A Rare Case of Accidental Esophageal Perforation in an Extremely Low Birth Weight Neonate
Pradeep Suryawanshi1, Amit Dahat2, Rema Nagpal3, Nandini Malshe4, Vijay Kalrao5
1NICU Incharge, Associate Professor & Consultant Neonatologist, Division of Neonatology, Department of Pediatrics,Bharati Vidyapeeth University Medical College,Pune, MS , India.
2Neonatal Fellow, Division of Neonatology, Department of Pediatrics,Bharati Vidyapeeth University Medical College,Pune, MS , India.
3Assistant Professor, Division of Neonatology, Department of Pediatrics,Bharati Vidyapeeth University Medical College,Pune, MS , India.
4Associate Professor & Consultant Neonatologist, Division of Neonatology, Department of Pediatrics,Bharati Vidyapeeth University Medical College,Pune, MS , India.
5Professor, Department of Pediatrics,Bharati Vidyapeeth University Medical College,Pune, MS , India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pradeep Suryawanshi , D 404, Treasure Park, Sant Nagar Parvati, Pune-411009, India.
Phone: +91-9923540500,
E-mail:drpradeepsuryawanshi@gmail.com
Spontaneous perforation of esophagus in neonates is a rare occurrence. However iatrogenic perforation of the esophagus is not that uncommon, and is most frequently seen in preterm and low birth weight infants. In premature infants, an esophageal perforation (EP) mainly occurs while inserting an orogastric tube. The commonly reported symptoms of EP are sudden onset respiratory distress, due to the pleural effusion and pneumothorax. In our case neonate presented with apnea requiring ventilation. We present a rare case of an Extremely Low Birth Weight (ELBW) neonate with an iatrogenic esophageal perforation who presented with recurrent apneas, outlining aspects of diagnosis and management.
Apnea, ELBW, Orogastric tube
Case Report
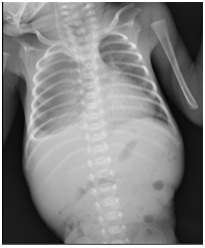
A female newborn weighing 860 gm was delivered by spontaneous vaginal delivery at 26 weeks of gestation. The baby cried immediately after birth and was shifted to a tertiary care hospital NICU for further management, where she received initial supportive care. On Day 17 of life, after insertion of 5 French orogastric tube, the baby’s condition suddenly worsened, and she developed recurrent episodes of apnea requiring mechanical ventilation. A chest radiogram showed the orogastric tube in the right pleural space with a right sided pleural effusion [Table/Fig-1a] . On all previous radiographs, the orogastric tube had been properly positioned. The orogastric tube was removed and a new 5 Fr orogastric tube was reinserted and positioned appropriately, and confirmed both clinically and radiologicaly. The patient was thereafter managed conservatively with no further complications. A radiological dye study was performed 8 days later which showed no leak in esophagus [Table/Fig-1b] , and the baby was gradually weaned off respiratory support. Feeds were reintroduced & gradually increased to full feeds, which were well tolerated, and she was discharged on Day 74 of life.
Chest radiographs showing orogastric tube in right sided pleural space and Pleural effusion
A radiological dye study performed 8 days later shows no leak in esophagus

Discussion
Traumatic perforations of the pharyngo-oesophageal region in the newborn were first reported by Elkof et al., [1]. Since then, it has been increasingly mentioned as a possible complication of neonatal intensive care. The neonates most at-risk are the small for gestational age (SGA) or premature infants [2]. The overall estimated incidence of iatrogenic EP is 0.8% in preterm infants. However, this incidence reaches 4% in newborns weighing <750 gm [3]. Vigorous suctioning of the nasopharynx and oropharynx, repeated attempts to insert nasogastric tubes and endotracheal tubes have been reported as the most common causes of injury [1]. Spontaneous rupture of the oesophagus, secondary to asphyxia and oesophagitis have also been reported [4]. In the above reported case, the esophageal perforation occurred secondary to insertion of a 5 French orogastric tube.
