Anterior Deep Bite Malocclusion Treated with Connecticut Intrusion Arch: Biomechanical Consideration
Safiya Sana1, Abhishek Bansal2, Laique Sami3, Roopali Tapashetti4, Shashank Gaikwad5
1 Assistant Professor, Department of Orthodontics, Al Badar Dental College, Gulbarga, Karnataka, India.
2 Post Graduate Student, Department of Orthodontics, Al Badar Dental College, Gulbarga, Karnataka, India.
3 Assistant Professor, Department of Orthodontics, Al Badar Dental College, Gulbarga, Karnataka, India.
4 Reader, Department of Periodontics, Al Badar Dental College, Gulbarga, Karnataka, India.
5 Assistant Professor, Department of Orthodontics, MGM Dental College, Navi Mumbai, Maharastra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Safiya Sana, Assistant Professor, Department of Orthodontics, Al Badar Dental College, Gulbarga, Karnataka, India.
Phone: 0-7795127340,
E-mail: sanommi_123@yahoo.com
Most Class II division 2 malocclusion manifest a severe deep bite, the orthodontic correction of deep overbite can be achieved with several mechanisms one such mechanics is true intrusion of anterior teeth. Deep overbite correction by intrusion of anterior teeth affords a number of advantages which includes simplifying control of the vertical dimension and allowing forward rotation of mandible to aid in Class II correction. It also aid in correction of a high gingival smile line. This case report presents the patient of a 14-year-old boy with Class II division 2 subdivision malocclusion treated with connecticut intrusion arch and also highlights the biomechanical aspect of this appliance. Intrusion of anterior teeth is difficult. An appropriate, effective and clinically manageable biomechanical system is required. The treatment approach shown in this case can treat the deep overbite precisely with incisor intrusion. The article shows the versatility of Connecticut Intrusion Arch and by applying the sound biomechanical principles we can execute the planned mechanics with minimal side effects.
Intrusion Arch, Deep overbite, Intrusion, Biomechanics
Case Report
A 14-year-male patient presented with a chief complaint of irregularly placed upper and lower front teeth. He had an orthognathic profile. A Class II division 2 subdivision malocclusion associated with a reduced overjet, crossbite with respect to 12, 22 and 80% of anterior deepbite. Both upper and lower incisors were upright. Both arches exhibited severe crowding. Patient had a normodivergent growth pattern [Table/Fig-1a].
(A) Pre-treatment photographs of patient with Orthognathic facial profile, 80% of deep bite. (B) After initial alignment and with CIA before intrusion. (C) After intrusion of maxillary incisors

The treatment objective in this case was to establish a Class I canine and molar relationship, achieve ideal overjet and overbite and correct the incisor lingual inclination along with maintaining the profile. The upper first and lower first premolar were extracted to relieve crowding and to align canines properly in the arch form. 0.022 × 0.028 MBT prescription was used. Alignment was done by 0.016 sectional Ni-Ti and active tiebacks. Most of the extraction space was utilized for alignment of canines. A 0.017 × 0.025 CNA beta Titanium Connecticut Intrusion Arch arch was placed to simultaneously intrude and flare the upper incisors [Table/Fig-1b]. Group A anchorage was maintained with the Connecticut Intrusion Arch during cuspid retraction. An intrusion arch was tied over the 0.017×0.025 stainless steel base archwire to simultaneously intrude canine and incisors and also to prevent incisor bite deepening due to the change in inclination of the canine during retraction [1] [Table/Fig-1c & 2]. Intrusion arch is ligated at lateral incisors and between central incisors, that creates a distal crown tipback moment on the molars to effectively control the loss of distal anchorage often associated with sliding mechanics [1] [Table/Fig-1c & 2]. Molar relation on the subdivision side was corrected by light Class II elastics. Finishing was accomplished with coordinated upper and lower .021×.025 stainless steel wire.
