Penile incarceration or strangulation by an encircling object is an uncommon surgical emergency. Incarceration from metallic and non-metallic object has been reported throughout the world since 1775 [1], with largest series reported in USA by Daikin [2].These objects can be plastic or metal rings [3-6], ball-bearings [7-9], nuts [10], washers [11], wedding ring [4-6],bottles [4,12],rubber bands, iron pipe [13] and even a hammer head [4,14]. A man may placed these objects for erotic or autoerotic purpose [4,15-17], to increase sexual performance [2,5,15],as self-treatment of erectile dysfunction [11]and in cases of psychiatric disturbance [4,18].
Genital incarceration with encircling object is a true surgical emergency that requires prompt decompression. Most of the surgeons and their team are unfamiliar to this type of emergency because of its unusual occurrence. Its management is challenging to the surgeons where all methods are considered in an attempt to remove the ring from an inflamed penis. The aim of this study is to outline the treatment guidelines for penile incarceration by reviewing available literature and analyzing our cases in relation to trauma grade, duration of incarceration, removal technique and outcome.
Materials and Methods
A retrospective review of seven patients who presented with penile incarceration with encircling metallic objects in surgical causality of our institute from January 2002 to December 2011 was performed. The records of these patients were analyzed with respect to age, marital status, motive, object used, who applied it, duration of incarceration, trauma grade by Bhat et al., [10] [Table/Fig-1], removal technique, removal time, anesthesia used, recovery time and complications.
Grading scales for penile incarceration
| Penile Injury Grading System By Bhat et al., [10] | Revised Grading System [5] |
| Grade | Injuries |
| Grade 1 | edema of distal penis. No evidence of skin ulceration or urethral injury | Low grade Injuries |
| Grade 2 | Distal oedema, skin and urethral trauma, corpus spongiosum compression and decreased penile sensation. |
| Grade 3 | Skin and urethral trauma, no distal sensation. |
| Grade 4 | Separation of corpus spongiosum , urethral fistula,corpus cavarnosum compression, no distal sensation. | High Grade Injuries |
| Grade 5 | Gangrene, necrosis, or complete amputation of distal penis. |
On admission, management of such a patient starts with history, general examination and local examination of penis to assess temperature, color, sensation, viability of constricted tissue and ability to void. Grading of penile injury was done. Analgesics, antibiotics, tetanus prophylaxis were given to all the patients. Foleys catheterization was done in all cases. Removal technique chosen was according to grade of penile injury, duration of incarceration and type of object used. Cases of penile incarceration with non-metallic objects were excluded from the study. Evaluation of removal technique was done according to grade of injury, duration of incarceration and type of object used.
Results
After analyzing the data of all seven patients it is found that self-sexual gratification was the most common motive (n=4), however, other motives were self-treatment for erectile dysfunction (n=1), to prolong errection (n=1) and punishment by fellow villagers (n=1) [Table/Fig-2]. Object was donned by self in five cases, by wife to prolong erection in 1 case and by fellow villagers in 1 case. As far as marital status is concerned 6 patients were married but 4 patients had not had sexual relation with their female counterparts for some time and 2 patients suffered from psychogenic erectile dysfunction. One patient was unmarried who put object by himself for autoerotic purpose as suggested by his friend. Two patients were suffered from psychogenic erectile impotence and pedophilia was found in one patient. [Table/Fig-2]. All patients presented with distal gross penile edema up to the encircling object upon the shaft of the penis [Table/Fig-3]. The age of patients ranged from 16 to 80 years (mean 46.71 years). Duration of incarceration varied from six hours to seven days. Most of the patients presented within 24 hours, however, one patient, having a grade III injury, was presented after seven days. Five patients had a grade II injury, while the one suffered with a grade I injury.
