Background: Dental health among the patients undergoing haemodialysis therapy has been found to be debilitated and gets worsened with the increased duration of hemodialysis.Hence the present study aimed to assess the effect of duration of hemodialysis and the underlying kidney disease on the dental health status of patients.
Settings and Design: A cross-sectional study was conducted on 400 patients and 400 controls selected through stratified random sampling method from five zones of Delhi, India.
Materials and Methods: The patient group was divided into following five groups in order to evaluate influence of duration of hemodialysis therapy on dental status of the subjects-a)≤ three months b)four to six months c)seven to nine months d) ten to twelve months and e) more than twelve months. Dental health was assessed using WHO dentition status and treatment needs, community periodontal index, oral hygiene index, prosthetic status and needs.
Statistical Analysis Used: Student t-test, Chi-square test, one-way analysis of variance (ANOVA) and Pearson’s correlation was used to determine the difference in clinical parameters among the subgroup and between the patients and controls.
Results: Positive correlation was found between the frequency of dialysis and maximum CPI scores (p-value=0.018). 81.25% of patients and 74.75% of the controls had CPI score 2. Loss of attachment scores in patients was higher than the healthy controls (p-value 0.035). Mean OHI scores for the patients was 5.15±1.975 and for controls was 5.01±2.213 (p=0.635). Mean DMFT score of patients and controls was 3.552 and 3.559 respectively (p=0.937). 23%of controls showed presence of dental prosthesis in comparison to only 14.5 % of patients (p=0.05). Type of underlying kidney disease and duration of hemodialysis had significant influence on O.H.I scores and Prosthetic needs.
Conclusion: Dental health status was found to be debilitated among the hemodialysis patients and got worsened with the duration of hemodialysis and the type of underlying kidney disease mainly due to oral health negligence contributing to morbidity and potential mortality. Further emphasis on the effective implementation of oral health promotion programme for medically compromised patients is thus advocated.
Introduction
Health is the most important human asset which determines the living efficiency of an individual. Since beginning, mankind has sought for good health. Good health is a major resource for social, economic and personal development and an important dimension of quality of life [1]. Diseases of various kinds influence the health of individuals and are broadly classified into two types-communicable and noncommunicable diseases. A shift in the prevalence of disease is now evident such that the communicable diseases which were the major reason for fatality are now on the downfall with the contrary rise of noncommunicable diseases [2].
Changes in diet, sedentary lifestyle and rapid population aging in developing countries like India have caused an increase in the major noncommunicable diseases (NCDs)—such as cardiac problems, cancers, diabetes, psychiatric disorders, and chronic respiratory diseases [2]. These are now quickly adding to the worldwide burden of disease and have become the leading cause of death globally killing more people each year than all other causes combined [3]. In the global burden of disease study for 1990, which estimated the distribution of deaths by region, noncommunicable diseases ranked first as the cause of death in developed countries, as well as in many developing countries and the world as a whole. Thus, addressing the problems and issues connected with noncommunicable diseases will lead to major health gains worldwide [3,4].
Kidneys are one of the most important excretory organs and renal diseases pose a major health problem of modern world [5,6]. The most frequent aetiology of chronic renal failure includes diabetes mellitus, hypertension, glomerulonephritis, polycystic kidney disease and pyelonephritis [7,8].
In the last 3 to 4 decades; improvements in dialysis and transplantation have reduced morbidity and mortality among patients with end-stage renal disease. Hemodialysis therapy is usually a long duration therapy with usual frequency of once, twice or more than twice a week increasing the stress level amongst the patients [9].
Despite the fact that the hemodialysis therapy have increased the survival rate among the patients affected by renal disease, there has been growing concerns regarding the other systemic diseases in these patients, due to lack of their ability to control water and electrolyte balance and filtrate waste products [10].
Also, dental health among the patients undergoing haemodialysis therapy have been found to be poor due to their debilitated state, neglect of oral hygiene, manifestations of systemic conditions and immunosupression as shown in the studies done by Parkar S.M. [11] and Malekmakan L et al., [12]. The specific effects of chronic renal disease and renal replacement therapy on periodontal tissues include gingival hyperplasia, increased level of plaque, calculus and destructive periodontal disease. The findings have been reported by Torkzaban P [10], Joseph R [13] and Ertugrul F et al., [14]. Other effects on oral health include bad odour/metallic taste due to increased concentration of fluid intake and salivary gland alteration, paleness of the mucosal membranes due to anaemia, uremic stomatitis, gingival bleeding due to platelet dysfunction and the affects of anticoagulants, enamel hypoplasia, erosions on the surface of the teeth because of acidic regurgitation and vomiting induced by uremia, pulp obliteration due to calcium and phosphorus metabolism, changes in maxillary bone and increased risk of fractures [5,15]. Furthermore, the severity of dental diseases have been found to be directly correlated with the duration of hemodialysis [8].
