Prevalence of Malocclusion and Need for Early Orthodontic Treatment in Children
R. Ramachandhra Prabhakar1, R. Saravanan2, M.K. Karthikeyan3, C. Vishnuchandran4, Sudeepthi5
1 Professor and H.O.D, Department of Orthodontics, Thaimoogambigai Dental College, Chennai, India.
2 Professor, Department of Orthodontics, Thaimoogambigai Dental College, Chennai, India.
3 Professor, Department of Orthodontics, Thaimoogambigai Dental College, Chennai, India.
4 Senior Lecturer, Department of Orthodontics, Thaimoogambigai Dental College, Chennai, India.
5 Post Graduate, Department of Orthodontics, Thaimoogambigai Dental College, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. R. Ramachandran Prabhakar, Professor and H.O.D, Department of Orthodontics, Thaimoogambigai Dental College, Chennai-600095, India.
Phone: 9444468399,
E-mail: dr.ramachandra.prabhakar@gmail.com
Background: With the advent of functional appliances and orthopedic appliances the elimination and correction of skeletal and dental discrepancies has been much reduced. Most orthodontists agree that elimination of oral habits and orthopaedic treatment of class 3 malocclusion and posterior cross bites deserve treatment at an early age. Early treatment was proposed along the lines of “catch them in the young”, and “you see it, you treat it” is the main ideology of Early Orthodonticc Treatment (EOT). Furthermore, the majority of children have habits driving the malocclusion. Mouth breathing, tongue thrusting and incorrect swallowing patterns are all known causes of malocclusion and poor facial growth.
Aims: To evaluate the prevalence of dental feature that might result in malocclusion and need for early orthodontic treatment.
Settings and Design: Groups of 532 school going children were selected and complete case history was taken and were categorized based on the type of malocclusions, dental features that can predetermine need for early orthodontic treatment. Statistical analysis used.
Results: The results shows the increase in prevalence of malocclusion and the dental features that gives clues for an orthodontist to frame up his treatment modalities not just for corrective orthodontics but for also preventive and interceptive orthodontics.
Conclusion: Angle’s Class I malocclusion is most commonly seen malocclusion followed by class II division 1 malocclusion followed by Angles class II division 2 malocclusion. In angle’s class I malocclusion, incidence of crowding is more followed by proclination of anterior teeth. There is no significant difference between incidence of malocclusion in males and females. The children who needed immediate orthodontic care were more than the children who doesn’t need an orthodontic treatment. Need for increase of awareness programs is required in order to educate the people about the early orthodontic treatment.
Early orthodontic intervention, Growth modification, Malocclusion prevalence
Introduction
The American Academy of Orthodontists (AAO) recommends that children should have an orthodontic examination by age 7 — for two very good reasons. One reason, it takes an expert to tell if a child may or may not develop malocclusion. The second reason for an early exam is that many conditions are easier to treat at early stage, when children’s natural growth processes are intense. A consensus definition of early treatment holds it as treatment started in primary or mixed dentition to enhance the dental and skeletal development before the eruption of permanent dentition [1]. Benefits of EOT include Minimizing severe protrusion, Correcting dental and skeletal malformation, Reducing severe over jet, Creating space for erupting permanent teeth, Modifying aberrant muscle morphology, Reducing the second phase of treatment. So, the aim of the study is to evaluate the prevalence of the dental features that are possibly seen in young patients that in future possibly lead to malocclusion and bring awareness to the children parents about the various non invasive treatment modalities available in present days.
Subjects and Methods
A total of 532 school children (252 girls and 280 boys) of age group 7-13 years were selected from the urban areas near maduravoyale in Chennai and consent was taken from government higher secondary school and from then children parents.
Three certified orthodontists were asked to assist in screening of all the children and the complete dental history which included family history, habits, and childhood diseases, previous dental and medical history was recorded. A total number of 337( 164 girls and 173 boys) having malocclusion who needed orthodontic treatment were grouped.
Inclusion criteria
Only children with informed and approved consent were only taken. Only Subjects with mixed dentition were only included.
Exclusion criteria
Children presented with permanent dentition were not considered.Patients who were currently taking or who took orthodontic treatment were not chosen for the study.
Results
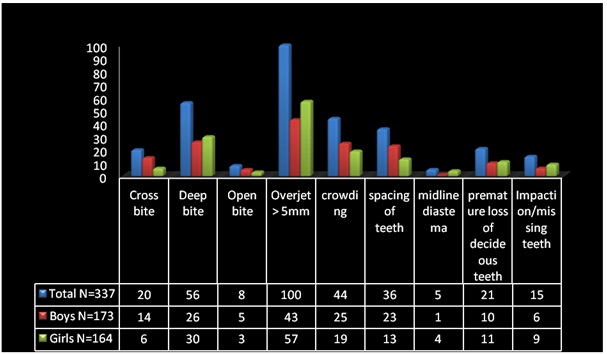
The distributions of the ages were 65.4% were 11-13 years of age and 34.6% were 8-10 years of age. There were no significant differences in distribution of malocclusion based on genders. After statistic analysis there was wide difference between the children who needed orthodontic treatment (63.4%) and children who doesn’t need orthodontic treatment, the list dental features and their prevalence’s are shown in [Table/Fig-1].