Patient profile according to history
| S.No. | Age | Motive | Applied by | Sexual life | Mental Status |
|---|
| 1 | 45 | To prolong erection | Wife | Married | Errectile dysfunction |
| 2 | 42 | Punishment | Fellow villagers | Married | Paedophilia |
| 3 | 80 | Self-sexual gratification | Self | Married (Not had sexual relationship for some time | Normal |
| 4 | 22 | Self-treatment for erectile dysfunction | Self | Married (Not had satisfactory sexual life) | Errectile dysfunction |
| 5 | 70 | Self-sexual gratification | Self | Married (Not had sexual relationship for some time | Normal |
| 6 | 16 | Self-sexual gratification | Self | Unmarried | Normal |
| 7 | 52 | Self-sexual gratification | Self | Married (Prisoner) | Normal |
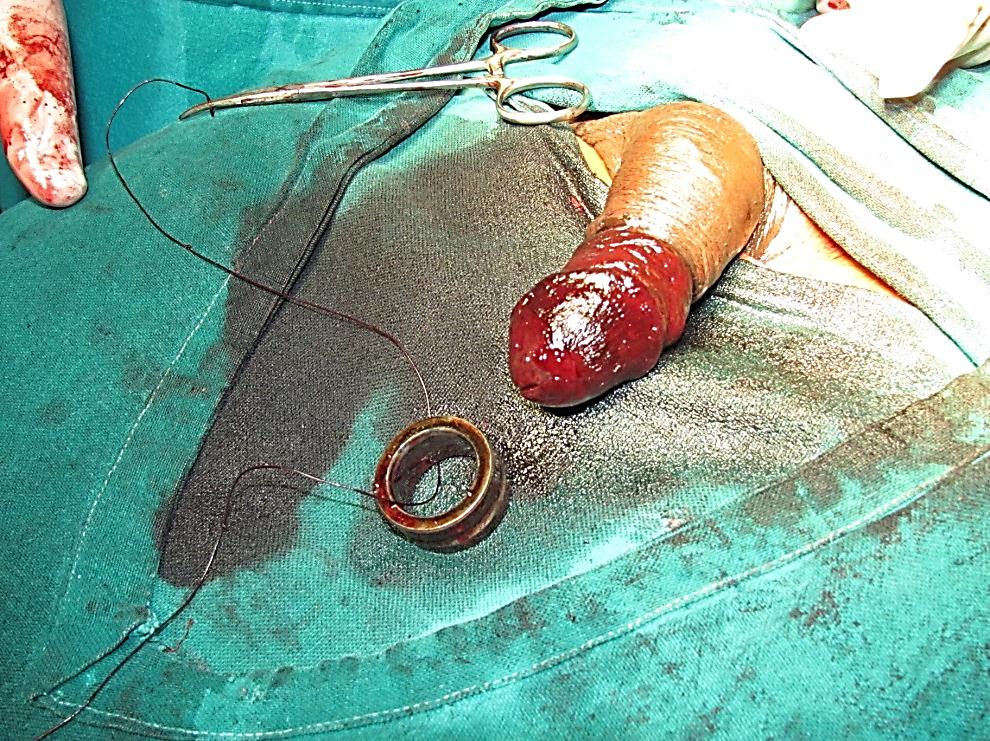
Penile incarceration due to metal ring

The technique of removal chosen was according to grade of penile injury, duration of incarceration and type of object used. String technique (Vicryl no 1, Vaseline tape gauze) with glans aspiration used in three cases [Table/Fig-4,5and6]. Cutting devices (steel saw) were used in two cases [Table/Fig-7]. Glans aspiration with hot compression to relieve distal penile edema was used in one case. Dorsal slit and removal of edematous distal prepuce skin, removal of ring and re-approximation was done in one case. Two cases required second staged procedure due to loss of penile skin secondary to necrosis, re-approximation done in one case, skin grafting done in other case. Removal time varied from 30 minutes to 100 minutes. Spinal anesthesia was used in five cases. Two cases were done under local anesthesia and sedation. Recovery time varied from two days to 21 days. One patient of grade III injury developed urethral fistula at penoscrotal junction postoperatively, and was a candidate for urethral reconstructive surgery, but did not come for follow up. Patient profile, object used, site time, grades of injury management and outcome of management are summarized in [Table/Fig-8].
