Objectives: To study the microbial flora and determine the efficacy of topical ciprofloxacin ear drops in comparison with combination of topical and oral ciprofloxacin as first line management in patients diagnosed with chronic suppurative otitis media.
Materials and Methods: Prospective randomized interventional clinical trial on 100 patients who presented with an acute episode of CSOM to our outpatient department.
Results: In our study, topical ciprofloxacin therapy was found to be an effective treatment for an acute on chronic otitis media as was the combination therapy though the overall recurrence rate was found to be more in the former group.
Conclusion: In the absence of systemic infection or serious underlying disease, topical antibiotics alone constitute first line treatment for most patients with chronic suppurative otitis media, finding no evidence that systemic antibiotics alone or in combination with topical preparations improve treatment outcomes compared with topical antibiotics alone.
Introduction
The incidence of chronic suppurative otitis media (CSOM) appears to depend on race and socio-economic factors. Socio-economic factors such as poor living conditions, overcrowding, poor hygiene and nutrition have been suggested as a basis for the wide spread prevalence of CSOM [1] .
Changes in the microbiological flora following the advent of sophisticated synthetic antibiotics increase the relevance of reappraisal of the modern day flora in CSOM and their in vitro antibiotic sensitivity pattern is very important for the clinician to plan a general outline of treatment for a patient with a chronically discharging ear [2].
There is a growing concern over the use of systemic antibiotics and the development of bacterial resistance. The question remains as to whether ototopical medications may also promote antibiotic resistant organisms on a local level in the ear. This study has been undertaken prompted by rising rates of antibiotic resistance in our country.
The present study is aimed at finding the organisms responsible for CSOM by taking the ear swab for culture and sensitivity and by treating the patient with topical / combination ciprofloxacin. The response to the treatment is studied and analyzed.
Materials and Methods
This is a time bound cross sectional study done on 100 patients who presented to the Ear Nose Throat (ENT) Out patient Department (OPD) at a tertiary health centre from October 2012 to September 2013, with an acute episode of CSOM. They were carefully selected with respect to the inclusion and exclusion criteria over the study period [Table/Fig-1]. Patients with active ear discharge [Table/Fig-2]. who are eligible for the study were counseled about their condition and an informed consent was obtained for the study.
Inclusion criteria
Patients presenting to ENT OPD above 18-years of age with:
• Mucopurulent or purulent otorrhea of more than 3weeks duration with a tympanic membrane perforation.
• Patients who have antibiogram revealing sensitivity to ciprofloxacin.
Exclusion criteria
• Acute (< 21 days) perforation of tympanic membrane (Acute otitis media)
• Known allergy to quinolone or benzalkonium chloride (preservative)
• Underlying chronic diseases such as Diabetes mellitus,
Tuberculosis
• Known case of immunodeficiency.
• Atticoantral type of chronic suppurative otitis media
• Otomycosis
• Impending complications
• Large aural polyp in the middle ear
• Have used any antibiotic therapy in target ear in the past month
• Otological surgery within the past year
• Presence of tympanostomy tube
• Acute traumatic perforation
• Pregnant or lactating mother
• Symptomatic conditions such as otitis externa , chronic sinusitis, chronic pharyngitis requiring systemic antibiotic therapy that could interfere with the evaluation of study drugs
• Known hepatitis or acute or chronic renal failure
The patients were then allotted to their respective groups by random sampling method (Picking one of the 2 coloured coins) as:
GROUP A (Red): Topical ciprofloxacin ear drops therapy for two weeks.
GROUP B (Green): Combination of topical and oral ciprofloxacin for two weeks.
At the first visit of each patient, a pretested proforma was used to record the relevant information of each individual included in the study. The aural discharge was collected with a conventional sterile swab preventing contact with the external auditory canal using a sterilized aural speculum. The specimens was immediately taken to the microbiology test laboratory. The samples was first put into a glucose broth and subsequently inoculated into blood agar (enriched medium) and Mac Conkey agar (differential medium) following which they were cultured for 24hours. The primary colony of the cultured bacteria was identified by Gram stain and biochemical tests. Culture and sensitivity of isolates was determined by the Kirby–Bauer disk diffusion method [Table/Fig-3].