There is limited literature available to evaluate the effect of duration of hemodialysis therapy and the underlying kidney disease on dental health status of the patients undergoing hemodialysis. Hence, the present study aimed to assess the effect of duration of hemodialysis and the underlying kidney disease on the Dental health status of patients undergoing hemodialysis at various dialysis centres of multispeciality hospitals in Delhi and to make appropriate recommendations and suggestions for improving their oral health.
Materials and Methods
Study Design
The present cross-sectional study was conducted at dialysis centres of five multispecialty hospital in Delhi over a period of four months ( March-June 2013).
Sampling
For the study purpose, Delhi is arbitrarily divided into five zones namely north, south, east, west & central. Using stratified random sampling method a total of 400 hemodialysis patients with mean age 51.33 ±16.1 years and 400 controls with mean age 50.05 ±14.4 years; (80 patients and 80 controls from each hospital) were selected, based on the inclusion and exclusion criteria. The patients were matched with the healthy controls for age and sex. The controls were mainly the relatives of the hemodialysis patients attending the dialysis unit.
Inclusion Criteria
Patients who needed outpatient hemodialysis therapy.
Subjects who gave consent for clinical examination.
Exclusion Criteria
The patients with the presence of an additional infectious disease (Hepatitis A, B, C, HIV infection).
Those suffering from drug dependency.
Patients who had seizures or nervous disorders.
The patient group was divided into following five groups in order to evaluate the influence of duration of hemodialysis therapy on dental status of the subjects:
a)≤ three months b)four to six months c)seven to nine months d) ten to twelve months and e) more than twelve months and further based on the frequency of dialysis as once, twice & more than twice a week.
Ethical Clearance and Informed Consent
The study design was reviewed and approved by the institutional ethical committee.
Written informed consent was obtained from the study subjects after explaining the purpose and methodology of the study.
Data Collection
A structured Performa in English was used to record information on sociodemographic profile, past dental history, adverse oral habits (like smoking, tobacco use, alcohol intake) and oral hygiene practices of all the study subjects. For the patients undergoing hemodialysis, additional information was collected regarding duration & frequency of hemodialysis, and underlying kidney disease to assess if they had any correlation with the clinical parameters. The Performa was filled through the personal interviews by the investigator.
Training and Calibration of Examiners
A single trained examiner carried out all the examinations in the survey. The examiner was trained and calibrated in the Department of Public Health Dentistry prior to the survey by carrying out the examinations on the preselected subjects and then repeating the examination on the successive day. The diagnostic variability in two assessments was found to be small and agreement was found to be appreciably high (Kappa value 0.85).
Clinical Assessment
Dental caries was assessed using WHO dentition status and treatment need, community periodontal index and loss of attachment were used to assess the periodontal status. Prosthetic status and prosthetic needs were also recorded [16]. Oral hygiene index (1960) was used to evaluate debris and calculus deposits on the teeth [17]. Referral was done for the patients with significant findings.
Statistical Analysis
All the collected data was entered in the Microsoft word excel sheet 2007 version and processed using the SPSS 16 version. The mean, standard deviations and the proportions (% of subjects affected) were calculated for each clinical parameter.
Student t-test was used to analyze the difference between the means of the two groups. The Chi-square test was used to anaylse difference between the proportions of the two groups. One-way-ANOVA and Pearson’s correlation was used to determine the difference in clinical parameters among the subgroups.
Results
A total of 400 hemodialysis patients, 268 (67%) males and 132 (33%) females and 400 healthy controls were included in the study.
The highest CPI and LOA score was used to assess the periodontal status in both dialysis group and control group. According to CPI scoring, 81.25% of the patients had calculus and plaque retentive factors as compared to 74.75% in the control group (CPI code 2). On the other hand 10% of the healthy controls had shallow pockets as compared to 7.5% in the patients (CPI code 3).None of the subjects in the patient group was found to have healthy periodontium (CPI code 0) while 2.25% of controls had healthy periodontium. The difference based on CPI scores was found to be statistically significant (p-value= 0.026).
