Torsion- of Para-Ovarian Cyst Resulting in Secondary Torsion of the Fallopian Tube: A Cause of Acute Abdomen
Jaya Kundan Gedam1, Disha Andhiwal Rajput2, Minal V Bhalerao3
1Associate Professor, Department of Obstetrics & Gynaecology,ESI-PGIMSR, MGM Hospital,Parel, Mumbai, Maharashtra, India.
2Associate Professor, Department of Obstetrics & Gynaecology,ESI-PGIMSR, MGM Hospital,Parel, Mumbai, Maharashtra, India.
3Senior Resident, Department of Obstetrics & Gynaecology,ESI-PGIMSR, MGM Hospital,Parel, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jaya Kundan Gedam, ESI-PGIMSR, MGM Hospital, Parel, Mumbai-12, Maharashtra, India.
Phone: 08652812224, 09920353513,
E-mail: jayagedam@gmail.com
A 32-year-old woman presented with abdominal pain in the left lower quadrant, of one day’s duration. Ultrasonography of the abdomen revealed a cystic structure in the right adnexa, probably with torsion. Computerized tomography of abdomen and pelvis showed a large pelvic cyst which arose most likely from the left ovary. An urgent laparotomy was done, which however showed a twisted para-ovarian cyst with a twisted fallopian tube on the left side. The para-ovarian cyst was removed along with left sided fallopian tube and the patient made an uneventful recovery. Torsion of a para-ovarian cyst and fallopian tube is rare, but it should be considered in the differential diagnosis of acute abdomen in women who are in the reproductive age group.
Twisted, Salpinx, Abdominal Pain, Para-ovarian cyst
Case Report
A 32-year-old woman, para one, presented to the Emergency Department with complaint of left lower abdominal pain of one day’s duration. The pain was spasmodic, radiating to the back, and it was accompanied by giddiness and vomiting. There was no history of fever, fainting attacks, bowl or urinary complaints. She had a history of polymenorrhagia and dysmenorrhoea which had been present since the past two years. Her last menstrual period had occurred 13 days ago and she was not using any contraceptives. The patient’s obstetric history included one live birth which had been delivered by lower segment caesarean section eight years ago.
On examination, her general condition was found to be stable. She was afebrile, her pulse rate was 90/minute and regular, and her blood pressure was 120/80 mm Hg. She was well-hydrated. Mild pallor was present. Per abdominal examination was normal, except for slight tenderness in the left iliac fossa. On per speculum examination, the cervix and vagina were found to be healthy and there was no abnormal discharge. Her per vaginal, bimanual examination revealed an anteverted bulky uterus which was firm, non-tender and mobile. A tense, tender, cystic mass which was sized about 10 x 8 x 8 cms was felt separate from the uterus, in the anterior and right fornix. The left fornix was free and tender.
Investigations revealed haemoglobin of10.6g/dl and a total leukocyte count of 11900 cu/mm. The differential leukocyte count was within normal limits and urine pregnancy test was negative. On doing ultrasonography of the abdomen, the uterus was found to be bulky in size. There was an anechoic cystic mass which was 10 x 8 x 8 cms in size, which was seen on the right side of the uterus. The left ovary could not be visualized separately. The right ovary was cystic and it measured 3 x 3 cms in size. There was no free fluid in the pouch of douglas. A provisional diagnosis of a twisted left ovarian cyst was made. Computerized tomography (CT) scan of the abdomen and pelvis suggested a large pelvic cyst which arose most likely from the left ovary [Table/Fig-1] .
An urgent laparotomy was done. Per operative findings revealed a bulky uterus which was normal in appearance. Bilateral ovaries and the right fallopian tube appeared to be normal. A left- sided para-ovarian cyst (fimbrial cyst) which measured 10 x 8 x 8 cm was observed [Table/Fig-2] . It was twisted, congested, tense and dark in appearance. The left-sided Fallopian tube (salpinx) had stretched over it and it had undergone torsion around its pedicle. It appeared to be distended and was bluish black in colour. The para-ovarian cyst was removed, along with the left sided fallopian tube. The post-operative period was uneventful. Histopathology revealed a haemorrhagic para-ovarian cyst with an oedematous fallopian tube, with haemorrhage in its lumen.
Computerized tomography scan of abdomen and pelvis showing large pelvic cyst (arrow) most likely arising from left ovary

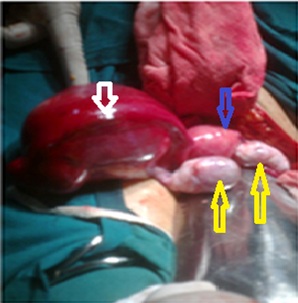
Per-operative photograph showing left-sided para-ovarian cyst (white arrow), both ovaries (yellow arrows) and uterus (blue arrow)
Discussion
Para ovarian cysts represent approximately 10% of all adnexal masses [1]. Isolated torsion of a fallopian tube or a para-ovarian cyst is rare, but it has been reported in literature and therefore, making a diagnosis is often difficult and delayed [2]. It is usually seen in women who are in the reproductive age group [3]. Being an uncommon surgical emergency with no definitive diagnostic signs, its diagnosis is often delayed, which results in causation of irreversible damage to the fallopian tube. Surgeons should be aware of this condition, so that an early diagnosis can be made and a conservative surgery, if possible, with salvage of the fallopian tube can be done. Complications of para-ovarian cysts, which have been described, include torsion (2-16%), haemorrhage, rupture, secondary infection and neoplastic transformation (2.9%). Torsion of para-ovarian cysts is 3 times more common in pregnant women, probably due to the rapid growth spurt. Physicians need to maintain a high index of suspicion for this uncommon and often difficult to diagnose cause of abdominal pain [4].
Acknowledgement
We would to thank Dr Preeti Shanbag, Professor of Paediatrics, for guiding us, and Dr. Vandana Laheri, Acting Dean, for permitting us to publish this manuscript.
[1]. Kiseli Mine, S Gamze, Caglar Clinical diagnosis and complications of paratubal cysts: review of the literature and report of uncommon presentations.Archives of Gynecology and Obstetrics 2012 285(6):1563-9. [Google Scholar]
[2]. Vijayaraghavan S. Boo Patchy, Senthil Sathiya, Isolated torsion of the Fallopian tube.J Ultrasound Med 2009 28:657-62. [Google Scholar]
[3]. Khawaja Bilges, Qazi Rohan Arab, Twisted right fimbrial cyst (Paraovarian cyst)-Journal of Surgery Pakistan (International) 2009 :14-4. [Google Scholar]
[4]. M Puri, K Jain, K Negi, Torsion of para-ovarian cyst: a cause of acute abdomen.Indian J Med Sci. 2003 57:361-2. [Google Scholar]