Unilateral Right Pulmonary Agenesis in Adulthood
Hediye Pinar Gunbey1, Emre Gunbey2, Asli Tanrivermis Sayit3, Taner Bulut4
1Faculty, Department of Radiology, Ondokuz Mayıs University, Samsun, Turkey.
2Faculty, Department of Otorhinolaryngology, Ondokuz Mayıs University, Samsun, Turkey.
3Faculty, Department of Radiology, Gazi Hospital, Samsun, Turkey.
4Faculty, Department of Radiology, Adıyaman University Hospital, Adıyaman, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hediye Pınar Gunbey, 19 Mayıs University, Department of Radiology, Kurupelit-55159 Atakum/Samsun, Turkey.
Phone: +90 (0362) 312 19 19, + 90 505 457 90 52, Fax: +90 (362) 457 60 91,
E-mail: hpgunbey@hotmail.com
Congenital malformations of the lung, which may vary in degrees of severity, are very rare diseases. Pulmonary artery agenesis is a rare anomaly that may occur during the early involution of the proximal portions of the sixth aortic arch, during embryological development of the heart. This agenesis may be accompained by a complete or partial absence of the lung and its bronchus on the same side, which is diagnosed as pulmonary agenesis. In the great majority of the cases, the diagnosis is usually made at or soon after birth and it can be associated with multiple anomalies. However, extremely rare asymptomatic cases may go unnoticed until adulthood. We are presenting a patient with unilateral right pulmonary agenesis, who survived through adulthood without any symptoms and other congenital anomalies. The multislice computed tomography findings and differential diagnoses have been discussed.
Pulmonary agenesis, Thorax imaging, MSCT
Case Report
A 26-year-old woman was referred to the department of diagnostic Radiology for assessing an incidentally found, unusual view in the chest radiogram, before she underwent cystectomy of the right ovary. She had a haemorrhagic cyst in the right ovary, that had not regressed for three months. The patient had no previous pulmonary complaint or physical restriction before and she had a healthy baby boy by a normal delivery. In the history of the patient, there was no mention of connective tissue disorders, other systemic anomalies, diabetes, trauma or surgery. Her physical examination revealed no breathing sound on the right and a normal breathing sound on the left hemithorax, while the heart’s sound was heard from the right hemithorax.
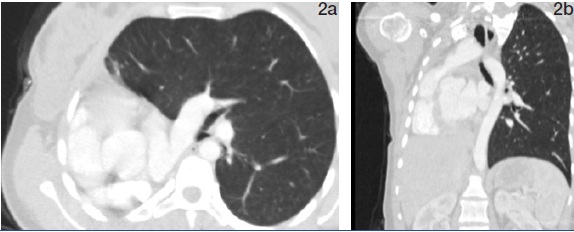
The posteroanterior chest X-ray which was taken prior to surgery demonstrated complete opacification of the right hemithorax, with a mediastinal and tracheal shift to the right side [Table/Fig-1]. The volume of contralateral lung was increased, with anterior herniation of the hyperinflated upper lobe. Computed tomograhy (CT) imaging was performed by using a 64-slice MDCT scanner (Brillance 64; Philips Medical Systems, Best, Netherlands) and following acquisition parameters were seen: 120 kVP, 200 mA with a tube rotation of 420 ms, 0.625 mm slice collimation, 14 mm/s table feed and 1.4 pitch factor. A lung window setting CT examination demonstrated total absence of the right pulmonary parenchyma, right pulmonary artery and right main bronchus [Table/Fig-2a,b]. On the basis of these findings, the patient was diagnosed to have right-sided pulmonary agenesis. The mediastinal window setting CT clearly showed deviation of mediastinal structures, heart and trachea totally to the right side [Table/Fig-3]. The left lung parenchyma was hyperaerated, with herniating upper lobe connected to the right hemithorax [Table/Fig-4]. Right hemidiaphragm was elevated. Agenetic azygos vein and dilated hemiazygos vein were the accompanying vasculary anomalies. Left main pulmonary artery and thoracic aorta showed normal configuration and measurements. The heart size was normal. The patient had no vertebral or rib abnormalities. Abdominal sonography did not reveal any abnormalities in this patient. She underwent cystectomy surgery of the right ovary under general ansesthesia, without any complications. The patient was discharged from the hospital 5 days after surgery, in good condition.
Posteroanterior radiograph shows a small, dense right hemithorax with mediastinal shift and herniation of the contralateral lung

2a and 2b, A lung window setting computed tomography scan reveals a complete absence of the right lung and the right main bronchus with anterior herniation of the left lung. The heart and mediastinum are shifted toward the right side
Mediastinal window setting computed tomography scan reveals the absent right pulmonary artery (arrow)

The posterior view of the 3-dimensional airway rendering image of the lung shows the anterior herniation of the left lung, and the absent right main bronchus (arrow)