Aspiration of blood from corpora cavarnosa

Removal of ring by String technique

Final appearance after removal of ring by string technique
Removal of ring by cutting device (steel saw), Knife handle
Object used, type of injury, management and outcome
| S. No. | Object used | Dimensions of object | Duration of incarceration | Grade | Removal Technique | Outcome |
|---|
| 1 | Metal Bearing | ID - 3.5cm | 6hrs | Gr.1 | Aspiration tech. with hot compression | Satisfactory |
| 2 | Metal Nut | UKN | 7days | Gr.3 | Desloughing of gangrenous skin over penis, object removal by string technique (lubricated tape gauze), | Developed skin necrosis and urethral fistula skin grafting done and candidate for urethral reconstructive surgery, but didn’t come for follow up. |
| 3 | Metal Ring | ID - 2cm | 14hrs | Gr. 2 | Cutting | Satisfactory |
| 4 | Metal Ring | ID - 2.5cm T - 4mm | 9hrs. | Gr.2 | Cutting | Minor injury to penile skin during removal |
| 5 | Metal Ring | ID - 2cm T - 8mm | 20hrs | Gr.2 | String Technique (Vicryl No1) with Aspiration | Absconded |
| 6 | Metal Bearing | ID - 3cm T - 2mm | 18hrs. | Gr.2 | Dorsal slit removal of distal prepuce skin and object re-approximation | Satisfactory |
| 7 | Metal Nut | ID - 2.5cm T - 1.5cm | 18hrs. | Gr.2 | String Technique (Vicryl No1) with aspiration | Developed skin necrosis, excision of necrotic tissue and reaproximation done later. |
ID – Internal Diameter T – Thickness UKN - Unknown
Discussion
Penile incarceration is a rare but serious problem. In adults strangulating objects are used for autoerotic purpose or to prolong erection while in adolescents they are used to increase erotic sensation during masturbation or as sexual curiosity. In infants and children common cause of penile strangulation is hair or thread which is used to prevent enuresis. Most authors did not highlight the cognitive state of their patients [5].
The placement of encircling metallic devices over the flaccid or partially erect penis results in the inability to remove them secondary to edema that developed due to prolonged period of genital entrapment, which leads to potential penile compartment syndrome with an initial obstruction to both venous and lymphatic outflow distal to device followed by arterial inflow obstruction, ultimately resulting in tissue ischemia and necrosis [17,19]. The time lapsed following penile incarceration, in which the patients presented at the hospital, ranging from three hours to 1 month [10,14,15,18].
Silberstein et al., [5] simplified grading system proposed by Bhat et al., [10] by dividing it into two broad categories. Low grade injuries corresponds to Grade 1-3 injuries and most of the time requires no further intervention after removal of encircled object, while High grade injuries corresponds to Grade 4,5 injuries and require surgical intervention [Table/Fig-1]. The types of constricting devices play a profound role in the degree of penile injury. It has been reported that nonmetallic constricting devices accounted for 77.7 % of high-grade penile injuries, while metallic objects accounted for only 22.22% [5]. The most severe injuries crop up from the non-metallic objects, but they can easily be removed by cutting the constricting device. On the other hand, it is difficult to remove metallic objects.
The method of choice for removal of encircling metallic object is dependent upon the grade of injury, material of the device, availability of the tools and surgeons experience. Treatment of urinary retention is a preliminarystep [15]. Foley’s catheter is recommended for grade I and II trauma [15], while suprapubic catheterization is recommended for grade III-V trauma [10,15,26]. Removal techniques can generally be divided into four groups [15]. String techniques with or without aspiration of blood from glans, cutting techniques, aspiration techniques, and surgical techniques.
String technique and its variants [Table/Fig-9]: The string technique was devised by Flatt [27] for removing rings from traumatized fingers. Bucy first used it in 1968 to remove a metal ball bearing from an incarcerated penis [7]. After relieving turgor a string is passed proximally beneath the ring, using remainder of the string penis bound tightly to the glans. The proximal end of the suture is lifted and unbound from the penis so that the encircling object is pushed gently over wrapped and molded penis. The series of steps may need to be repeated several times before the object can completely remove from penis [9,11,18]. Some authors have chosen to aspirate blood from glans before starting or during string procedure. Different author used different material as string such as thread, suture [8], umbilical tape [19], intravenous drip [20] and Vaseline gauze. String technique and its variants can effectively use in grade 1-3 injuries [15]. In present series this technique was used in three cases and Vicryl No. 1 was used as string in two cases while Vaseline tapes gauze in one case. According to our experience string technique with aspiration is highly effective and safe for removing metallic devices from incarcerated penis in low grade injuries. The key point is, the winding process should begin by passing a string through the encircling object.