Each patient was then randomly assigned to a study group by means of a lot. In Group A, Ciprofloxacin ear drops (3 drops) was to be used thrice a day for 14 days in the affected ear. In group B, a combination of topical Ciprofloxacin (3drops) thrice a day and tablet Ciprofloxacin (500mg) twice a day was to be administered for 14 days.
Patients was asked to prevent water entry into affected ear and dry mopping before instilling the ear drops. The right technique of instilling with intermittent tragal pressure was advised.
At the patient’s next visit, two weeks post-treatment, compliance was assessed and defined by the number of times the patient forgot to use the drug within the two weeks: Good (0-3), Moderate (4-7), Poor(>7) [3]. Non compliant patients (moderate and poor) were substituted by new cases to meet the sample size. A detailed assessment of the ear discharge was done subjectively and objectively [Table/Fig-4] and repeat ear culture and sensitivity test was performed if drainage was still present [Table/Fig-5a,5b].
“CURED” [4] was defined as the absence of otorrhea or otoscopically inactive (no pooling of discharge; non inflamed middle ear mucosa) or the presence of a serous mucous otorrhea with negative bacteriological culture after the treatment period.
Two weeks post-treatment, the patients of either group who were ‘cured but still having persistent otorrhea’ was continued for one more week on supportive anti inflammatory agents and reviewed at the end of the 3rd week [Table/Fig-6].
Two weeks post-treatment, the patients of GROUP A who were not cured were made to continue Ciprofloxacin ear drops (if still sensitive to ciprofloxacin) or changed to a systemic antibiotic (if no longer sensitive to ciprofloxacin) for one more week and evaluated at the end of the 3rd week [Table/Fig-7]. The latter was termed as “CLINICAL FAILURE”. At the 3rd visit if the patients who continued the ear drops were still not relieved of otorrhea, they were classified as a “CLINICAL FAILURE” and changed to a systemic antibiotic according to the culture and sensitivity test report.
Two weeks post treatment, the patients of GROUP B who were not cured were asked to continue the combination therapy (if sensitive to ciprofloxacin) or changed to a systemic antibiotic (if no longer sensitive to ciprofloxacin) for one more week and evaluated at the end of the 3rd week. The latter was termed as “CLINICAL FAILURE”. At the 3rd visit if the patients who continued the ciprofloxacin combination treatment were not relieved of otorrhea [Table/Fig-8]they were classified as “CLINICAL FAILURE” and changed to another systemic antibiotic (taken alone) according to the culture and sensitivity test report.
Excluding the candidates who were cured or taken up for surgery, all the other patients were followed up at the 8th week for resolution or recurrence of symptoms [Table/Fig-9].
The post-treatment clinical and bacteriological improvement were subject to appropriate analysis. Categorical data were analysed by χ2 test and Z-test for proportions between the two groups.
The criteria of withdrawal was failure to follow up or intolerance to the study medication.
| Age in years | No.of patients | Percentage |
| 20-29 | 51 | 51 |
| 30-39 | 23 | 23 |
| 40-49 | 9 | 9 |
| 50-59 | 11 | 11 |
| 60-69 | 6 | 6 |
| Total | 100 | 100 |
| Ear Discharge | No.of patients | Percentage |
| Duration (years) |
| 1-5 | 66 | 66 |
| 6-10 | 19 | 19 |
| >10 | 15 | 15 |
| Amount |
| Scanty | 13 | 13 |
| Moderate | 23 | 23 |
| Profuse | 64 | 64 |
| Character |
| Mucoid | 96 | 96 |
| Purulent | 4 | 4 |
Bacterial isolated in ear discharge
| Group A | Group B |
| Present | 18 (36%) | 20 (40%) |
| Absent | 32 (64%) | 30 (60%) |
| Chi-square 0.17, p-value 0.91, NS |
| Culture | Group A | Group B |
| Klebsiella | 9 (18%) | 5 (10%) |
| Staphylococcus aureus | 3 (6%) | 4 (8%) |
| Pseudomonas | 2 (4%) | 1 (2%) |
| Proteus | 2 (4%) | 0 |
| E-coli | 1 (2%) | 0 |
| No growth | 15 (30%) | 20 (40%) |
| Not done | 18 (36%) | 20 (40%) |
