In and around Ammapettai, a rural area with an economically backward community, 515 cases were operated for prolapsed uteri, by doing modified pelvic floor repairs (Dr. Sunthanthradevi’s method), without any incidence of vault prolapse, with patients being followed up for two years after their surgeries.
Fungal, Allergic, Charcot, Charcot, Charcot
Introduction
Gynaecological problems, particularly prolapse of uterus, in women of a rural and economically backward community, was taken into account. Surgery was chosen as the definite line of treatment. The diagnosed cases included postmenopausal women- 80% and those who were in post child bearing period-20%.
Aim
To study the incidence of prolapse in different age groups, parity, degree of prolapse, working pattern, duration and medical complications.
To prevent the descent of vault of the vagina in the post vaginal hysterectomy patients by new surgical method.
Materials and Methods
A total number of 748 patients who belonged to the rural population which resided in and around Ammapettai, Kancheepuram district, underwent different gynaecological surgeries within three years (from 2009 to 2012). Out of these, 515 patients with prolapsed uteri were selected. Surgery which was done was vaginal hysterectomy, with anterior colporraphy and colpoperiniorraphy.
In order to achieve complete surgical reconstructions in pelvic floor disorders, followed by routine vaginal hysterectomy, a new method which was called MODIFIED PELVIC FLOOR REPAIR, which was introduced by Dr. SUTHANTHIRADEVI, is being practised in patients who undergo vaginal hysterectomies.
After the removal of the uterus by routine vaginal hysterectomy, peritoneum is closed by extra peritonization of the pedicles by using purse string suture. Subsequently, anterior colporraphy is done by Kelly’s method Routinely, the vault is closed in the transverse position after doing Kelly’s procedure and then, a pelvic floor repair is done. In this modified step, anterior colporraphy is done without closing the vault and it is stopped in the middle. Routine pelvic floor repair is done with approximation of levator ani and closure of the pelvic floor apex is continued upwards to middle portion, where the anterior colporraphy is stopped in a vertical manner. This was done in 515 patients and patients were followed up for two- three years after their surgeries.
Technique which was Involved
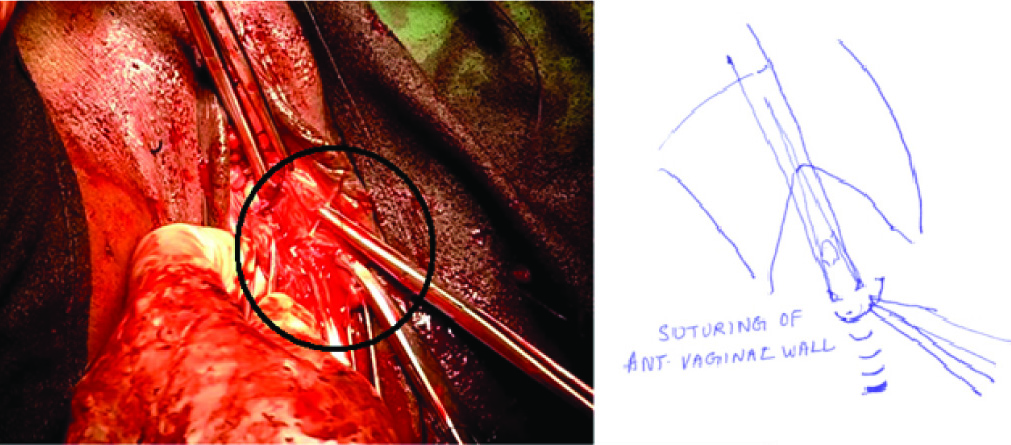
• Anterior wall closure done vertically – and vault done transversely with PFR was the routine method which had been adapted so far. A defect which occurred in this method was pericervical tissue laceration and apical gaping in the vault area, which caused a post-operative vault prolapse. Modification which was done here was stoppage of anterior wall closure[Table/Fig-1].
