Introduction: Neglected Monteggia fracture dislocation in the paediatric age group constitutes significant disability in respect to pain, stiffness, deformity, neurological compromise and restriction of activities of daily living.
Materials and Methods: A longitudinal prospective study was done on 21 children with old Monteggia fracture-dislocation which included 18 cases of Bado type I and 3 cases of Bado type III at the department of orthopaedics, IPGME&R,SSKM hospital, Kolkata, India between 2007 and 2012. All were treated by modified Hirayama corrective osteotomy of ulna with wedge bone grafting along with restoration of its length and reconstruction of annular ligament using Bell Tawse method and fixation of radial head with transcapitellar Kirschner wire. Average follow up period was 5.5 years.
Results and Analysis: Results were evaluated on the basis of 100 point Mayo Elbow Performance Index, radiology and questionnaire. The mean postoperative increase in Mayo Elbow Performance Index score was 30 with average increase in the range of movement by 30o. In three cases, there was subluxation of radial head and in addition one had transient palsy of posterior interosseous nerve. Three cases showed distortion of the radial head which were insignificant functionally. Results of improvement in mean MEPI were analysed by chi-square test and was significant at 0 .01 level of significance.
Conclusion: Study showed good results with modified Hirayama osteotomy with annular ligament reconstruction using Bell Tawse procedure which is a more biological option for restoration of elbow biomechanics.
Introduction
Neglected Monteggia fracture-dislocation is an uncommon injury in children, which often results in significant disability from malunion due to persistent angulated and displaced fracture of ulnar shaft along with dislocation of radial head. Pain, stiffness, deformity, neurological compromise and even instability of distal radioulnar joint ensues [1,2] .
Missed Monteggia fracture dislocation classically implies duration of more than 4 weeks [3,4] . The patients also have significant disability in less severe injury with minimum angulations of ulnar fracture, where radial head dislocation may be missed. Therefore, this emphasises the importance of such injury to a competent orthopedic surgeon in reviewing all elbow injuries at an early stage. Often patients attend hospital, weeks or months after the injury. These two factors of significant deformity and delayed presentation constitute the problem of management of old Monteggia fracture-dislocation in paediatric age group. Restoration of radiocapitellar joint and biomechanics of the elbow joint is of paramount importance for favourable long term functional outcome.
Previously many authors have described various operative procedures regarding its management such as reconstruction of annular ligament [5,6] , osteotomy of ulna [7,8] or a combination of annular ligament reconstruction and osteotomy [9] or a combination of open reduction of radial head with a repair of annular ligament and osteotomy of ulna [10] .
Such studies have been an ongoing process in our department. This study is a part of a series of related studies some of which has been previously published in similar esteemed journals and further studies in the series will be reported by us in the future.
Here, we are reporting the result of modified Hirayama corrective osteotomy [7] of ulna with internal fixation and bone grafting combined with reduction of radial head and its fixation by Kirschner wire along with annular ligament reconstruction with a strip of triceps fascia in single stage [6,11] .
Aims and Objectives
The aim was to evaluate the outcome of neglected Monteggia fracture dislocation with modified Hirayama osteotomy of ulna along with annular ligament reconstruction with a strip of triceps fascia using the Bell Tawse method in single stage.
The objective was to analyse the results in respect to mean increase in Mayo Elbow Performance Index (MEPI).
Null hypothesis: Neglected Monteggia fracture dislocation Bado I and III types does not show significant improvement in MEPI after modified Hirayama osteotomy combined with annular ligament reconstruction with a strip of triceps fascia using the Bell Tawse method.
Material and Methods
We have treated 21 patients of post traumatic symptomatic old Monteggia fracture –dislocation from the year 2007 to 2012 in the department of orthopaedics at IPGME&R, SSKM Hospital, India. The age of patients at the time of reconstruction ranged from 7-14 years (average 10.7 years). There were 13 girls and 8 boys ; right side were affected in 10 patients and left side in 11. Among them, 18 patients were of Bado [12] type I and 3 were of Bado [12] type III. No patients with either type II or type IV were reported.