| Sensitivity | Group A | Group B |
| Positive | 10 (20%) | 5 (10%) |
| Negative | 7 (14%) | 5 (10%) |
Result after 2 weeks of treatment
| Group A | Group B |
| Cured | 18 (36%) | 20 (40%) |
| Improved | 25 (50%) | 25 (50%) |
| Failed | 7 (14%) | 5 (10%) |
| Chi-square : 0.44, p-value 0.80, NS |
Plan after two weeks of treatment
| Group A | Group B |
| One more week of antibiotics | 10 (20%) | 4 (8%) |
| Supportive treatment | 15 (30%) | 21 (42%) |
| Change to higher antibiotics | 7 (14%) | 5 (10%) |
| Group A | Group B |
| Present | 6 (12%) | 2 (4%) |
| Absent | 25 | 25 |
| Chi-square : 2.17, p-value 0.14, NS |
| Group A | Group B |
| Non recurrent | 31 (62%) | 46 (92%) |
| Recurrent | 19 (38%) | 4 (8%) |
| Chi-square : 12.71, P-value 0.00, HS |
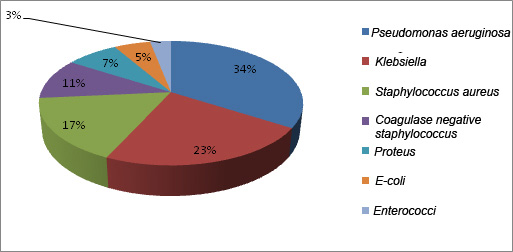
Showing the commonest bacterial organisms isolated in various studies
*NA - Not available
| Commonest isolate | Second commonest isolate | Third commonest isolate |
| Loy et al., [4] | Pseudomonas aeruginosa (33.3%) | Staphylococcus aureus (33.3%) | Coagulase negative staphylococcus (21.1%) |
| Gul et al., [5] | Pseudomonas aeruginosa (52.2% | Staphylococcus aureus (15%) | Proteus (6.5%o) |
| Poorey et al., [6] | Pseudomonas aeruginosa (35.2%) | Klebsiella aerogincs (25.4%) | Staphylococcus aureus (14.7%) |
| Ettehad et al., [3] | Staphylococcus aureus (31.5%) | Pseudomonas aeruginosa (26.23%) | Proteus (19.67%) |
| Present study | Pseudomonas aeruginosa (35.48%) | Staphylococcus aureus (21.5%) | Klebsiella (13.97%) |
Comparison of various treatment options
| Study | Drugs administered | Percentage of patients with dry ears |
| Kasemsuwan et al., [10] | Ciprofloxacin eardrops | Ciprofloxacin -84% Controls-12,5% |
| Macfadyen et al., [11] | Ciprofloxacin ear drops Tobramycin ear drops | Ciprofloxacin-47.4% Tobramycin-23.5% |
| Jaya et al., [12] | Ciprofloxacin ear drops Povidone iodine ear drops | Ciprofloxacin -90% Povidone iodine -88% | | |
| Eposito et al., [13] | Ciprofloxacin oral Ciprofloxacin topical | Ciprofloxacin oral-40% Ciprofloxacin topical-85% |
| Present study | Ciprofloxacin ear drops Combination of oral and topical ciprofloxacin | Ciprofloxacin ear drops-64% Combination Ciprofloxacin60% |
Results
This study was conducted in patients above 18-years and they were found to be between age groups of 20 to 69 years. Out of 100 patients, 60 (60%) were males and 40 (40%) patients were females. 67 patients had unilateral CSOM and 33 patients had bilateral CSOM. Hence the total number of ears studied were 133.
In the study population Pseudomonas aeruginosa is the most common organism isolated in 45 patients followed by Klebsiella in 30 patients [Table/Fig-10]. The organisms were all sensitive to Ciprofloxacin.
Discussion
The topical antibiotics were found to be as effective as oral antibiotics. A vastly higher concentration of antibiotic solution can be delivered to the site of infection by topical administration [7]. The bactericidal and lethality of bactericidal kill of quinolones is progressively enhanced by 3the extent to which the delivered concentration exceeds the minimum inhibitory concentration (MIC). The possibility for the emergence seems to be vastly lower when topical routes of administration are used as compared with drugs that are administered systemically [8]. Further the use of topical agents allows for the simultaneous modification of the local microenvironment. The administration of an antibiotic in an acidic medium helps restore and fortify the normal host defence mechanism, therefore increase efficacy of antibiotics used [9]. Another character of topical delivery systems is the absence of systemic effects. Because no appreciable systemic delivery of topically administered agents occurs, the normal flora in the respiratory and gastrointestinal tracts is not exposed to antibiotics [3]. Ototopical antibiotics are generally less expensive than systemic medications, therefore reduces the cost of treatment [Table/Fig-11].