In the patients undergoing hemodialysis, the loss of attachment scores were significantly higher as compared to the healthy controls (p-value =0.035). 35.6 % of the patients reported with LOA scores of 1 as compared to 20.9 % in the controls. The attachment loss of 4-5 mm (score 2) was present in 5.1% of the patients whereas 3.3% of the patients had LOA score 2. None of the healthy controls and patients had attachment loss of 9-11 mm (LOA score 30).
The caries prevalence was significantly higher (p=0.005) among the hemodialysis patients (88%) as compared to the healthy controls (72.5%). However there was no statistically significant difference between the mean caries experience of the patient and controls (mean DMFT score of patients 3.552 and of controls was 3.559, p=0.937).
The oral hygiene index revealed that the mean OHI scores for the hemodialysis patients (5.15±1.975) was marginally higher as compared to the healthy controls (5.01±2.213) but this difference was not statistically significant (p=0.635).
Discussion
Hemodialysis has become a life saving intervention for the patients with compromised renal function that has significantly reduced the mortality caused by these diseases. It is well documented that systemic conditions such as renal disease and its treatment modalities may affect the oral cavity resulting in an increased global burden of oral diseases amongst these patients [2,10,11].
The mean age of the patients was 51.33±16.1 years & controls was 50.05 ±14.4 years respectively. This is in agreement with the studies done by Dumitrescu et al., [18], Malekmakan et al., [12] and Murthy AK et al., [18] but was higher than the studies done by Jenabian et al., [8], Joseph et al., [13] and Parkar SM et al., [11]. This could be due to higher prevalence of renal diseases in older age groups and wider age group included in our study (patients from 20 to 88 years of age groups).
The difference in the periodontal status based on CPI and LOA scores was significantly poor in the patients as compared to the controls Similar results were reported by Parkar SM et al., [11], Joseph R et al., [13], Murthy AK et al., [19], Cervero J.A. et al., [20], Bayraktar G et al., [21], Dencheva M et al., [22] and Bhatsange A et al., [23]. The debilitated periodontal condition among the patients may be attributed to neglect of proper oral hygiene practices by the patient as they are preoccupied by more time consuming and life threatening kidney disease. Low self esteem, dissatisfaction and stress contribute to anxiety reactions and depression in hemodialysis patients, further deteriorating their periodontal health. Early intervention in dental health with proper recall scheduling can improve their dental health remarkably [11,13,22].
The study shows that the dental health deteriorated with the increasing duration of hemodialysis. Though the difference was not significant, the various clinical parameters measured get worsened [Table/Fig-1]. Similar results were reported by Parkar SM et al., [11], Murthy AK et al., [19] and Markagolu et al., [24]. Also, the type of kidney disease did not influence the periodontal status indicating the lack of risk factor present in the various kidney diseases related to periodontal status [Table/Fig-2]. However the frequency of hemodialysis had significant influence on the periodontal status of the patients with a deteriorated CPI scores with the increased frequency of hemodialysis from once to twice and more than twice a week [Table/Fig-3].