The inclusion criteria included time interval between injury and surgical repair at least more than four weeks and this varied in our study between 8-26 weeks (average 17.5 weeks).The exclusion criteria included gross distortion of the radial head. No posterior interosseous nerve palsy was detected preoperatively in any of the cases. Only one patient had associated ipsilateral anterior dislocation of hip.
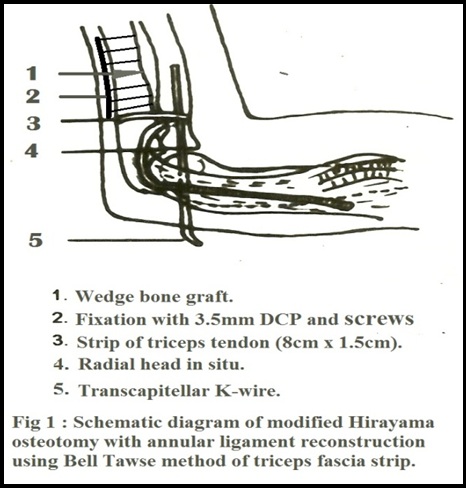
Under general anaesthesia and tourniquet, applied on the upper arm, a postero-lateral skin incision was made extending from 10cm above the elbow to expose triceps muscle, radio-capitellar joint and the malunited site of the ulna through Speed and Boyd approach. Subperiosteal ulnar osteotomy was done about 5cm below the olecranon and distraction of the osteotomy was made by about 1cm to lengthen the ulna with angulation to produce overcorrection of the deformity. Correction of anterior displacement of the radial head by posterior angulation of the ulna and lateral dislocation by medial angulation was made. Oblique osteotomy of malunited ulna was fixed with a 3.5mm narrow dynamic compression plate or a recon plate bent to an angle of 150 with at least three proximal and distal screws after correction of malunion and height of ulna and ensuring proper repositioning of radial head without excessive notching. An autoiliac ipsilateral wedge graft was inserted in the osteotomy site. The radial head was defined. Fibrous remnant of annular ligament and other fibrous tissues were removed. A new annular ligament was reconstructed by turning down a strip of triceps fascia with tendon leaving its base attached to the ulna and passing it round the neck of the radius from behind forward and anchoring it through a drill hole in the ulna. Radial head was fixed in position with a transcapitellar Kirschner pin [Table/Fig-1] . Wound was closed in layers. The limb was immobilized in plaster cast with 900 elbow flexion and full supination. After two weeks, transcapitellar Kirschner pin was removed.
The limb was kept immobilized in a plaster cast for six weeks. After removal of plaster, the patient was encouraged to do active exercises (flexion, extension, pronation and supination).
Schematic diagram of modified Hirayama osteotomy with annular ligament reconstruction using bell tawse method of triceps fascia strip
Chi-Squre test on the effectiveness of the outcome of the surgery
| Results of Postoperative Clinical Assessment |
| Montegggia Type FRA CTURE ↓ | Improvement in mean ME PI → | Total |
| BADO- I | 30 | 40 | 35 | 30 | 25 | 20 | 25 | 20 | 30 | 35 | 30 | 30 | 30 | 30 | 30 | 30 | 35 | 35 | 540 |
| BADO- III | 40 | 30 | 20 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 90 |
| TOTAL | 70 | 70 | 55 | 30 | 25 | 20 | 25 | 20 | 30 | 35 | 30 | 30 | 30 | 30 | 30 | 30 | 35 | 35 | 630 |
| No of subjects | Subluxation of radial head | Distortion of radial head | Post-interosseus nv. palsy | Av increase in ROM in degrees | Av increase in MEPI | Av duration of union in weeks | Superficial infection |
| 21 | 3 (14.3%) | 3 (14.3%) | 1 (4.8%) | 30 | 30 | 10 | 3 (14.3%) |
(4a,b) Preop AP and lateral view skiagrams showing Bado type III Monteggia fracture dislocation
(4c,d) Postop AP and lateral view skiagrams showing Hirayamacorrective osteotomy fixed with DCP, wedge bonegraft and radiocapitellar K wire in the same case.