String technique and its variants
| Author | Object | Size | Grade | Incarceration Time | Technique |
|---|
| Bucy [7] | Ball Bearing | 2cm ID 1.5cm T | 2 | 8 hrs. | Cord, glans aspiration |
| Browning and Reed [19] | Metal Ring | UKN | 3 | 3 hrs. | Umbalical tape glans drainage |
| Vahsarja et al., [18] | Loop wrench | 11 mm ID | UKN | 5 hrs. | String, glans aspiration |
| Ball Bearing | UKN | 2 | 24 hrs. | String, glans aspiration |
| Rana and Sharma [11] | 3 Washer | UKN | 1 | 14 hrs. | Spring, glans drainage |
| Noh et al., [8] | Metal Bearing | 11 mm ID | UKN | 5 hrs. | String, glans aspiration |
| Metal | 22 mm OD | UKN | 8 hrs. | String, glans aspiration |
| Bearing | UKN | | | |
| Faroqui and Meena [20] | 2 Metal Rings | 3.5 cm OD | UKN | UKN | Intravenous drip, compression |
| | 2.5 cm ID | | | |
| Present Study | Metal Nut | UKN | 3 | 7 days | Tape Gauze |
| Metal Ring | 2 cm ID | 2 | 20 hrs. | Desloughing of gangrenous skin String, glans aspiration |
| Metal Nut | 8 mm T | | | String, glans aspiration |
| | 2.5 cm ID | | | |
| | 1.5 cm T | | | |
UKN- Unknown, OD- Outer Diameter, ID, Inner Diameter, T- Thickness
Cutting devices: Cutting methods are often the first method for dividing an encircling device that cannot be removed with sequential compression. Due to diversity of encircling device various cutting devices are used by different authors. These can be 2 types: non electric cutting devices [Table/Fig-10] and electric cutting devices [Table/Fig-11]. Non-electric cutting devices like hammer and chisel [10], ring cutter [4], hack saw [23] and metal saw [4,10] are useful but they require strength to operate and they cannot cut thick metal ring. Use of various electric cutting devices like dremmel rotary tool [5,22], Anspach saw with tungsten carbide bits [9], heavy drills [10], high speed electrical steel saw [4] and pneumatic drill [17] have been reported in literature. These electrical devices are highly effective in cutting thick metal ring but it should be used with caution to prevent injury to surgeon and patients. To avoid damaging the surrounding edematous tissue a shielding device should be placed between foreign body and penis. Shielding device selected for cutting include: laryngoscope blade [5],metal tongue depressor [4], wooden tongue depressor [9],silastic guards and poly vinyl chloride plaques. Heats produced from the metal object from friction can potentially results thermal injury which can be prevented by cool water irrigation [9,10] and water sprays [26]. Metal device is either cut in two location 180o apart [9], or by one cut and scoring of device on opposite side by using an expander tool [10]. Cutting device can be combined with corpus cavarnosum aspiration so that the tumescence could be reduced to allow for easy removal of foreign body [4,10]. Grade 1-3 can be treated by this technique provided appropriate cutting tools are available [15]. In present series this technique was used in two cases,metal saw used as cutting device and knife handle used as shielding device.
