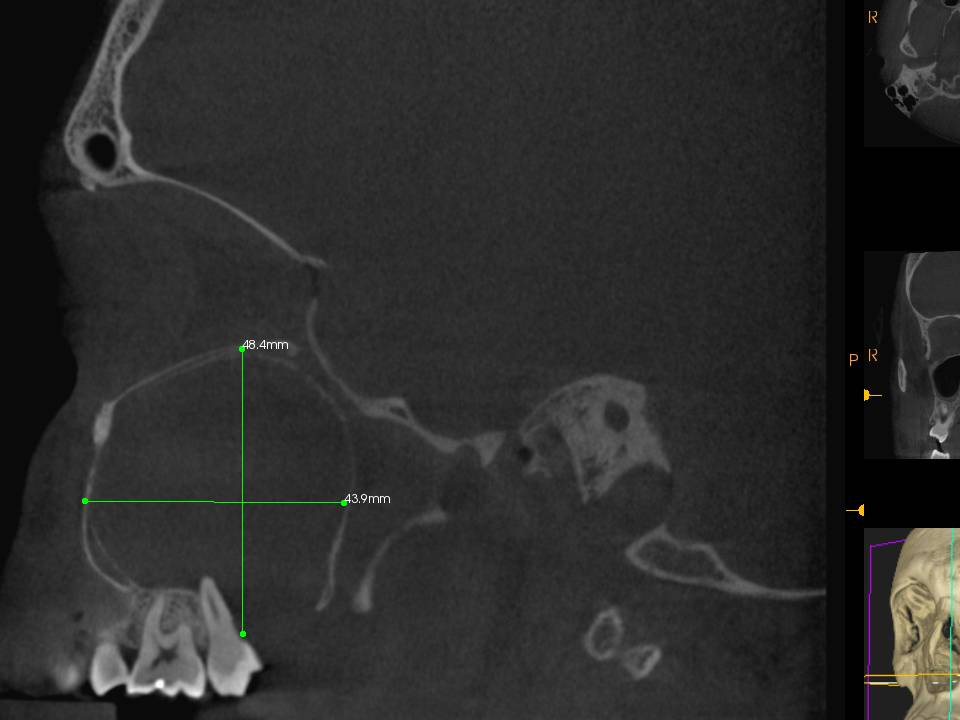
Sagittal CBCT section showing the resorption of the alveolar process inferiorly resulting in a communication with the oral cavity
Bony window created in the maxillary sinus via the Caldwell-Luc procedure
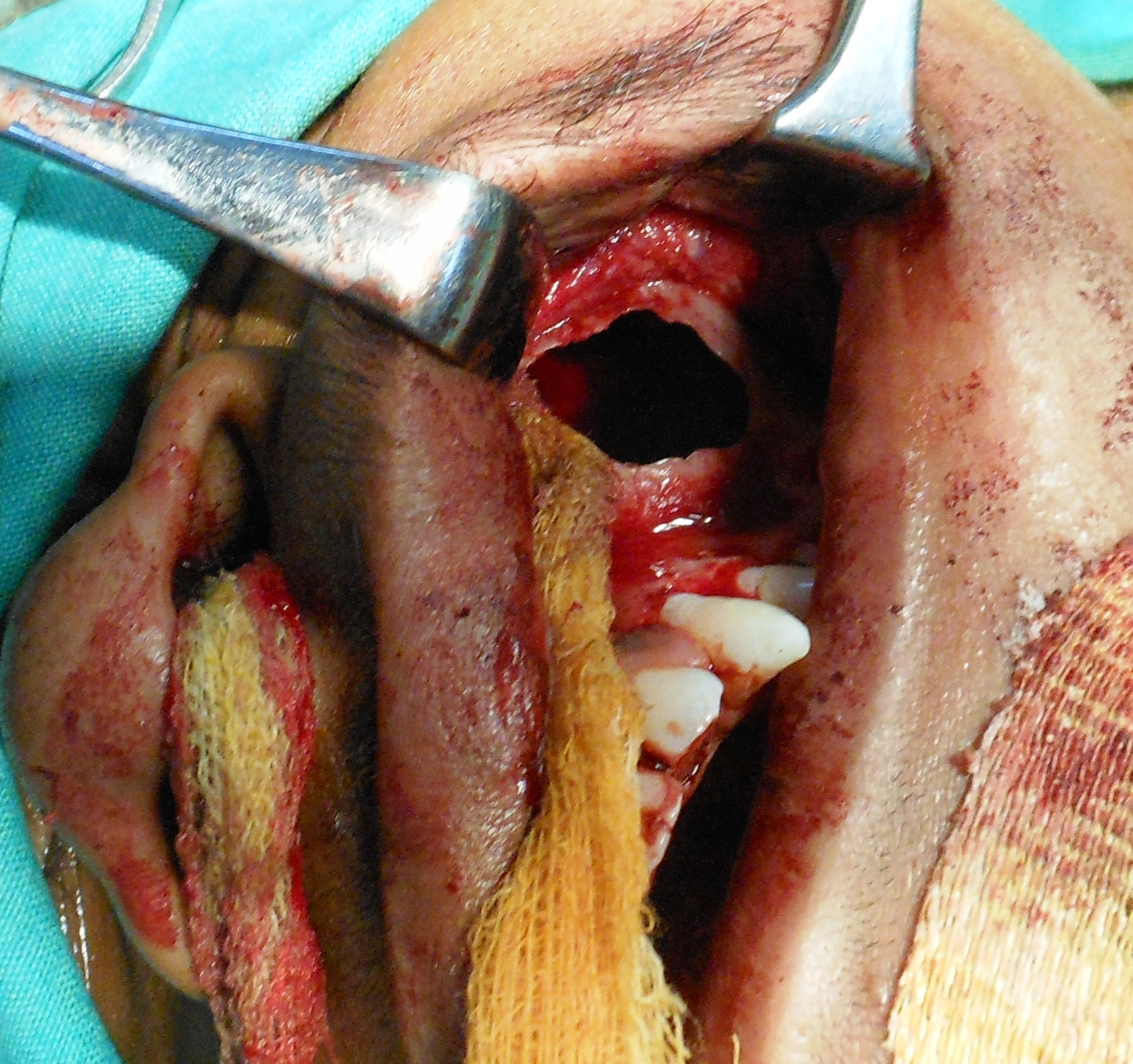
Cyst with the attached third molar that was enucleated from the sinus

Shows histological section of the specimen. The epithelial lining of the dentigerous cyst can be appreciated (H&E staining, original magnification 10x)
Conclusion
Dentigerous cysts of maxillary third molar are less common than those occurring elsewhere. They can enlarge to involve the maxillary sinus and may result in chronic maxillary sinusitis, nasal obstruction and oro antral fistula if they remain untreated. Missing tooth or unusual eruption pattern should be investigated radiologically to identify and prevent development of pathology. CT and CBCT are particularly useful in the surgical planning of such expansile cysts. In our case Caldwell-luc procedure provided a wide exposure for removal of tooth and enucleation of dentigerous cyst. Inferior meatal antrostomy was performed, without any complications, to provide a dependent drainage. Oro antral fistula was successfully closed.