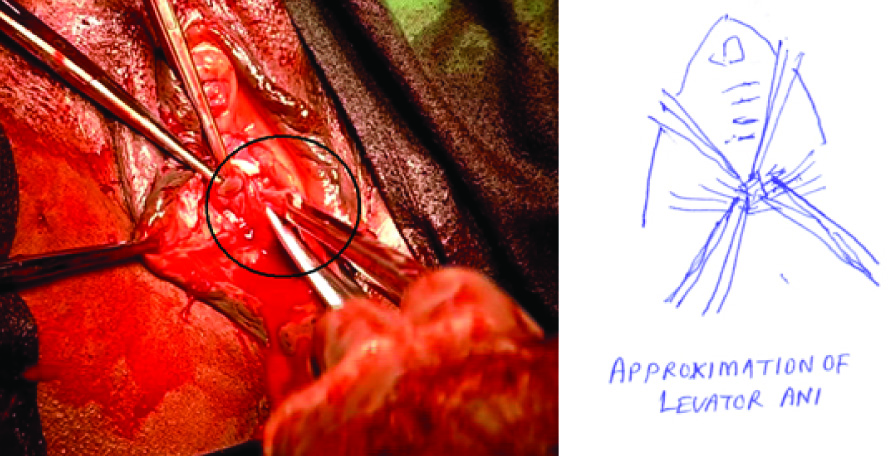
• Next PFR was started [Table/Fig-2] as usual, but extensive dissection of ischiorectal fossa was not done – which produced a big defect laterally.
• Tying the levator [Table/Fig-3], approximated together by using H shaped suture - gave more strength at the posterior vaginal wall [Table/Fig-2].
• The excess vaginal wall was excised posteriorly.
• The stay suture which was left in the anterior vaginal wall was lifted up. There was a canulated conical defect. If this defect is not identified and closed properly, it will definitely cause vault prolapse.
• The same was sutured and the defect was obliterated – this is an important step in this surgery.
• Connecting the anterior vaginal wall, with posterior up to apex of the pelvic floor in vertical manner, will obliterate pericervical area and prevent pericervical tissue gap and weakness, thereby preventing vault prolapse [Table/Fig-4].
• All the particulars of the patients after surgery regular follow ups were carried out for three years. Complications were also tabulated with 100% success, as far as the prevention of vault prolapse was considered
Observations
Seven hundred and forty eight patients underwent different gynaecological surgeries. They have been listed in [Table/Fig-5].
Prolapsed uteri were common in age group of 56-65 years [Table/Fig-6].
Remaining two cases had vault prolapse among a total of 515 cases. Prolapsed uteri were commonly observed in females who were Para 3 [Table/Fig-7].
A majority of patients who underwent surgeries for prolapse had 3rd degree uterine prolapses with cystoceles and rectoceles [Table/Fig-8].
Most of the patients who had undergone vaginal hysterectomies for prolapses were anaemic [Table/Fig-9].
A majority of patients who had prolapses were field workers [Table/Fig-10].
Anterior vaginal colporaphy proceeded. I tis stopped at the level of cervical region
PFR started and levator ani approximated together by H-shaped structure to give more strength at the posterior vaginal wall
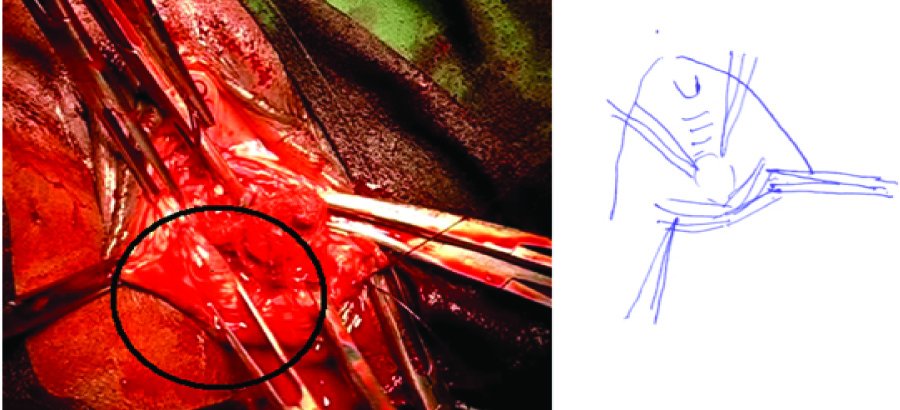
I & II continued so that the pericervical tissue are included and the space is obliterated the suture is continued with the Anterior colporaphy as a vertical suture

Indication for surgeries were given
| S.No | Diagnosis | No of cases |
| 1 | Prolapse Uterus | 515 |
| 2 | Fibroid Uterus | 84 |
| 3 | DUB | 97 |
| 4 | Adenomyosis | 21 |
| 5 | Pyometra | 1 |
| 6 | Endometrial Cancer | 1 |
| 7 | Endometriosis | 5 |
| 8 | Ovarian Problems | 12 |
| 9 | Recanalisation | 12 |
| TOTAL | 748 |
Age wise particulars for female with prolapse
| Age group | No of cases |
| 30-40 yrs | 35 |
| 41-50 yrs | 75 |
| 51-55 yrs | 115 |
| 56-65 yrs | 180 |
| 66-75 yrs | 100 |
| 76-80yrs | 08 |
| Total | 518 |
| Para | No of cases |
| Para 2 | 35 |
| Para 3 | 305 |
| Para 4 and more | 175 |
| Total no of cases | 515 |
Degree of Prolapse in the group
| Degree of prolapse | No of cases |
| procendentia | 70 |
| 3rd degree cystocele and rectocele | 315 |
| 2nd Degree cystocele and rectocele | 110 |
