Prevalence and Recognition of Alcoholism in Emergency Department Patients
Murali Krishna1, Dharma Rao Vanamali2
1 Resident, Department of Internal Medicine, Mamata Medical College, Andhra Pradesh-507002, India.
2 Professor, Department of Internal Medicine, Mamata Medical College, Andhra Pradesh-507002, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dharma Rao Vanamali, Q.No.-7, Kinnerasani Block, MGH Campus, Giriprasad Nagar, Khammam, Andhra Pradesh-507002, India.
Phone: +(91)9849093421,
E-mail: vdrao1@rediffmail.com
Introduction: Alcohol addiction is very common in India, and is a major risk factor and etiology of many acute medical and surgical emergencies. Alcohol addiction history is frequently missed by medical team in emergency department. The present study is to investigate the prevalence of alcoholism among emergency department patients and to determine its rate of recognition by the medical team.
Materials and Methods: It is double blind cross-sectional study done in a 750 bedded tertiary care hospital (Mamata general hospital, Khammam). The study population consisted of all patients admitted in the emergency room and who stayed in the hospital for a minimum period of 24 hours between 1st March 2013 and 30th April 2013.
Results: Total of 144 patients were interviewed, 62 (43.05%) were identified as alcoholics in emergency department by treating doctors. On reviewing the records additional 11 (7.63%) were identified as alcoholics, out of which 2 (1.38%) were fulfilling the criteria for severe alcoholism.
Conclusion: Alcoholism is often not investigated and diagnosed on hospital admission. Standardized diagnostic tool will improve the identification of alcoholic patients. This is the first step to reduce alcohol consumption and offer appropriate treatment to these patients.
Audit, Alcohol, Alcoholism
Introduction
Alcoholism is a major risk factor and etiological agent for many chronic diseases (eg:- Hypertension, cirrhosis of liver) and acute medical emergencies (eg:- Stroke, acute pancreatitis) [1]. According to a study conducted by Alden J. McDonald III et. al. in United States, Emergency department visits attributable to alcohol, were at a rate of 28.7 per 1000 population [2].
According to WHO in 2004, 3.8% of all global deaths were attributable to alcohol, 6.2% for men and 1.1% for women. The harmful use of alcohol is the leading risk factor for death in men aged 15–59 [3].
Alcohol addiction is very common in India, Government statistics show that 21% of adult men and around 2% of women drink, but up to a fifth of this group about 14 million people are dependent drinkers requiring “help” [4]. There has been a rapid change in patterns and trends of alcohol use in India. Chief among them is people are beginning to drink at younger ages. The percentage of the drinking population aged under 21 years has increased from 2% to more than 14% in the past 15 years, according to studies in the southern state of Kerala by Alcohol and Drugs Information Centre India, a Non-Governmental Organisation (NGO). Alarmingly, the study found that the “average age of initiation” had dropped from 19 years to 13 years in the past two decades [4].
Inspite of increased prevalence of alcoholism, morbidity and mortality due to its intake alcohol addiction is frequently missed in the history by medical team.
Evidence shows that use of questionnaires to screen patients is helpful in identifying individuals with alcohol abuse and brief interventions during hospitalization would be effective in reducing alcohol consumption [5–9]. Therefore, the present study is to investigate the prevalence of alcoholism in emergency department patients and to determine its rate of recognition by the medical team.
Materials and Methods
This study was done on 154 emergency department patients in a tertiary care hospital (Mamata general hospital) in Khammam, for a period of two months, is a double blinded cross- sectional study done between 1st March 2013 and 30th April 2013. The study population consisted of all patients admitted in the Emergency room and who stayed in the hospital for a minimum period of 24 hours. Patients whose age was less than 15 years, who were unable to answer the pre-validated questionnaire (eg. Patients on ventilation, unable to understand or speak due to confusion) and patients not willing to participate in the study were excluded. The study protocol was approved by the ethics committee, written and informed consent was taken from all the patients.
Data collection is done in 2 steps: Interviewing the patient and review of medical records by researchers. A pre-validated questionnaire Alcohol Use Disorders Identification Test (AUDIT) [10] was used for interviewing the patients who were admitted. AUDIT consists of 10 questions about alcohol intake in last 1 year. The maximum score is 40 and a score of 8 or more signifies alcohol related disorders. A score of > 20 indicates severe dependency. The length of the interview was 5-8 minutes.