Discussion
Pulmonary agenesis is a rare developmental defect which is characterized by a complete absence of the lung and its bronchus [1]. Its incidence varies between 1/10,000 to 12,000 births [2]. The aetiology, as per experimental evidence, shows implicated vitamin A deficiency, folic acid deficiency and salicylates as the causes of the pulmonary agenesis [3]. The appearance of pulmonary agenesis in twin studies which were done, suggested a genetic origin, which simulated foetal vascular conditions. In one case, there was an anomaly in the short arm (p arm) of choromosome 2 [4,5].
Pulmonary agenesis can be localized to a single lobe and it can affect an entire lung or in rare cases, both lungs [6]. It is frequently diagnosed soon after birth or during childhood, due to early onset of its symptoms [3,7-9]. Although a majority of patients with unilateral agenesis die soon after birth or in early childhood, in some extreme cases, patients can survive upto adulthood without any symptoms, like our patient, who has been mentioned above. Only few cases have been reported in the literature [10,11]. There is no right versus left or male versus female predominance [6], but right pulmonary genesis has a poor prognosis and a high risk of coexistance with other congenital anomalies. Associative congenital abnormalities have been found in more than 50% of the patients, which mainly involve the cardiovascular, gastro-intestinal, musculoskeletal and urogenital systems [4,12], chest wall, diaphragm, ipsilateral face and abdominal wall, Vertebral anomalies are also seen [6].
In our case, no other congenital anomaly was detected in the presence of unilateral right pulmonary agenesis, except agenetic azygos vein and dilated hemiazygos vein. In physical examination, this condition can be detected incidentally, as it was in our case, but patients frequently come with respiratory distress when the degree of underdevelopment of the lung is severe.
The most common presentations on Pulmonary Agenesis (PA) chest films are opacification and decreased size of affected hemithorax, compensatory hyperinflation of the contralateral hemithorax, elevation of ipsilateral hemidiaphragm, absent ipsilateral and enlarged contralateral pulmonary artery shadow and ipsilateral shift of mediastinum [1].
Our patient demonstrated all of these findings. In order to make a definitive diagnosis, bronchographic or angiographic techniques can be used. But today’s technological developments in radiology have reduced the need of invasive procedures, like pulmonary angiography. A definitive diagnosis can easily be made by MDCT and MR angiography.
Radiographically, agenesis of a lung may appear as pneumonectomy or a total collapse of the lung. The differential diagnosis may also include diaphragmatic hernia and eventration, pneumonitis, pleural effusion, hypoplasia, obstructive lung diseases and mainly, lung cancer.
We are presenting this case in view of its asymptomatic status until adulthood, which was an exceptionally rare condition. MDCT can demonstrate parenchymal, bronchial, vascular and all structural features of pulmonary agenesis. Although examples of most of the anomalies in children have been reported, physicians who treat adults should also be aware of abnormal chest radiography.
[1]. AC Argent, BJ Cremin, Computed tomography in agenesis of lung in infantsBr J Radiol 1992 65:221-4. [Google Scholar]
[2]. RG Fraser, JAP Pare, Developmental anomalies affecting the airways and lung parenchyma. In: Fraser RG, Pare JAP, Eds. Fraser and Pare’s Diagnosis of Diseases of the Chest. 1999 PhiladelphiaW.B. Saunders Company:597-635. [Google Scholar]
[3]. AS Roque, EM Burton, Unilateral pulmonary agenesis without mediastinal displacement.South Med J. 1997 90:335-7. [Google Scholar]
[4]. C Campanella, JA Odell, Unilateral pulmonary agenesis: A report of four casesS Afr Med J 1987 71:785-7. [Google Scholar]
[5]. B Say, NJ Carpenter, G Giacoia, Agenesis of the lung associated with a chromosome abnormality (46,XX,2P+).J Med Genet 1980 17:477-8. [Google Scholar]
[6]. RM Kravitz, Congenital malformations of the lungPedatr Clin North Am 1994 41:453-72. [Google Scholar]
[7]. H Nazaroğ lu, A Mete, Y Bukte, Agenesis of the right lung presenting as a pulmonary infectionClin Radiol. 2002 57:529-30. [Google Scholar]
[8]. G Shivanand, S Mukhophadyay, S Vashisht, An unusual cause of recurrent respiratory tract infection: unilateral pulmonary agenesisEur J Radiol E. 2003 48:67-9. [Google Scholar]
[9]. RJ Thomas, HC Lathif, S Sen, Varied presentations of unilateral lung hypoplasia and agenesis: a report of four cases.Pediatr Surg Int 1998 14:94-5. [Google Scholar]
[10]. A Mas, RM Mirapeix, C Domingo, Pulmonary hypoplasia presented in adulthood as a chronic respiratory failure: report of two cases. Embryology, clinical symptoms and diagnostic procedures.Respiration. 1997 64:240-3. [Google Scholar]
[11]. SS Hacıevliyagil, H Günen, O Yetkin, Asymptomatic Pulmonary Agenesis: Our Experience with Two CasesTurkish Respiratory Journal. 2006 7(1):31-3. [Google Scholar]
[12]. IS Kaya, U Dilmen, Agenesis of the lungEur Respir J.. 1989 2:690-2. [Google Scholar]