A majority of studies suggest that sudden respiratory distress, secondary to a pneumothorax or hydrothorax is the most common presentation [1,4,5-9]. However, our baby presented with recurrent apnea requiring mechanical ventilation. The diagnosis of EP is made by identifying a malposition of orogastric tube in the pleural cavity. A plain chest radiograph suffices in usual EP cases [4]. A lateral view, taken at the same time, is also helpful for the diagnosis [10].However; a contrast study of oesophagus adds little information [5].Neonates with iatrogenic pharyngo-oesophageal perforation should be treated according to the severity and presentation in each individual case. Removal of the nasogastric tube, initiation of broad spectrum antibiotics and provision of parenteral nutrition /gastrostomy feeds for 7–10 days provides adequate treatment in most cases [9,11]. Most babies can be treated conservatively although surgical intervention may be required in severe cases [11,12].There is no difference in the reported rate of survival when treated medically versus surgically [9]. Routine surgical intervention does not improve the survival and should be restricted for patients with mediastinitis or mediastinal mass [9]. In our case, conservative management was successful.
In conclusion, EP is a rare complication in the modern neonatal intensive care setting, but can occur even in most experienced hands.It is associated with significant morbidity or mortality. A high index of suspicion is warranted in infants with a sudden deterioration of respiratory status, especially following procedures involving the pharyngeal region. Radiological investigation is required for the diagnosis. Furthermore, we need to be cautious when an orogastric tube is inserted in ELBW neonates.
[1]. PA Cairns, BG McClure, HL Halliday, M McReid, Unusual site for oesophageal perforation in an extremely low birth weight infant.Eur. J. Pediatr 1999 158:152-3. [Google Scholar]
[2]. HA Al-Khawahur, AH Al-Salem, Iatrogenic perforation of the esophagusSaudi Med J. 2002 23(6):732-4. [Google Scholar]
[3]. L Filippi, M Pezzati, C Poggi, Use of polyvinyl orogastric tubes and iatrogenic pharyngo-oesophageal perforation in very low birth weight infantsActa Paediatr 2005 94:1825-8. [Google Scholar]
[4]. M Grünebaum, C Horodniceanu, E Wilunsky, S Reisner, Iatrogenic transmural perforation of the esophagus in the preterm infant.Clin Radiol 1980 31:257-61. [Google Scholar]
[5]. PS Shah, MS Dunn, VS Shah, Esophageal perforation in preterm neonates: not aninnocent bystander.J Paediatric Child Health 2003 39:697-9. [Google Scholar]
[6]. SK Singh, S Taneja, RD Singh, Unusual presentation of an iatrogenic esophageal perforation in a new born.Indian J Pediatr 2005 72(87) [Google Scholar]
[7]. E Sapin, L Gumpert, A Bonnard, E Carricaburu, E Sava, P Contencin, Iatrogenic pharyngoesophageal perforation in premature infantsEur J Pediatr Surg. 2000 10:83-7. [Google Scholar]
[8]. VR Kairamkonda, A rare cause of chylo-pneumothorax in a preterm neonateIndian J Med Sci. 2007 61:476-7. [Google Scholar]
[9]. DE Johnson, J Foker, DP Munson, A Nelson, P Athinarayanan, TR Thompson, Management of esophageal and pharyngeal perforation in the new born infantPediatrics 1982 70:592-6. [Google Scholar]
[10]. BH Su, HY Lin, HY Chiu, HC Lin, Esophageal perforation: a complication of nasogastric tube placement in premature infants.J Pediatr 2009 154(460):460-e1. [Google Scholar]
[11]. DL Mollitt, N Schullinger J, V Santulli T, Selective management of iatrogenic esophageal perforation in the newbornPediatr Surg 1981 16:989-93. [Google Scholar]
[12]. IH Krasna, D Rosenfeld, BG Benjamin, G Klein, M Hiatt, T Hegyi, Esophageal perforation in the neonate: an emerging problem in the newborn nurseryJ Pediatr Surg. 1981 16(6):989-93. [Google Scholar]