Clinical parameters according to duration of dialysis
| Duration of dialysis | Mean D.M.F.T± Std. Dev. | Max. C.P.I score 1 | Max. C.P.I score 2 | Max. C.P.I score 3 | Max. C.P.I score 4 | Max. C.P.I score X | Max. L.O.A score 0 | Max. L.O.A score 1 | Max. L.O.A score 2 | Max. L.O.A score X |
|---|
| 0-3 months | 2.09±2.318 | 0 (0%) | 106 (26.5%) | 7 (1.75%) | 4 (1%) | 4 (1%) | 75 (18.75%) | 38 (9.5%) | 4(1%) | 4 (1%) |
| 4-6 months | 2.00±2.619 | 0 (0%) | 27 (6.8%) | 0 (0%) | 0 (0%) | 0 (0%) | 7 (1.75%) | 17 (4.25%) | 4 (1%) | 0 (0%) |
| 7-9 months | 1.40±2.074 | 0 (0%) | 14 (3.5%) | 4 (1%) | 0 (0%) | 0 (0%) | 7 (1.75%) | 10 (2.5%) | 0 (0%) | 0 (0%) |
| 10-12 months | 3.03±5.196 | 7 (1.75%) | 85 (21.25%) | 7 (1.75%) | 0 (0%) | 12 (3%) | 55 (13.75%) | 44 (11%) | 4 (1%) | 4 (1%) |
| More than 12 months | 2.57±3.118 | 10 (2.5%) | 82 (20.5%) | 14 (3.5%) | 0 (0%) | 17 (4.25%) | 62 (15.5%) | 34 (8.5%) | 10 (2.5%) | 21 (5.25%) |
| Total | 2.46±3.552 | | | | | | | | | |
| p-value | 0.773** (not significant) | 0.331** (not significant) | 0.43** (not significant) |
Test applied -*one way ANOVA **Pearson’s correlation
Clinical parameters according to type of underlying kidney disease
| Type of kidney disease | MEAN D.M.F.T ± Std.Dev. | Max. C.P.I score 1 | Max. C.P.I score 2 | Max. C.P.I score 3 | Max. C.P.I score 4 | Score x | Max. L.O.A score 0 | Max. L.O.A score 1 | Max. L.O.A score 2 | Max. L.O.A score x |
|---|
| Hypertensive nephropathy | 2.08 ± 2.940 | 2.56% | 45.2% | 2.7% | 0% | o.8% | 75 (18.75%) | 38 (9.5%) | 4 (1%) | 4 (1%) |
| Diabetic nephropathy | 2.78 ± 2.137 | 0.8% | 17.1% | 0.8% | 0.8% | 3.42% | 7 (1.75%) | 17 (4.25%) | 4 (1%) | 0 (0%) |
| CKD | 1.83 ± 7.064 | 0% | 3.42% | 1.71% | 0% | 0.8% | 7 (1.75%) | 10 (2.5%) | 0 (0%) | 0 (0%) |
| E.S.R.D | 4.18 ± .447 | 0.8% | 11.11% | 0% | 0% | 2.56% | 55 (13.75%) | 44 (11%) | 4 (1%) | 4 (1%) |
| others | .20 ± 2.265 | 0% | 3.42% | 0.8% | 0% | 0.85% | 62 (15.5%) | 34 (8.5%) | 10 (2.5%) | 21 (5.25%) |
| p-value | 0.13 * | 0.7** | 0.5** |
Test applied -*one way ANOVA **Pearson’s correlation
Relation of frequency of hemodialysis with periodontal status of patients
| Frequency of hemodialysis | Max.CPI Score 1 | Max.CPI Score 2 | Max.C.P.I Score3 | Max.C.P.I score4 | Max.C.P.I score X |
|---|
| Once a week | 0 (0%) | 8 (66.7%) | 0 (0%) | 0 (0%) | 4 (33.3%) |
| Twice a week | 17(5.13%) | 280 (84.59%) | 26 (7.85%) | 4 (1.2%) | 4 (1.2%) |
| More than twice a week | 0 (0%) | 49 (86%) | 8 (14%) | 0 (0%) | 0 (0%) |
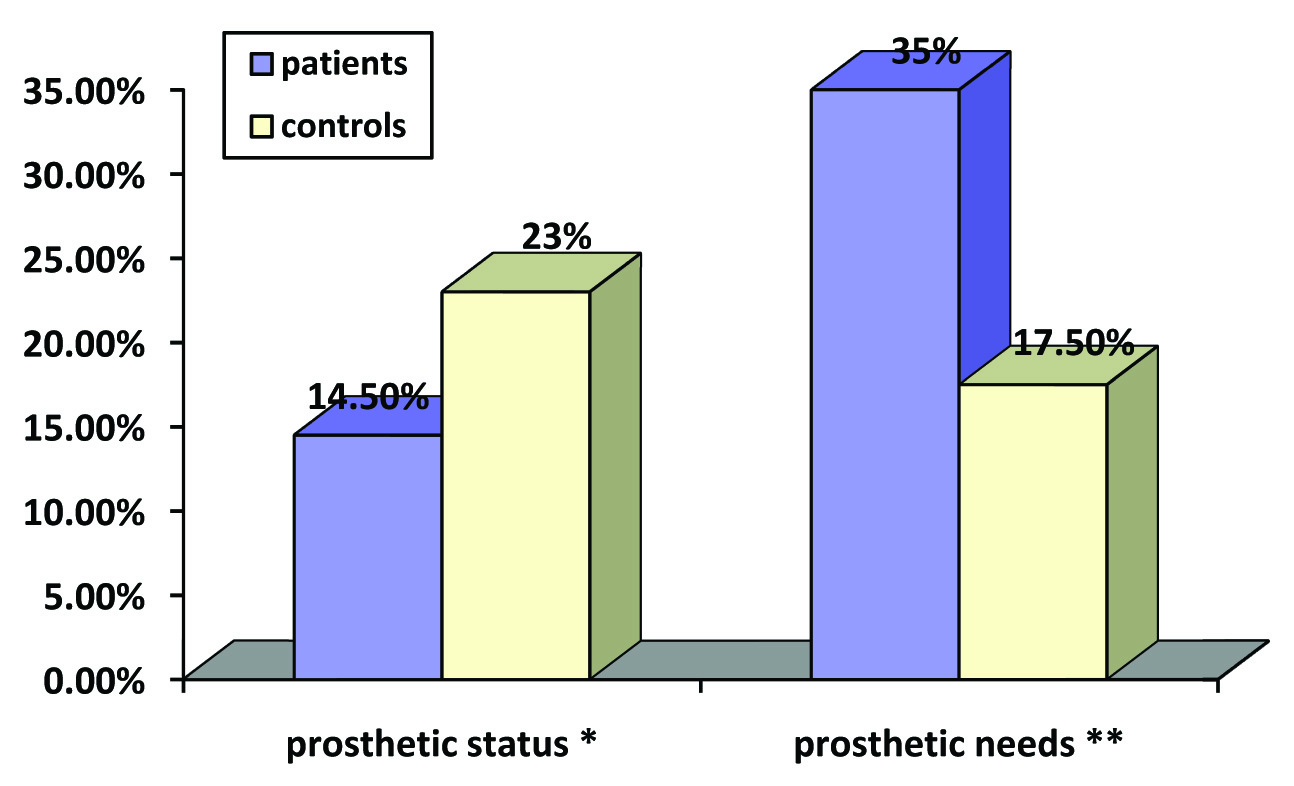
