Removable Partial Denture Supported by Implants with Prefabricated Telescopic Abutments - A Case Report
Lalit Kumar1, Komal Sehgal2
1 Senior Lecturer, Department of Prosthodontics, Dr Harvansh Singh Judge Institute of Dental Sciences and Hospital, Chandigarh, India.
2 Reader, Department of Prosthodontics, Dr Harvansh Singh Judge Institute of Dental Sciences and Hospital, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lalit Kumar, House No 222 G/F, Sector 37 A, Chandigarh 160036, India.
Phone: +91 9914419876,
E-mail: drlalitbida@gmail.com
Implants have been designed to rehabilitate edentulous patients with fixed prosthesis or implant supported overdentures. Implant-supported single crowns and fixed partial dentures have become successful treatment alternatives to removable and fixed partial dentures. However, it is common to have clinical situations which make it impossible to use conventional as well as implant supported fixed partial dentures. The implant supported removable partial dentures can be a treatment modality that offers the multitude of benefits of implant-based therapy—biologic, biomechanical, social, and psychological to such patients.
The aim of this article is to present a case report describing the fabrication and advantages of removable partial denture supported by teeth and implants for a patient with long edentulous span. The patient was satisfied with his dentures in terms of function and aesthetics. Regular follow-up visits over a period of three years revealed that the periodontal condition of remaining natural dentition and peri-implant conditions were stable. There was no evidence of excessive residual ridge resorption or mobility of the teeth, nor were any visible changes in the bone levels of the natural teeth or implants noted on radiographs.
Implant supported removable partial denture, Implants, Telescopic Crowns
Case Report
A 62-year-old, healthy male patient reported to the department of prosthodontics with the complaint of ill fitting flexible upper partial denture fabricated about four years back. A recent orthopantomograph(OPG) and exploring the dental history of the patient revealed that he had got 14, 24 extracted about 2 months back as they got fractured and were the abutments with clasps for his existing Removable Partial Denture (RPD) [Table/Fig-1]. The initial clinical findings are as mentioned in [Table/Fig-2].
Intraoral view showing ill fitting conventional RPD

Initial clinical findings
| • Missing Teeth- 16,14,13,12,11,21,22,23,24,25,27 |
|---|
| • Crown – 26 (inadequate marginal fit) |
| • FPD – 33 to 38 |
| • Implant supported Crowns 45,46 |
| • Ill fitting partial denture |
The oral examination along with the recent radiograph showed insufficient bone for implant placement in maxillary posterior region without extensive bone grafting and sinus lift surgery. The patient was not keen for implant supported fixed prostheses because of the additional surgical procedures and the financial limitations and desired a less complicated, yet effective treatment. Radiographic examination revealed availability of sufficient bone for implant placement in the 13, 23 regions. The presence of mandibular anterior teeth opposing maxillary anterior ridge and hence the need to prevent maxillary anterior ridge resorption (Kelly’s combination syndrome) in the future was also a consideration while planning to place implants in the maxillary canine regions bilaterally.
For retention and support of removable partial denture, circumferential clasps on 15,17, 26 and two ANKYLOS® SynCone® C/ Abutment (Dentsply Friadent Mannheim/Germany) with ANKYLOS® Taper Cap Degulor® for SynCone® 4° in region of 13 and 23 were used. The implant system used was ANKYLOS® C Mannheim/Germany.
Procedure
Prophylactic antibiotic (Amoxicillin+ Clavulanic acid 625mg TID) was administered to the patient on the day of the surgery and continued for five days.
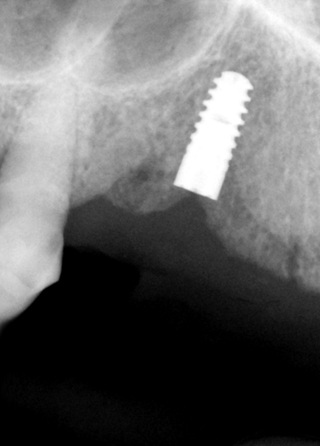
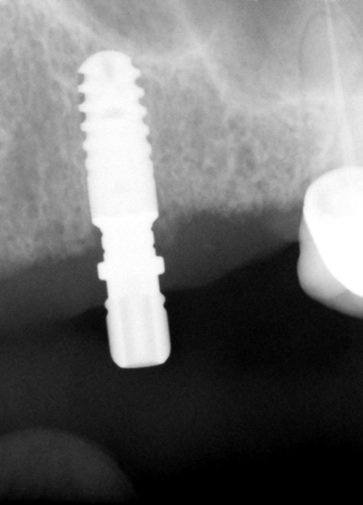
ANKYLOS® C implants of dimension B9.5(4.5 x 9.5) in region of 23 and A11.5 (3.5 x 11.5) in region of 13 were placed using the standard protocol [Table/Fig-3,4].
Radiograph showing implant in 13 region
Radiograph showing implant in 23 region
After three months of healing period, radiographs demonstrated successful oseointegration of the implants placed.
Implant level impression was taken using ANKYLOS® Regular C/Transfer Post (Repositioning Technique) with polyether impression material [Table/Fig-5].
Transfer posts for taking implant level impression