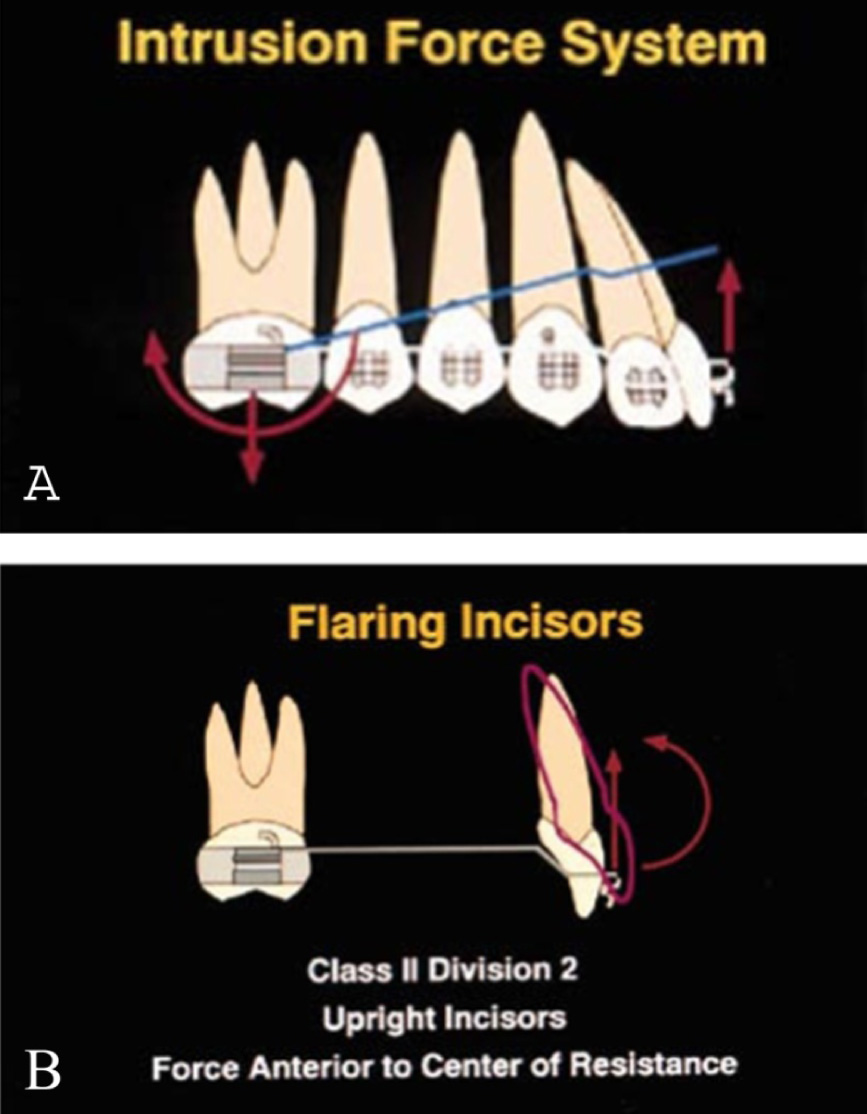
(A) Intrusion force system consists of anterior intrusive force, posterior extrusive force, and posterior tipback moment. (B) Force system for incisor flaring. CTA is not cinched back, and can be ligated directly into incisor brackets for maximum flaring [6]
Discussion
Class II malocclusions can be treated with various treatment protocols which includes variety of fixed appliances, extraction procedures, functional jaw orthopaedic appliances, extraoral traction, expansion appliances and surgery. Most class II division 2 malocclusion manifest severe deep bite. Likewise, deep overbite malocclusions need careful diagnosis, various treatment options and appliance design has been advocated for correction of excessive overbite [2]. According to Nanda [2,3] the correction of deep overbite can be achieved by four types of tooth movement, i.e., extrusion of posterior teeth, proclination of anterior teeth in lingually tipped incisors, intrusion of incisors and surgical method. Extrusion of posterior teeth results in increasing the lower anterior facial height which may not always be stable especially in hyperdivergent growth pattern. Patients with large interlabial gap, a short upper lip, long lower facial height, high gingival smile line and adult patient who have had significant bone loss are benefitted by intrusion of incisors both esthetically and functionally [4].