The study showed a significant existence of higher prosthetic needs (p=0.004) among the patients as compared to controls along with prosthetic status which emphasizes the need for proper dental care and rehabilitation for these patients to enjoy a satisfactory oral health [Table/Fig-4]. The prosthetic needs of the patients increased significantly with the duration of dialysis which might be explained on the basis of denied dental care by the dental practitioners owing to their compromised medical status [Table/Fig-5]. No previous literature is available regarding the prosthetic status among the hemodialysis patients; hence this study is the first attempt to assess the prosthetic status and prosthetic needs among the hemodialysis patients.
Prosthetic status and prosthetic needs among study subjects:
*p-value 0.05 (chi-square test)
**p-value 0.004 (chi-square test)
Clinical parameters according to duration of dialysis
| Duration of dialysis | Mean O.H.I scores | Prosthetic status absent | Prosthetic status Present | Prosthetic need absent | Prosthetic need absent |
|---|
| 0-3 months | 5.05 | 30 (25.6%) | 5 (4.27%) | 99 (24.75%) | 26 (6.5%) |
| 4-6 months | 5.40 | 7(5.9%) | 1 (0.85%) | 14 (3.5%) | 14 (3.5%) |
| 7-9 months | 4.52 | 5 (4.27%) | 0 (0%) | 14 (3.5%) | 4 (1%) |
| 10-12 months | 5.59 | 29 (24.7%) | 3 (2.56%) | 68 (17%) | 34 (8.5%) |
| More than 12 months | 4.89 | 29 (24.7%) | 8 (6.83%) | 62 (15.5%) | 65 (16.25%) |
| Total | 5.15 | | | | |
| P value | 0.620 *(not significant | 0.6** | 0.007 (Significant) |
Test applied -*one way ANOVA **Pearson’s correlation
Poor oral hygiene of the patients is in agreement with the studies done by Ertugrul et al., [14]. However the results are in contradiction to the findings of Parkar SM et al., [11] and Bhatsange A et al., [23] who reported poor oral hygiene among the patients undergoing hemodialysis therapy. The probable reason for the current findings could be that, the results of the previous studies were based on the assessment of oral hygiene status by OHI-S index which is a simplified index and does not give the comprehensive picture of the individual’s oral hygiene. In the present study more comprehensive assessment was made based on the full mouth oral hygiene index which gave the true picture of the oral hygiene in these patients. No significant correlation was found between the duration of dialysis and the oral hygiene status as in accordance with the previous studies by Queiroz SM et al., [25], Bhatsange A et al., [23] and Parkar SM et al., [11]. This result indicates that although these patients exhibit immunocompromised state, they are not completely immune deficient and are still able to deal with bacterial challenge [11,23]. The patients with chronic kidney disease showed maximum mean O.H.I values than the patients with hypertensive nephropathy, diabetic nephropathy, E.S.R.D and other diseases which could probably be due to long standing disease duration leading to a debilitated oral hygiene [Table/Fig-6]. Though no significant difference was found for oral hygiene status, but the calculus component was at higher level in study subjects as compared to controls and this might be due to uremic salivary pH in hemodialysis patients [Table/Fig-7].