Maxillary anteroposterior palatal strap cast metal framework was fabricated and trial was done to check for the fit.
After recording maxilla-mandibular jaw relation record, teeth arrangement and trial of waxed up RPD was done.
SynCone® C/ Abutment 4° taper of 4.5 mm gingival height(G/H) and 15° angulation was used for 13 region and 3.0 mm G/H and 0° angulation for 23 region was used and torqued with 15 Ncm [Table/Fig-6].
SynCone Abutment with prefabricated telescopic copings

The final denture was tried in the patients mouth and the prefabricated telescopic copings ANKYLOS® Taper Cap Degulor® for SynCone® 4° were retro- fitted and cemented to the cast metal framework using self cure acrylic resin [Table/Fig-7].
Intaglio surface of the finished removable partial denture

The denture base acrylic replicated the lost natural soft-tissue architecture and permitted placement of appropriate sized teeth. The final result provided a stable and functional RPD with a highly aesthetic appearance for the patient [Table/Fig-8].
Intraoral facial view of the implant supported RPD

Discussion
Numerous studies and clinical reports have demonstrated the multitude of merits and patient benefits derived from implant based therapy. The predictability of fixed implant supported restorations, as well as health, psychological and functional benefits of overdentures are well documented [1]. There is however, sparse literature discussing the utilization of implants with removable dentures for partially edentulous patients.
Although the advantages of fixed implant restorations are undisputed, there are many patients wherein the fixed implant restoration may not be possible without bone grafting and additional surgical procedures. Other limitations of fixed implant restoration are a result of excessive ridge resorption with loss of facial support of lips and soft tissues of face, lack of hygiene access, requirement of more number of implants for fixed restorations, multiple surgical procedures and more time and cost involved [2,3].
In contrast, the limitations of conventional, non-implant supported RPD include a lack of stability, insufficient retention, periodontally compromised abutment teeth, and unaesthetic clasps. These limitations frequently are accompanied by discomfort, accelerated tooth loss, ridge resorption and traumatic forces, as well as patient reluctance to use the appliance routinely [4,5].
Considering these limitations, an implant supported RPD can be a viable treatment alternative to conventional RPDs and implant supported fixed prostheses in many patients with few remaining teeth and anatomical challenges [6,7]. Many of the problems with conventional RPDs can be overcome with the placement of one or more strategically positioned implants. These enhanced RPDs have been called implant-assisted removable partial dentures (IARPD) (Schneid T, et al.,), implant-retained partial overdentures (IRPOD) (Chikunov I, et al.,) and implant-supported removable partial dentures (ISRPD) (Ohkubo C et al.,) [8–10]. The ISRPD serves as a cost-effective, prosthetic solution for partially edentulous patients who are not candidates for extensive, fixed implant supported restorations [9].
The current case report describes the fabrication of a maxillary RPD supported by existing posterior teeth and two implants with prefabricated telescopic attachments (Ankylos® SynCone®, DENTSPLY Friadent GmbH, Mannheim, Germany), which effectively provided support and retention to the partial denture. Though other type of attachments [9,11] has been reported to be used with removable partial dentures, this report includes the use of implants with prefabricated telescopic copings.
The combination of dental implants to support the RPD might alleviate some of the problems associated with conventional RPDs [Table/Fig-9] and also offers an effective treatment alternative to patients where implants supported prostheses is not feasible or desirable because of emotional or financial limitations. Studies have reported that the use of implants in conjunction with remaining natural teeth in the implant supported RPD substantially improve oral health quality of life for patients compared to conventional treatment options [12–14]. The patients receiving this treatment had only minor prosthetic complications, great satisfaction, and improved chewing efficiency. The researchers determined that the treatment modality is viable and cost-effective. Other studies have confirmed improved esthetics, fewer patient visits, and the ability to avoid additional surgical procedures. This modality can be a rewarding treatment option as it can provide outstanding comfort and satisfaction to patient and offers prosthetic simplicity and the ability to perform maintenance and modification over the long term to clinician.