Oral antibiotics can be of immense use when the systemic effect of antibiotic is desired like in patients of CSOM with concomitant acute or chronic rhinosinusitis, adenotonsillitis, pharyngitis and upper respiratory tract infection [14].
Conclusion
In my study, Pseudomonas aeruginosa was the most common organism isolated followed by Klebsiella. Topical ciprofloxacin was found to be as effective as combination of oral and topical ciprofloxacin ear drops though the chances of recurrence was found to be more when topical ear drops was used as the sole agent in the first line management of discharging chronic supportive otitis media.
[1]. M Kiris, M Berktas, E Egeli, The efficacy of topical ciprofloxacin in the treatment of chronic suupurative otitis media.Ear Nose Throat J. 1998 20(77):904-5. [Google Scholar]
[2]. SM Wintermeyer, Efficacy of ototopical ciprofloxacin in paediatric patients with otorrhea.American Academy of Otolaryngology – Head and Neck Surgery. 1997 116(4):450-3. [Google Scholar]
[3]. GH Ettehad, S Refahi, A Neemati, A Pirzadeh, A Daryani, Microbial and antimicrobial susceptibility patterns from patients with chronic otitis media in Ardebil.International Journal of Tropical Medicine. 2006 1(2):62-5. [Google Scholar]
[4]. JM Loy, AL Tan, PKS Lu, Microbiology of chronic suppurative otitis media in Singapore.Singapore Medical Journal. 2002 43(6):296-99. [Google Scholar]
[5]. AA Gul, L Ali, E Rahim, S Ahmed, Chronic suppurative otitis media – frequency of pseudomonas aeruginosa in patients and its sensitivity to various antibiotics.Professional Medical Journal. 2007 13(3):411-15. [Google Scholar]
[6]. VK Poorey, A Iyer, R Kalra, Study of bacterial flora in CSOM and its clinical significance.Indian Journal of Otolaryngology and Head and Neck Surgery. 2002 54(2):91-5. [Google Scholar]
[7]. P Supiyaphun, K Tonsakulrungruang, L Chochaipanichnon, The treatment of chronic suppurative otits media and otits externa with 0.3 % ciprofloxacin otic solution:a clinicomicrobiological study. J Med Assoc Thai. 1995 78:18-21. [Google Scholar]
[8]. N Micro, HS Sharma, Controlled multicenter study on chronic suppurative otits media treated with topical applications of ciprofloxacin 0.2% solution in single dose containers or combination of polymyxin B, neomycin and hydrocortisone suspension.Otolaryngol Head Neck Surg. 2000 123:617-23. [Google Scholar]
[9]. Dohar C M Alper, A Elizabeth, W J Doyle, Treatment of Chronic Suppurative Otits Media with topical Ciprofloxacin.Ann Otol Rhino Laryngol. 1998 107:865-71. [Google Scholar]
[10]. L Kasemsuwan, P Clongsuesuek, A double blind prospective trial of topical ciprofloxacin versus normal saline solution in the treatment of otorrhea.Clin Otolaryngol Allied Sci. 1997 22(1):44-6. [Google Scholar]
[11]. CA Macfadyen, JM Acuin, Gamble Systemic antibiotic versus topical treatments for chronically discharging ears with underlying eardrum perforations.Cochrane Database Syt Rev. 2006 1-CD005608. [Google Scholar]
[12]. C Jay, A Job, E Mathai, B Antonisamy, Evaluation of topical povidoneiodine in chronic suppurative otitis media.Arch Otolaryngol Head Neck Surg. 2003 129(10):1098 [Google Scholar]
[13]. S Eposito, S Noviello, G D’Errico, C Montanaro, Topical and oral treatment of chronic otitis media with ciprofloxacin.Arch Otolaryngol Head Neck Surg. 1990 116(5):557 [Google Scholar]
[14]. C Nawabusi, FE Ologe, PKS Lu, Pathogenic agents of chronic suppurative otitis media in Ilorin Nigeria.East African Medical Journal. 2002 79(4):202-05. [Google Scholar]