Non electric cutting devices
| Author | Object | Size | Grade | Incarceration Time | Cutting Tool |
|---|
| Steiner [21] | Metal Nut | 1 cm wide | 2 | 8 days | Hacksaw |
| Bhat et al., [10] | Metal Nut | 0.5 cm T | 3 | 8 days | Hammer & Chiesel Metal |
| Metal Nut | 0.5 cm T | 3 | 5 days | Saw |
| Metal Ring | 0.3 cm T | 2 | 4 days | Metal Saw |
| Vahsarja et al., [16] | Loop wrench | 11 mm ID | UKN | 5 hrs. | String, glans aspiration |
| Ball Bearing | UKN | 2 | 24 hrs. | String, glans aspiration |
| Perabo et al., [4] | Wedding Ring | UKN | 1 | 3 hrs. | Ring Cutter |
| Metal Cuff | UKN | 1 | Earlier in the day | Metal Saw |
| Bull Ring | 33 mm wide | 1 | 3 days | Bolt Cutter |
| | 5 mm T | | | |
| Patel et al., [3] | 2 Metal radiator clamp | UKN | 2 | 6 months | Orthopedic wire cutter |
| Present study | Metal Ring | 2 cm ID | 2 | 14 hrs. | Metal Saw |
| Metal Ring | 2.5 cm ID | 2 | 9 hrs. | Metal Saw |
| | 4 mm T | | | |
UKN- Unknown, OD- Outer Diameter, ID, Inner Diameter, T- Thickness
| Author | Object | Size | Grade | Incarceration Time | Cutting Tool |
|---|
| Greenspan [22] | Steel Ring | UKN | 2 | 7 hrs. | Dremmelmoto tool with grinder |
| Snoy et al., [19] | 2 Steel brushing | UKN | 3 | 33 hrs. | Dental drill with flat carbide disk |
| McLaughin and Coyner [9] | Steel bearing | 1.9 cm wide 3mm T | 1 | UKN | Anspach saw with Tungsten carbide bits |
| Bhat et al., [10] | Ball bearing | 3 cm T | 3 | 5 days | Heavy drill |
| Perabo et al., [4] | Hammerhead | UKN | UKN | UKN | High speed electrical steel saw |
| Silberstein et al., [5] | Metal Ring on Penis & Scrotum | 6.5cm OD | 3 days | UKN | Dremmel rotating saw |
| | 4.5cm ID | | | |
| Darby et al., [17] | 7 metal rings | UKN | UKN | UKN | Midas Rex pneumatic drill |
UKN- Unknown, OD- Outer Diameter, ID, Inner Diameter, T- Thickness
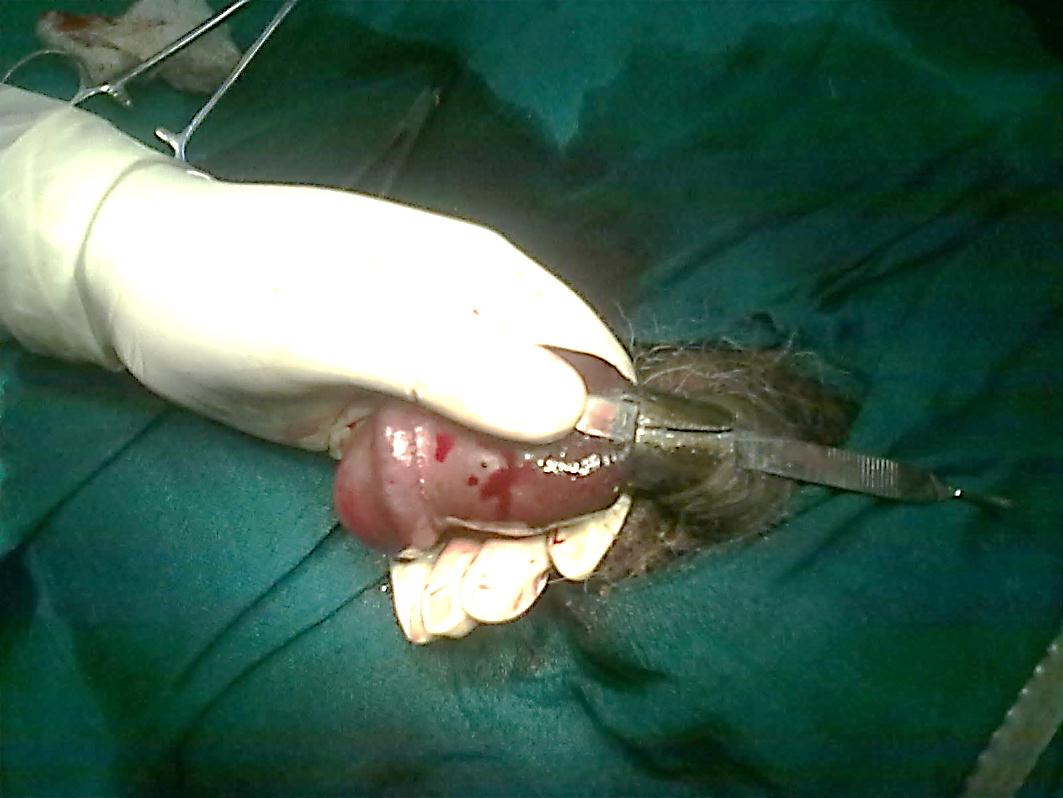
Aspiration techniques [Table/Fig-12]: De-tumescence can be achieved by placement of 18-gauge needle into the corpora or glans and aspiration of congested blood from penis [15,24]. Multiple punctures of distal penis with 18-gauge needle into subcutaneous tissue drains lymph which decreases edema and aids in removal of metal ring [15, 23]. Most of the time aspiration technique is not sufficient alone and needs to be combined with aspiration or cutting technique [5]. This technique is useful in grade 2 and 3 injuries [15].This technique was used in one case of present series.