Clinical parameters according to type of underlying kidney disease
| Type of kidney disease | Mean O.H.I scores | Prosthetic status absent | Prosthetic status Present | Prosth-etic need absent | Prosthetic need absent |
|---|
| Hypertensive nephropathy | 5.05 | 30 (25.6%) | 5 (4.27%) | 99 (24.75%) | 26 (6.5%) |
| Diabetic nephropathy | 5.40 | 7 (5.9%) | 1 (0.85%) | 14 (3.5%) | 14 (3.5%) |
| CKD | 4.52 | 5 (4.27%) | 0 (0%) | 14 (3.5%) | 4 (1%) |
| E.S.R.D | 6.52 | 29 (24.7%) | 3 (2.56%) | 68 (17%) | 34 (8.5%) |
| others | 4.89 | 29 (24.7%) | 8 (6.83%) | 62 (15.5%) | 65 (16.25%) |
| P value | 0.001* | 0.071 | 0.092 |
Test applied -*one way ANOVA **Pearson’s correlation
Comparison of calculus index scores (OHI) for patients and controls test applied –student t-test
| Calculus Index–scores (mean±Std.dev.) | p-value |
|---|
| Patients | 3.02 ±1.12 | 0.000 |
| Controls | 2.15±0.5 |
Contrary to the other dental findings, the mean caries experience of the patients (DMFT=3.552) was marginally lower than the control group (DMFT=3.559).This could be due to strict dietary restrictions in hemodialysis patients. Majority of the hemodialysis patients in the present study were diabetic and thus followed strictly monitored dietary pattern. Also, the increased alkalinity of the oral cavity in the uremic patients due to increased urea level in saliva inhibits bacterial growth and neutralizes bacterial plaque acids resulting in lower caries experience in hemodialysis patients [20].This was similar to the results of Murthy AK et al., [19] but was much less than reported by Malekmakan et al., [12]. The duration of dialysis and type of kidney disease did not show any influence on caries experience which was similar to the findings reported by Murthy AK et al., [19].
Conclusion
The present study concluded that dental health status among the hemodialysis patients gets worsened with increasing duration of hemodialysis and underlying kidney disease which might contribute significantly to morbidity and potential mortality among these patients. This warrants the need for intensified preventive oral health care modalities in these patients. The dialysis team should be encouraged to make the dental referral as early as possible, if needed and regular monthly dental checkups should be advocated. Chair side counseling can help to motivate and educate the hemodialysis patients and their caretakers regarding the importance of maintaining good oral health status. Also, dentists should become more sensitive and competent towards the dental needs of hemodialysis patients so that the rate of denied dental care due to their medical condition and the risk involved in their treatment can be lowered. Although, an appropriate sampling methodology and adequate sample size was considered for this study, our findings may be limited as only the physical measurements of dental health status were considered and the effect of biochemical markers (serum calcium, serum phosphorus) could not be assessed. Further longitudinal studies are recommended to assess the influence of hemodialysis state on clinical dental parameters along with the biochemical serum markers over duration of time so as to validate the influence of duration of dialysis therapy on dental health.