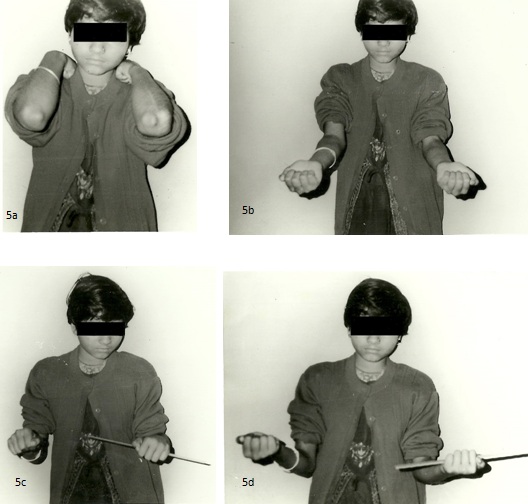
Clinical photograph of a patient evaluated in our study showing good range of post-operative flexion, extension, pronation & supination movements
Results and Analysis
Follow up period varied from 2 to 7 (average 3.54) years [Table/Fig-2]. All patients of ulnar osteotomy united in good position and the length of ulna was maintained. All 18 (85.7%) patients of Bado type I fracture achieved good range of motion with no evidence of residual radial head subluxation. Three (14.3%) Bado type III fractures showed mild subluxation of radial head – which however did not interfere with the normal functional activity. Transient posterior interosseous nerve palsy detected in one case (4.8%) recovered at 6.5 months after operation. Three patients (14.3%) had distortion of the radial head which however did not interfere significantly with the final functional outcome. Three patients (14.3%) also had superficial wound infection which subsided by change of antibiotic based on swab culture and sensitivity report [Table/Fig-3] .
The mean operating time was 80 (range 70–90) minutes. The patients were followed up every six weeks for the initial six months then every 12 wks for the next 6 months and finally annually thereafter. The mean duration of radiological bony union was 10 weeks (range 8-12 wks).
Postoperative assessment comprised of clinical evaluation, skiagrams and questionnaire.
Physical Examination comprised of reduction in tenderness,Range of Movement (ROM) of elbow, forearm and wrist, grip and two point pinch strength (with Dynamometer), motor and sensory exam, stability to varus-valgus stress test with elbow in maximum extension and 300 flexion, stability of distal Radioulnar Joint (RUJ) in maximum pronation and carrying angle.
Questionnaire especially comprised of ability to perform daily activities with level of satisfaction as well as hand dominance, occupation, anatomic location of pain in the elbow and wrist joint, stiffness, weakness or limitation of motions.
Skiagrams in true AP in as much as full extension and lateral view in 900 elbow fexion with forearm pronated and shoulder abducted 900 were taken and carrying angle, capitellum-radial head distance, percentage of subluxation, diameter of radial head, ulnar bow and ulnar variance were noted [Table/Fig-4] . Assessment of radiological analysis was done using the method devised by Kim et al., [13 ,14] .
The Mayo Elbow Performance Index was used to assess subjective, objective, and functional characteristics before and after the operation and at the final follow-up. This scoring system has 4 parameters: 45 points are given for a pain-free elbow, 20 points for normal elbow movement, 10 for a stable elbow and 25 for performance of five activities of daily living. Stability of the elbow is rated as stable (no apparent varus/valgus instability), moderate (<10º varus/valgus instability), or gross (≥10º varus/valgus instability).