Advantages of an implant-enhanced removable partial denture versus conventional removable partial denture
| Enhanced retention, support and stability |
|---|
| Improved aesthetics with elimination of some retentive clasps |
| Preservation of remaining residual ridge by better distribution of forces and elimination of damaging leverage to natural abutment teeth |
| Improved comfort and confidence |
| Psychological advantage to patient of preserving compromised natural teeth that are not suitable to use as abutments to support an RPD |
| An increase in masticatory efficiency |
| A futuristic treatment plan where implant placement may be staged and this prosthesis can be used as an interim option |
ISRPD is a space-sensitive treatment [15]. Inter-occlusal space must be carefully assessed prior to treatment. Insufficient bulk of acrylic may lead to poor strength and need for frequent repairs of the prosthesis. Design principles for an ISRPD should be consistent with those of a conventional RPD. The partial denture should be well reinforced with metal around the location of the implant attachments. This prevents complications like the fracture of acrylic around the implant attachment housing.
As discussed in this case report, this patient’s major problem was inability to chew properly and non retentive partial denture. A conventional RPD distributes chewing force between natural teeth abutments and soft tissues. An ISRPD distributes the force among natural teeth abutments, soft tissues and implants. By adding an implant to a RPD, the retention, support and stability of the RPD are all enhanced. The implants and the maxillary RPD have been followed for 36 months and the patient has been comfortable and satisfied as regards the fit and chewing efficiency. It can be concluded that incorporation of dental implants to improve the support and retention and to enhance patient acceptance should be considered when treatment planning for removable dentures for partially edentulous patients.
[1]. Awad MA, Locker D, Korner-Bitensky N, Measuring the effect of intraoral implant rehabilitation on health-related quality of life in a randomized controlled clinical trialJ Dent Res 2000 79(9):1659-63. [Google Scholar]
[2]. Vogel RC, Implant overdentures: a new standard of care for edentulous patients- current concepts and techniquesFunctional Esthetics and Restorative Dentistry 2007 1(2):30-6. [Google Scholar]
[3]. Chang LC1, Wang JC, Tasi CC, Removable partial denture on osseointegrated implants and natural teethChang Gung Med J 2007 30(3):274-9. [Google Scholar]
[4]. Mitrani R, Brudvik JS, Phillips KM, Posterior implants for distal extension removable prostheses: a retrospective studyInt J Periodontics Restorative Dent 2003 23(4):353-9. [Google Scholar]
[5]. Mijiritsky E, Implants in conjunction with removable partial dentures: a literature reviewImplant Dentistry 2007 16(2):146-54. [Google Scholar]
[6]. Mijiritsky E, Ormianer Z, Klinger A, Use of dental implants to improve unfavourable removable partial denture designCompend Contin Educ Dent 2005 26(10):744-50. [Google Scholar]
[7]. Grossmann Y, Nissan J, Levin L, Clinical effectiveness of implant-supported removable partial dentures: a review of the literature and retrospective case evaluationJ Oral Maxillofac Surg 2009 67(9):1941-6. [Google Scholar]
[8]. Schneid T, Mattie P, Implant-assisted removable partial dentures. In: Phoenix RD, Cagna DR, DeFreest CFStewart’s Clinical Removable Partial Prosthodontics 2008 4th edHanover Park, ILQuintessence Publishing:259-77. [Google Scholar]
[9]. Chikunov I, Doan P, Vahidi F, Implant-retained partial overdenture with resilient attachmentsJ Prosthet Dent 2008 17:141-8. [Google Scholar]
[10]. Ohkubo C, Kobayashi M, Suzuki Y, Effect of implant support on distal-extension removable partial dentures: in vivo assessmentInt J Oral Maxillofac Implants 2008 23:1095-101. [Google Scholar]
[11]. Kim JH, Lee JH, An implant supported removable partial denture on milled bars to compromise the inadequate treatment plan: a clinical reportJ Adv Prosthodont 2010 2(2):58-60. [Google Scholar]
[12]. Gates WD, Cooper LF, Sanders AE, Reside GJ, De Kok IJ, The effect of implant-supported removable partial dentures on oral health quality of lifeClin Oral Implants Res 2014 25(2):207-13. [Google Scholar]
[13]. Wolfart S, Moll D, Hilgers RD, Wolfart M, Kern M, Implant placement under existing removable dental prostheses and its effect on oral health-related quality of lifeClin Oral Implants Res 2013 24(12):1354-9. [Google Scholar]
[14]. Gonçalves TM, Campos CH, Gonçalves GM, de Moraes M, Mastication improvement after partial implant-supported prosthesis useDent Res 2013 92(12):189S-94. [Google Scholar]
[15]. Carpenter JF, Implant-assisted unilateral removable partial denturesDent Today 2014 33(1):106:108-11. [Google Scholar]