Basic Principles of Intrusion
Burstone [5] has listed the important principles for obtaining intrusion:
Light and constant force,
Single point of force application,
Sequential intrusion,
Good control of anchorage,
Analysis of forces and moments involved in different biomechanical situation [5].
This article describes treatment of Class II division 2 subdivision which requires premolar extraction. Class II division 2 patient are characterized by severe deepbite, lingually inclined upper and lower incisors and labial flaring of lateral incisors or canines. Because of anterior deep overbite the maxillary anterior teeth had improper gingival margins ie, excessively high gingival margins [1] [Table/Fig-3]. The treatment objectives in such cases would be extraction of upper premolars to create space for retraction of canine and simultaneous correction of deep bite with intrusion of incisors. In our case intrusion mechanics was performed with Connecticut Intrusion Arch made of CNA beta titanium archwires.
Unaesthetic gingival margin Heights, B. Gingival margin height discrepancy in anterior segment

Connecticut Intrusion Arch (CIA) [
6]
This intrusion arch was given by Ravindra Nanda. They are available as preformed with appropriate bends and available in 2 sizes: 0.016″ × 0.022″ and 0.017″ × 0.025″ with anterior dimension of 34 mm for maxillary arch and 28 mm for mandibular arch. Connecticut Intrusion Arch can deliver a force of 35-40 g in patient with average arch length. It is made of nickel titanium alloy because of its unique properties i.e., shape memory, springback and low load deflection rate delivering light continuous force. It incorporates the characteristics of the utility arch as well as those of conventional intrusion arch. It is not only used for absolute intrusion of anterior teeth but also can be used for class II correction (molar tipback), preparation of posterior anchorage, proclination of incisors, correction of minor open bites, leveling of anterior occlusal cants and finishing. It works on the V-bend principle which lies just anterior to molar bracket. When arch wire is activated it results in force system consisting of an anterior intrusive force and a moment in the posterior region [6] [Table/Fig-4a].
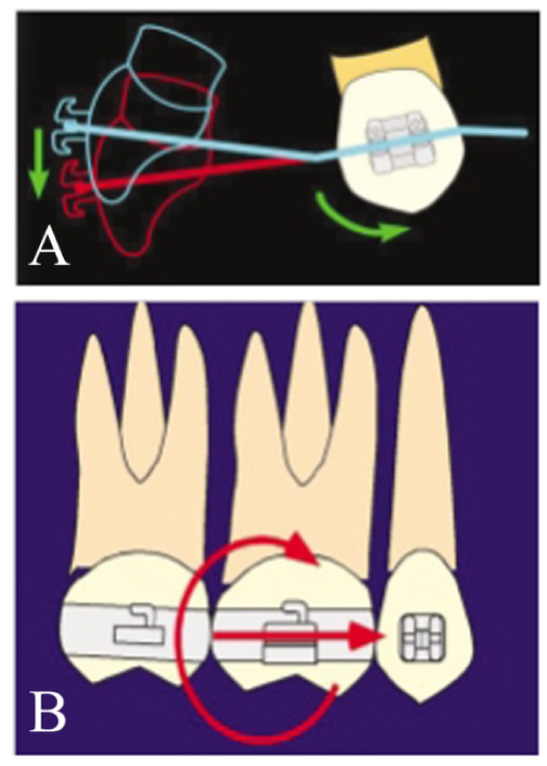
(A) Canine retraction generates extrusive effect on incisors. To counteract this tendency, intrusion arch is tied anteriorly. (B)Moment at molar counteracts mesial reactive force in anchor unit
Connecticut Intrusion Arch can be used for proclining the incisors when needed without any side effects on adjacent teeth, i.e. in Class II division 2 cases. Here intrusion arch should not be cinched distal to molar tube, so that it will slide forward through the molar tube and incisors will flare [Table/Fig-4b]. Full engagement in the incisors brackets will create moment for lingual root torque that will flare incisors even more [1,6].