Pure aspiration techniques
| Author | Object | Size | Grade | Incarceration Time | Technique |
|---|
| Punekar et al., [23] | Hammerhead | 1.5 cm T | 3 | 14 hrs. | Needle puncture, drainage of lymph |
| Sinha [24] | Metal Nut | 1.5 cm T | 2 | 8 hrs. | Aspiration of 66 ml of blood |
| Present Study | Metal Bearing | 3.5 cm ID | 1 | 6 hrs | Aspiration of blood |
ID, Inner Diameter, T- Thickness
Surgery [Table/Fig-13]: Surgical technique by dorsal slit, removal of edematous prepuce skin or degloving with circumcoronal incision, retrieval of ring and subsequent approximation can be used in grade 2-3 injuries [12,13,16,25], concurrent or delayed skin grafting can be done if defect is large due to skin excision. Advanced grade injuries can be treated with wide tissue debridement of devitalized tissue and partial thickness cutaneous graft. Penile amputation with re-implantation using microsurgical technique for grade IV and V has been suggested [28]. In case of gangrene of penis partial or total amputation of penis can be done [12].
| Author | Object | Size | Grade | Incarceration Time | Technique |
|---|
| Schellhammer & Donnely [13] | Iron pipe | UKN | 5 | 6.5 days | Degloving of penis up to Buck’s fascia |
| Klein & Smith [25] | Ball bearing | UKN | 5 | 7 days | Degloving of penis up to Buck’s fascia |
| Wasadikar [14] | Metal ring | 1.4 cm ID | 2 | 30 days | Excision up to Corpus Cavernosum |
| Ivanovski et al., [12] | Steel ring | 3 cm OD | 2 | UKN | Wide excision of affected skin |
| | 3 mm T | | | |
| Baruah & Bagchi [14] | Metal Ring | UKN | 2 | 17 hrs. | Wide excision of affected skin & Reapproximation |
| Present Study | Metal Bearing | 2.5 cm ID | 2 | 18 hrs. | Wide excision of affected skin & Reapproximation |
| | 1.5 cm T | | | |
UKN- Unknown, OD- Outer Diameter, ID, Inner Diameter, T- Thickness
Penis should be examined thoroughly after removal of metal ring to ascertain any vascular or irreversible tissue injury. If there is any doubt color Doppler may help in determining the vascular patency and may rule out thrombosis or rupture of vasculature [5]. Heparinization can be considered if distal pulsations are absent on Doppler study. Hospitalization and repeat examination are essentially recommended,because secondary infection and skin necrosis develop days after removal of the metal ring.
Complications are directly related to duration and grade of incarceration include: urinary retention [9,10,26], urethral stricture [10], urethral fistula [10], skin ulcerations [10]; decreased or loss of penile sensation [10,17], priapism [10,26], gangrene of penile skin and subcutaneous tissue [12], gangrene of penis [12]. Complications noted in two patients of our series were skin necrosis and urethral fistula.
Following removal of the encircling devices urethral stricture is potential complication and can be ruled out with follow-up imaging [10,26]. Long term follow-up with micturating cysto-urethrogram and uroflowmetry is necessary [16]. Psychiatric evaluation and counseling of patients against such experimental practices on their penis is also required. Follow-up is poor because of most of the patients are feeling embarrassed and do not want to disclose the incidence.
Conclusion
Penile incarceration with encircling devices is an unusual clinical condition and consequences can be severe. Prompt recognition, urgent decompression of involved tissue by removing encircling object is required to prevent potential complication. Numerous removal techniques have been described in literature, but every case needs individual approach depending on the patient presentation, type of encircling object and facilities available.
ID – Internal Diameter T – Thickness UKN - Unknown
UKN- Unknown, OD- Outer Diameter, ID, Inner Diameter, T- Thickness
UKN- Unknown, OD- Outer Diameter, ID, Inner Diameter, T- Thickness
UKN- Unknown, OD- Outer Diameter, ID, Inner Diameter, T- Thickness
ID, Inner Diameter, T- Thickness
UKN- Unknown, OD- Outer Diameter, ID, Inner Diameter, T- Thickness