Test applied -*one way ANOVA **Pearson’s correlation
Test applied -*one way ANOVA **Pearson’s correlation
Test applied -*one way ANOVA **Pearson’s correlation
Test applied -*one way ANOVA **Pearson’s correlation
[1]. World Health Organization. Ottawa Charter for Health Promotion; Europe. 1986;1:5–16 [Google Scholar]
[2]. World Health Organization. Global status report on non communicable diseases 2010. WHO press. Italy : 1–11 [Google Scholar]
[3]. FDIFDI Policy statement-non-communicable diseases.FDI General Assembly; 2012Hong Kong 2012 26(Suppl. 1):103-107. [Google Scholar]
[4]. Nissinen A, Berios X, Puska P, Community based non communicable disease interventions: lessons from developed countries for developing onesBull World Health Organ 2001 79(10):963-70. [Google Scholar]
[5]. Cervero AJ, Bagan JV, Soriano YJ, Roda RP, Dental management in renal failure: Patients on DialysisMed Oral Patol Oral Cir Bucal 2008 13(7):E419-26. [Google Scholar]
[6]. Zhang QL, Rothenbacher D, Prevalence of chronic kidney disease in population –based studies: systematic reviewBMC Public Health 2008 8:11-40. [Google Scholar]
[7]. Klassen JT, Krasko BM, The Dental Health Status of Dialysis PatientsJ Can Dent Assoc 2002 68(1):34-8. [Google Scholar]
[8]. Jenabian N, Mirsaeed AMG, Ehsani H, Kiakojori A, Periodontal status of patient’ underwent hemodialysis therapyCaspian J Intern Med 2013 4(2):658-61. [Google Scholar]
[9]. Sullivan JD, End Stage Renal Disease Economics and the Balance of Treatment ModalitiesJ. Service Science & Management 2010 3:45-50. [Google Scholar]
[10]. Torkzaban P, Arabi R, Kadkhodazadeh M, Moradi J, Khoshhal M, Periodontal Status in Patients Undergoing HemodialysisDent J Hamadan 2009 1(1):7-10. [Google Scholar]
[11]. Parkar SM, Ajithkrishnan CG, Periodontal status in patients undergoing hemodialysisIndian J Nephrol 2012 22(4):246-50. [Google Scholar]
[12]. Malekmakan L, Haghpanah S, Pakfetrat M, Ebrahimic Z, Hasanlic E, Oral health status in Iranian hemodialysis patientsIndian J Nephrol 2011 21(4):235-8. [Google Scholar]
[13]. Joseph R, Krishnan R, Narayan V. Higher prevalence of periodontal disease among patients with predialytic renal diseaseBraz J Oral Sci 2009 8(1):14-8. [Google Scholar]
[14]. Ertugrul F, Elbek-Cubukçu C, Sabah E, Mir S, The oral health status of children undergoing hemodialysis treatmentTurk J Pediatr 2003 45(2):108-13. [Google Scholar]
[15]. Haider RS, Tanwir F, Momin IA, Oral aspects of chronic renal failurePak Oral Dent J2013(1):87-90. [Google Scholar]
[16]. World Health Organization. Oral Health Surveys-basic Methods.1997. Geneva ;4th ed.27-54 [Google Scholar]
[17]. Greene JC, The oral hygiene Index-Development and usesJ. Periodontol 1967 38:625-9. [Google Scholar]
[18]. Dumitrescu AL, Garnieta L, Guzun O, Anxiety, Stress, Depression, Oral Health Status and Behaviours in Romanian Hemodialysis PatientsRom J Intern Med 2009 47(2):161-8. [Google Scholar]
[19]. Murthy AK, Hiremath SS, Assessment of oral health status of patients undergoing renal dialysis in a hospital at Bangalore cityJournal of Indian Association of Public Health Dentistry 2005 5:35-8. [Google Scholar]
[20]. Cervero JA, Bagan JV, Soriano YJ, Roda RP, Dental management in renal failure: patients on dialysisMed Oral Patol Cir Bucal 2008 13(7):E419-26. [Google Scholar]
[21]. Bayraktar G, Dental and periodontal findings in Hemodialysis patientsOral Diseases 2007 13(4):393-7. [Google Scholar]
[22]. Dencheva M, Research of periodontal status and Treatment needs by CPITN in patients on Haemodialysis and renal transplanted PatientsJournal of IMAB – Annual Proceeding (Scientific Papers) 2009 2:1-3. [Google Scholar]
[23]. Bhatsange A, Patil SR, Assessment of periodontal health status in patients undergoing renal dialysis: A descriptive, cross-sectional studyJ Indian Soc Periodontol 2012 16(1):37-42. [Google Scholar]
[24]. Marakogolu I, Gursoy UK, Demirer S, Sezer H, Periodontal patients of chronic renal failure patients receiving hemodialysisYonsei Med J 2003 44(4):648-52. [Google Scholar]
[25]. Queiroz SM, Influence of dialysis duration and parathyroid hormone on the clinical and radiographic oral conditions of pre-transplant patients with chronic kidney diseaseBraz. J. Oral Sci 2013 12(2):10-7. [Google Scholar]