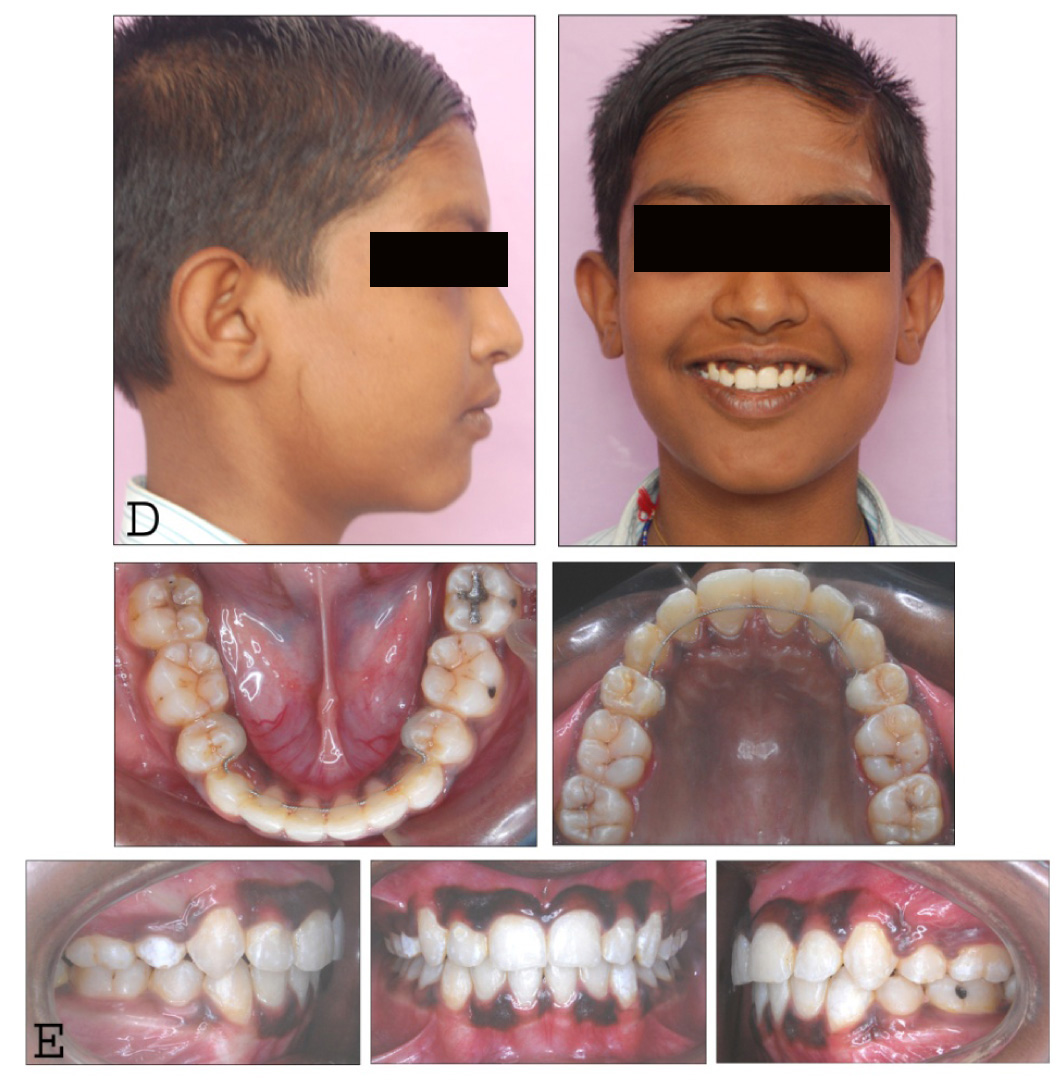
Our treatment objective was to attain ideal overjet, overbite with maintenance of facial balance. After treatment, a Class I canine and molar relationship was achieved, with proper incisor lingual inclination. Post treatment facial photograph showed fairly good results with pleasant smile, improved gingival smile line and reduced gingival display [Table/Fig-5]. According to Nanda deep overbite can be corrected by genuine intrusion of the anterior teeth, extrusion of the posterior teeth or a combination of intrusion and extrusion [6,7]. The type of tooth movement depends on many factors, including the growth potential of the patient, the vertical skeletal dimension, skeletal convexity, esthetics, stability of final occlusion [8]. Here deepbite correction with intrusion mechanics was desirable as this helped the patient to achieve improved gingival smile line. When planning for true intrusion mechanics the forces should be light continuous which is directed towards the root apex of the incisor, so that a successful intrusion can be achieved. This is accomplished by use of wires with low modulus of elasticity. The force magnitude must be kept to minimum to prevent any extrusion of the posterior teeth [9]. Connecticut Intrusion Arch here is fabricated with CNA Beta titanium provides light continuous force distribution and remains active for long duration. In the present case report number of reactionary units is increased by including premolars, Ist and 2nd molars so as to reduce the extrusive force on the reactionary unit [10]. Another added advantage of this technique is anchorage control. As seen in present case report the intrusion arch was tied over the stainless steel base wire that creates a distal crown tipback moment on the molars. These mechanics is ideal for cases where anchorage is critical [1,6]. Low forces also helps in minimizing root resorption.
(D,E) Post-treatment photograph with finished occlusion showing overbite correction, excellent anchorage control in upper arch and improvement in gingival margin height