[1]. PJ Slotweg, Carcinoma arising from reduced enamel epithelium.J Oral Pathol. 1987 16:497-82. [Google Scholar]
[2]. MC Buyukkurt, MM Omezli, O Miloglu, Dentigerous cyst associated with an ectopic tooth in the maxillary sinus: a report of 3 cases and review of the literature.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 109:67-71. [Google Scholar]
[3]. S Asnani, U Mahindra, BM Rudagi, Y Kini, VR Kharkar, Effect of administration of tetracycline in pregnancy on the primary dentition of the offspringD Ind J Dent Res. 2012 23(6):833-34. [Google Scholar]
[4]. ZA Amin, M Amran, A Khairudin, JJ Hefferren, Removal of extensive maxillary dentigerous cyst via a Caldwell- Luc procedure.Arch Orofac Sci. 2008 3(2):48-51. [Google Scholar]
[5]. S Takagi, S Koyama, Guided eruption of an impacted second premolar associated with a dentigerous cyst in the maxillary sinus of a 6-year-old child.J Oral Maxillofac Surg. 1998 56:237-9. [Google Scholar]
[6]. WK Low, S Mehta, R Kalra, Complications of Caldwell-Luc and how to avoid them.Aus NZ J Surg. 1995 65(8):582-4. [Google Scholar]
[7]. FA Al-Belasy, Inferior meatal antrostomy : is it necessary after radical sinus surgery through the Caldwell-Luc approach?J Oral Maxillofac Surg. 2004 62(5):559-62. [Google Scholar]