The second step of data collection was done after the patient was discharged from the hospital. Two researchers who were not involved in the interview reviewed the medical case records. The review was to search for the cases of alcoholism recorded by the medical team and the department in which the patient was admitted. A case is considered not recorded when the patient obtained a score above or equal to 8 in AUDIT and the record did not show a history of abusive alcohol consumption or similar terms (alcoholism, alcohol related disorders).
There was no contact between the researchers and the medical team, which, in turn, was blinded to the data collected in the interview.
For statistical analyses, p<0.05 was considered a statistically significant number. SPSS 18.0 software was used for the statistical analyses.
Results
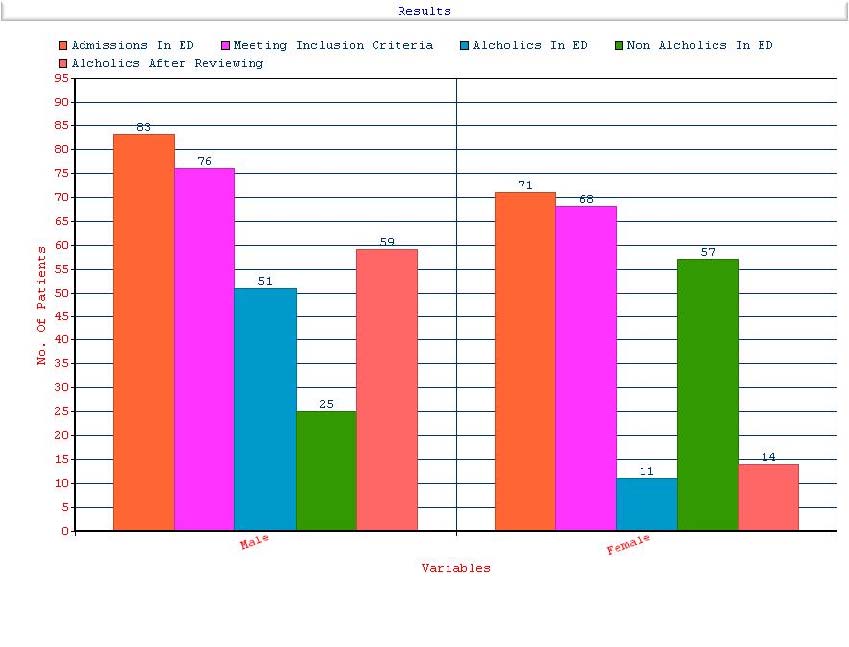
Out of the total 154 admissions in the emergency room, 10 were excluded (4 were not interested, 3 were mechanically ventilated, 2 were unable to answer the questionnaire, 1 was dead before interview) as they were not fulfilling the inclusion criteria. 144 (93.5%) patients fulfilled inclusion criteria; 62 (males- 51, females – 11; 43.05%) cases were diagnosed as alcoholics in emergency room by reviewing the medical records. 82 (m-25, f-57; 56.94%) cases not having history of alcohol mentioned in the records available in emergency room. All the cases diagnosed as alcoholics in emergency room were also identified as alcoholics on reviewing the AUDIT records. 11 (7.63%) more patients were identified as alcoholics by AUDIT. 9 (98.62%) had a score of 8 - 20, which represents mild to moderate dependency. 2 (1.38%) had a score > 20 (severe dependency) and these 2 were males [Table/Fig-1].
Shows sex distribution of cases before and after AUDIT
The mean age of study population was 51.1 ± 16.6, out of which 76 (52.7 %) were males and 68 (47.2 %) were females. The alcoholic patients were slightly younger (mean 48.5 ± 15.9 years vs. 51.1 ± 16.6 years) (p = 0.1) than the non-alcoholic patients, which is non-significant. Compared to patients with a negative AUDIT, male patients were more in patients with a positive AUDIT. General Medicine and Orthopedics were the two departments where most of the alcoholic patients were admitted. There is a clear cut difference between the AUDIT scores of patients with a positive AUDIT (mean 11.9; SD 3.4) and a negative AUDIT (mean 3.1; SD 1.8). AUDIT showed a Sensitivity of 84.93 %, Specificity of 100%. The Positive predictive value is 100 % and Negative predictive value is 86.59%. p-value is <0.0001.