Conclusion and Clinical Implications
Intrusion of incisors is difficult. Deep overbite correction by intrusion of anterior teeth offers a number of advantages including simplifying control of the vertical dimension, and prevents downwards rotation of mandible to aid in Class II correction. As said by Nanda applying sound biomechanical principles to the planned mechanics we can achieve predictable results with minimal side effects. Connecticut Intrusion Arch is versatile, simple in design and requires minimal auxiliary hardware; make it an ideal addition to the armamentarium of the busy clinician.
[1]. Uribe F, Nanda R, Treatment of Class II Division 2 Malocclusion in AdultsBiomechanical consideration 2003 37(11):599-606. [Google Scholar]
[2]. Kim SH, Park YG, Chung K, Severe Class II Anterior bite malocclusion treated with a C-lingual retractorAngle Orthod 2004 74:280-5. [Google Scholar]
[3]. Nanda R, Correction of deep over bite in adultsDent Clin North Am 1997 41:67-87. [Google Scholar]
[4]. Dermaut LR, De Pauw G, Biomechanical aspects of Class II mechanics with special emphasis in deep bite correction as part of the treatment goal. In : Nanda R edBiomechanics in clinical Orthodontics 1997 Philadelphia, PaW.B. Saunders Co:86-98. [Google Scholar]
[5]. Burstone C, Deep overbite correction by intrusionAm J Orthod Dentofac Orthop 1977 72:1-22. [Google Scholar]
[6]. Nanda R, Marzban R, Kuhlberg A, The Connecticut Intrusion archJ Clin. Orthod 1998 32:708-15. [Google Scholar]
[7]. Proffit WR, Contemporary orthodontics 1999 3rd edSt LouisMosby:200-1. [Google Scholar]
[8]. Horiuch Y, Horiuch M, Soma K, Treatment of severe Class II division 1 deepoverbite malocclusion without extractions in an adultAm J Orthod Dentofacial Orthop 2008 133(4):S121-9. [Google Scholar]
[9]. Karanth DHS, Shetty SV, Comparative study of various Intrusion archesJ Ind Orthod Soc 2001 34:82-91. [Google Scholar]
[10]. Nanda R, Upadhyay M. Skeletal and dental consideration in orthodontic treatment machanics: a contemporary view. As cited from URL- http://EJOOxfordJournals.org/. on 24th Oct, 2013 [Google Scholar]