Shows variations in different dental features seen during the survey excluding the dental features of children presented with dental habits
The incidence of malocclusion tends to be high regarding Angle’s class I malocclusion (>by 21.8%) followed by Angle’s class II division 1 malocclusion (> by 17.2%) followed by Angles class II division 2 (>by 5.0%) followed by Angle’s class III malocclusion [Table/Fig-2]. Significance of habits was represented in [Table/Fig-3].
Shows types of malocclusion, n refers to total number of children and * refers to inclusion of habits
| Type of Malocclusion | Total | Boys | Girls |
|---|
| n | % | n | % | n | % |
|---|
| Class I Malocclusion | 183* | 48.5% | 97 | 25.7% | 86 | 22.8% |
| Class II Division 1 Malocclusion | 101* | 26.7% | 48 | 12.7% | 53 | 14.05% |
| Class II Division 2 Malocclusion | 36* | 9.5% | 17 | 4.5% | 19 | 5.03% |
| Class III Malocclusion | 17* | 4.5% | 11 | 2.9% | 6 | 1.5% |
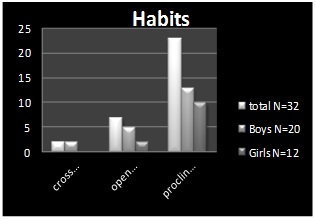
Prevalence of habits and n refers to number of children presented with habits
There is no radiological evidence for impaction but according to the chronological age we considered it to be either an impaction or missing teeth [Table/Fig-4].
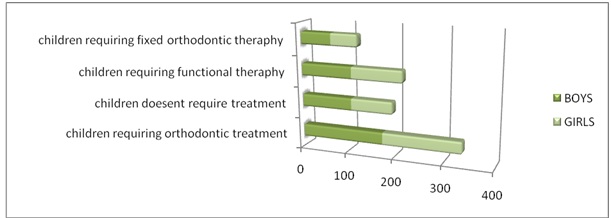
Chart shows the children in necessity of orthodontic treatment and type of orthodontic treatment
Discussion
Our study showed the number of children who has malocclusion and does need a immediate orthodontic treatment was approximately 63% greater to the children who doesn’t need orthodontic treatment which is similar to a study conducted in southern India, in Bangalore by Usha mohan das et al.,[2] and Prasad AR and Savadi [3].
The prevalence of angles class I malocclusion was more compared to the other malocclusions. Overall statistics state that proclination is the severe type of dental feature seen in most of the children (33.7%) which is similar to the studies conducted in south India by Prasad et al., [3] Nataraja rao et al., [4] and Das et al., [2], class I malocclusion had the more prevalence. In this study it was clear that the children who have oral habits were also present in a considerable ratio that definitely needs an immediate orthodontic care and awareness about EOT. A study conducted by Miriam shalish et al., [5] on 432 patients, more than 1/3rd of the patients required EOT and another study conducted by Ragavendra manjunath Shetty et al., [6], 33.3% of children had oral habits and 38% on the Survey conducted by Deepak. P Bhayya [7].
Heidi Kerosuo et al., [8], in his study concluded that early orthodontic treatment has a good long term stability than delayed orthodontic treatment.
Conclusion
The results clearly shows the increase in prevalence of malocclusion and the dental features that gives clues for an orthodontist to frame up his treatment modalities not just for corrective orthodontics but for also preventive and interceptive orthodontics. The study also emphasis the need for awareness brought to the children’s parents about early orthodontic treatment (EOT).
[1]. Thomas Rakosi, Thomas M, Graber:textbook of orthodontic and dentofacial orthopedic treatmentTIS 2009 (1):18 [Google Scholar]
[2]. Das Usha Mohan, Venkatasubramanian Reddy Divya, Prevalence of malocclusion among school children in Bangalore, IndiaInternational journal of clinical pediatric dentistry 2008 1(1):10-2. [Google Scholar]
[3]. Shivaratna Prasad AR, Epidemiology of malocclusion a report of a survey conducted in Bangalore cityJ Ind Orthod Soc 1971 3(3):43-55. [Google Scholar]
[4]. Rao DB, Hegde AM, Munshi AK, Malocclusion and orthodontic treatment need of handicapped individuals in South CanaraIndia Int Dent J 2003 53:13-8. [Google Scholar]
[5]. Miriam Shalish, Prevalence of dental features that indicate a need for early orthodontic treatmentEur J orthod 2013 34(4):454-9. [Google Scholar]
[6]. Shetty Raghavendra Manjunath, Oral Habits in children of Rajnandgaon, Chhattisgarh, India- A prevalence study internationalJournal of Public Health Dentistry 2013 4(1):1-7. [Google Scholar]
[7]. Bhayya Deepak P, Shyagali Tarulatha R, Prevalence of Oral Habits in 11–13 year-old School Children in Gulbarga city, IndiaVirtual Journal of Orthodontics 2009 8(3):1-4. [Google Scholar]
[8]. Heidi Kerosuo, Outcome and long-term stability of an early orthodontic treatment strategy in public health careEur J Orthod 2013 35(2):183-9. [Google Scholar]