| 1st degree with big cystocele and rectocele | 20 |
| Total cases | 515 |
Medical complication in the group
| Medical complications | No of cases |
| Diabeted Nlallitus | 30 |
| Hypertension | 25 |
| Anaemia | 245 |
| Anaemia | 215 |
| Total | 515 |
Working pattern of the case group
| Working pattern | No of cases |
| a. Field workers. - Heavy weight lifting - Hard field work | 90% |
| b. House hold of work | 10% |
| Total | 100% |
| Duration | Percentage |
| 10- 15 yrs | 14% |
| 6 - 10 yrs | 22% |
| Less than 5 yrs | 74% |
Complications due to prolapsed
| Problems | Percentage |
| Urinary problem | 90% |
| Bowel problem (constipation) | 5% |
| Difficulty in walking | 60% |
| General discomfort | 100% |
Previous surgical status in the group
| Previous surgeries | No of cases |
| Previous LSCS | 10% |
| Sterilization done | 20% |
| Not sterilized | 70% |
| Total | 100% |
| Duration | No of cases |
| < 1 hr | 375 |
| 1-1 1/2hr | 80 |
| 2 hr | 60 |
| Total | 515 |
Post-operative complications
| Post-operative complication | No of cases |
| UTI | 3 |
| Kinking of the ureter | 4 |
| Insensitive bladder | 1 |
| Bladder injury (during surgery) | 2 |
Menopausal status
Most of the patients who had prolapses were post menopausal (480 out of 515 cases) and the durations of the prolapses have been shown in [Table/Fig-11].
Some of these patients had undergone some surgeries earlier. Most of the patients who had prolapses had not been sterilized [Table/Fig-12,13].
Type of Anaesthesia which was Given
Spinal anaesthesia was given to all 515 patients. Durations of the surgeries have been given in [Table/Fig-14] and the post-operative complications have been enumerated in [Table/Fig-15].
Discussion
Mc Call’s [1] culdoplasty involves the uteroscaral ligaments in the vault and posterior vaginal wall repair, though it had marked an improvement in the present procedure. Vault prolapse had not occurred in any of the cases. Zimmerman [2] had used a mesh to repair the vault. Lemack et al., [3] had used levartor ani to prevent vault prolapse and it was also used by the present author, but in a modified way, to achieve best results [4].
Conclusion
Post menopausal and multi parous women who do hard field work and anaemic patients develop prolapsed uteri more than other women.
This article was presented to reveal the common occurrences seen in women in this area that had a high incidence of prolapsed uteri (it was more or less like an endemic problem in this place, in and around Shri Sathya Sai Medical College and Research Institute), India.
[1]. Call Mc, Posterior culdoplasty .Obstet Gynecol. 1957 10:595 [Google Scholar]
[2]. CM Zimmerman, Vaginal hysterectomy :Is still the limiting factor?OBG Management. 2006 18:21-31. [Google Scholar]
[3]. G Lemack, P Zimmern, Margulis Margulis, The Levator myorraphy repair for vaginal vault prolapse.Urology. 2000 56(6 suppl 1):50-54. [Google Scholar]
[4]. G Lemack, D Blander, V Margulis, P Zimmern, Vaginal vault fixation and prevention of enterocele recurrence. [Google Scholar]