Discussion
Alcohol abuse recognition is frequently missed in patients who are admitted in hospital and so the probability of early intervention is reduced. Demographic details provide risk factors and when used along with a standard diagnostic tool will significantly improve the rate of identification of alcoholic patients. AUDIT will take an average of 6 minutes to apply and 93.50% of the patients agreed to co-operate for the study. Statistics show that it is possible to quickly diagnose patients who come to emergency room have alcohol dependent, as it doesn’t take much time and the patients are often co-operative. These findings had already been verified by Horn et al., [11] Most of the alcoholic patients (97.2%) in our study shown, mild to moderately dependent (AUDIT score ranging from 8 to 20). Evidence shows that early interventions to decrease alcohol intake have good impact on the patients [12]. Moore et al., found that patients were identified as alcoholics in screening responded well to brief interventions (e.g. telling them of the diagnosis, telling them to stop drinking and making an appointment with a psychiatrist) [13]. Gentilello et al., published positive results for brief interventions at a trauma center, concerning the reduction of alcohol consumption and the reduction of risk of being readmitted for trauma [9]. He also conducted an intervention at Houston and it showed good results in getting problem drinking patients to treatment [11]. For these reasons, it seems logical that using an instrument with a greater capacity to identify at risk individuals in casualty, as opposed to the traditional medical approach that has a low sensitivity, would allow for the initiation of early intervention that may provide more positive outcomes for individuals with mild to moderate dependency on alcohol.
Conclusion
Our study has shown that identification of alcoholism in emergency department patients is often missed by medical team and by using a standardized diagnostic tool such as AUDIT for identifying alcoholism in emergency room will increase the rate of identification. Thus early identification would help in counceling these patients regarding reduction of alcohol consumption.
[1]. Marc A, Schuckit. Alcohol and Alcoholism. In: Longo DL, Fauci AS, editorsHarrison’s Principles of Internal Medicine 2011 18th edNew YorkMc Graw-Hill Companies:3546-50.Chapter 392 [Google Scholar]
[2]. McDonald AJ III, Wang N, Camargo CA, Jr, US Emergency Department Visits for Alcohol-Related Diseases and Injuries Between 1992 and 2000Arch Intern Med 2004 164(5):531-537. [Google Scholar]
[3]. Global Status report on alcohol and health. Switzerland: Alcohol And Health; 2011 [Google Scholar]
[4]. Prasad Rekha, Alcohol use on the rise in India: TheLancet 2009 373:17-18.doi:10.1016/S0140-6736(08)61939-X [Google Scholar]
[5]. Moore RD, Bone LR, Geller G, Mamon JA, Stokes EJ, Levine DM, Prevalence, detection, and treatment of alcoholism in hospitalized patientsJAMA 1989 261:403-7. [Google Scholar]
[6]. Rumpf HJ, Bohlmann J, Hill A, Hapke U, John U, Physicians’ low detection rates of alcohol dependence or abuse: a matter of methodological shortcomings?Gen Hosp Psychiatry 2001 23:133-7. [Google Scholar]
[7]. Seppa K, Makela R, Heavy drinking in hospital patientsAddiction 1993 88:1377-82. [Google Scholar]
[8]. Bien TH, Miller WR, Tonigan JS, Brief interventions for alcohol problems: a reviewAddiction 1993 88:315-35. [Google Scholar]
[9]. Gentilello LM, Rivara FP, Donovan DM, Jurkovich GJ, Daranciang E, Dunn CW, Alcohol interventions in a trauma center as a means of reducing the risk of injury recurrenceAnn Surg 1999 230:473-83. [Google Scholar]
[10]. Mendez EB, Lima MS, Olinto MTA, Farrel M, Uma versãobrasileira do AUDIT (Alcohol Use Disorders Identification Test) 1999 PelotasUniversidade Federal de Pelotas [Google Scholar]
[11]. Gentilello LM, Duggan P, Drummond D, Major injury as a unique opportunity to initiate treatment in the alcoholicAm J Surg 1988 156:558-61. [Google Scholar]
[12]. D’Onofrio G, Bernstein E, Bernstein J, Woolard RH, Brewer PA, Craig SA, Patients with alcohol problems in the emergency department, part 2: intervention and referral. SAEM Substance Abuse Task Force. Society for Academic Emergency MedicineAcad Emerg Med 1998 5(12):1210-7. [Google Scholar]
[13]. Moore RD, Bone LR, Geller G, Mamon JA, Stokes EJ, Levine DM, Prevalence, detection, and treatment of alcoholism in hospitalized patientsJAMA 1989 261:403-7. [Google Scholar]