Based on the Mayo Elbow Performance Index, at the final follow-up the mean increase in MEPI was 30. The mean range of motion increased by 300. All patients had a supination-pronation arc of ≥100º; the range of supination was always less than that of pronation. The mean supination-pronation arc was 140º. Although no significant correlation was noted between the range of movements achieved and the duration of treatment, patients treated earlier had a greater range of movements than those treated later. At the final follow-up, no patient had any sign of instability [Table/Fig-5] .
The X2 critical value for 17 df is 33.409 at 0.01 level of significance and the obtained value is 247.27, greater than the table value. This indicates that there is a positive relationship in between the type of fracture and the improvement in the mean results after surgery.
Monteggia fracture dislocation, Bado-I and Bado-III types show a significant mean improvement which is accepted at 0.01 level of signicance after surgical management with modified Hirayama osteotomy and annular ligament reconstruction by Bell Tawse method. Thus, the null hypothesis is rejected and the alternative hypothesis is accepted.
Discussion
Neglected fracture-dislocation of Monteggia is due to delayed presentation and/or delayed or inadequate treatment which constitute a definite problem. Closed reduction does not correct the deformity nor maintain the anatomical reduction.
Missed Monteggia fracture causes chronic radial head dislocation even with malunion of proximal ulna. The resultant shortening of the forearm with associated deformity produces significant restriction of elbow and forearm motions, pain, instability and compromise of the activities of daily living (ADL).
Modified Hirayama osteotomy with annular ligament reconstruction is a biological option addressing to the restoration of the elbow biomechanics. The stabilizing action of the interosseous membrane further helps to maintain the reduced position of the radial head [15] . Soft tissue stabilization by annular ligament reconstruction is essential for prevention of residual radial head dislocation or subluxation which is originally not a part of the conventional Hirayama osteotomy [16] . A wedge ipsilateral autoiliac bone graft was inserted to promote bony union which also was not included in the classical Hirayama osteotomy. Controversy exists regarding reconstruction of the annular ligament. Nakamura et al., [2] and David-West et al., [17] advocate it in all cases while others like Devnani [3] and Bhojraj et al., [18] disregard it completely. Others like Bhaskar et al., [4] prefer an intra operative decision based on the stability of reduction. Garg et al., [19] reported better results with annular ligament reconstruction using Palmaris longus graft but we believe that Bell Tawse procedure is a better option than the free Palmaris longus and is more biological and viable with improved long term functional outcome.
Open reduction of radial head and reconstruction of annular ligament combined with ulnar osteotomy by Rodgers et al., [1] showed unpredictable results in his five of seven cases; whereas Inoue and Shionoya [20] reported their good result only in anterior Monteggia lesion. We have no experience regarding closed reduction by gradual lengthening of angulated ulna using an external fixator in the treatment of old dislocation Monteggia as reported by Exner [21] In our series, we have achieved good function of elbow and forearm with mean increase in MEPI by 30 points.
We believe that even though spontaneous reduction of the radial head takes place after correction of the ulnar deformity, annular ligament reconstruction should be done in all cases for restoration of elbow biomechanics. No evidence of significant extension lag or notching and restriction of motion were seen in our study using the triceps sling.
Conclusion
Neglected Monteggia fracture dislocation in children can produce significant orthopaedic complications with gross restriction of activities of daily living. Early diagnosis and prompt management results in favourable long term outcome. Restoration of ulnar length and reduction of the radial head with the combined approach of modified Hirayama osteotomy along with annular ligament reconstruction using Bell Tawse sling method is a more biological option for the restoration of the elbow biomechanics and increase in the Mayo Elbow Performance Index.
[1]. WB Rodgers, PM Waters, JE Hall, Chronic Monteggia lesions in children. Complications and results of reconstructionJ Bone Joint Surg Am 1996 78:1322-9. [Google Scholar]
[2]. K Nakamura, K Hirachi, S Uchiyama, M Takahara, A Minami, T Imaeda, Long term clinical and radiographic outcomes after open reduction for missed monteggia fracture-dislocations in children.J Bone Joint Surg Am 2009 91:1394-404. [Google Scholar]
[3]. AS Devnani, Missed Monteggia fracture dislocation in childrenInjury. 1997 28:131-3. [Google Scholar]
[4]. A Bhaskar, Missed Monteggia fracture in children: Is annular ligament reconstruction always required?Indian J Orthop 2009 43:389-95. [Google Scholar]
[5]. AJ Bell Tawse, The treatment of malunited anterior Monteggia fractures in children.J Bone Joint Surg Br 1965 47:718-23. [Google Scholar]
[6]. WC Campbell, Malunited fractures and unreduced dislocation about elbowJAMA. 1929 92:122-8. [Google Scholar]
[7]. T Hirayama, Y Takemitsu, K Yagihara, A Mikita, Operation for chronic dislocation of the radial head in children. Reduction by osteotomy of the ulna.J Bone Joint Surg Br. 1987 69:639-42. [Google Scholar]
[8]. R Judet, G Lord, R Roy-Camille, Osteotomy of the cubital diaphysis in old dislocations of the radial head in the childPresse Med 1962 70:1307-08. [Google Scholar]
[9]. GC Lloyd-Roberts, TM Bucknill, Anterior dislocation of the radial whead in children: Aetiology, natural history and management.J Bone Joint Surg Br 1977 59:402-7. [Google Scholar]
[10]. A Kalamchi, Monteggia fracture-dislocation in children. Late treatment in two cases.J Bone Joint Surg Am 1986 68:615-9. [Google Scholar]
[11]. A Cappellino, SW Wolfe, JS Marsh, Use of a modified Bell Tawse procedure for chronic acquired dislocation of the radial head.J Pediatr Orthop 1998 18:410-4. [Google Scholar]
[12]. JL Bado, The Monteggia Lesion.Clin Orthop 1967 50:71-86. [Google Scholar]
[13]. HT Kim, JN Conjares, JT Suh, CI Yoo, Chronic head dislocation in children, Part 1: Pathologic changes preventing stable reduction and surgical correction.Pediatr Orthop. 2002 22:583-90. [Google Scholar]
[14]. HT Kim, BG Park, JT Suh, CI Yoo, Chronic radial head dislocation in children, Part 2: Results of open treatment and factors affecting final outcome.J Pediatr Orthop 2002 22:591-7. [Google Scholar]
[15]. T Nakamura, Y Yabe, Y Horiuchi, Functional anatomy of the interosseous membrane of the forearm—dynamic changes during rotationHand Surg 1999 4:67-73. [Google Scholar]
[16]. JV Fowles, N Sliman, MT Kassab, The Monteggia lesion in children. Fracture of the ulna and dislocation of the radial headJ Bone Joint Surg Am 1983 65:1276-82. [Google Scholar]
[17]. KS David-West, NI Wilson, DA Sherlock, GC Bennet, Missed Monteggia injuriesInjury. 2005 36:1206-9. [Google Scholar]
[18]. SD Bhojraj, Surgical correction of malunited Monteggia fractures in childrenIndian J Orthop 1981 21(2):138-44. [Google Scholar]
[19]. P Garg, P Baid, S Sinha, R Ranjan, U Bandyopadhyay, SR Mitra, Outcome of radial head preserving operations in missed Monteggia fracture in childrenIndian J of Orthop 2011 45(5):404-9. [Google Scholar]
[20]. G Inoue, K Shionoya, Corrective ulnar osteotomy for malunited anterior Monteggia lesions in children. 12 patients followed for 1-12 years.Acta Orthop Scand 1998 69:73-6. [Google Scholar]
[21]. GU Exner, Missed chronic anterior Monteggia lesion: closed reduction by gradual lengthening and angulation of the ulna,J Bone Joint Surg [Br.]. 2001 83(B):547-50. [Google Scholar]