Retrocaval Ureter: An Innocent Bystander
Gosavi VS1, Hombalkar NN2, Dhandore PD3, Mody NB4, Bankar SS5
1 Honorary Associate Professor, Department of Surgery, Government Medical College, Miraj, Maharashtra, India.
2 Associate Professor, Department of Surgery, Government Medical College, Miraj, Maharashtra,India.
3 Assisstant Professor, Department of Surgery, Government Medical College, Miraj, Maharashtra, India.
4 Ex-registrar, Department of Surgery, Government Medical College, Miraj, Maharashtra, India.
5 Ex-registrar, Department of Surgery, Government Medical College, Miraj, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bankar SS, Ex-registrar, Department of Surgery, Government Medical College, Miraj, Maharashtra, India.
Phone: 9545048508,
E-mail: sanketbankar23@gmail.com
Retrocaval ureter is a rare congenital anomaly, with the ureter passing posterior to the inferior vena cava. Though it is a congenital anomaly, patients do not normally present with symptoms until the 3rd and 4th decades of life, which result from a hydronephrosis. We are presenting a case of 45-year-old lady who had right flank pain and dysuria, which were associated with right hydroureteronephrosis. Diagnosis was confirmed by doing Intravenous Pyelogram (IVP) and patient underwent an open surgical repair of the anomaly.
Retrocaval ureter, Flank pain, Hydroureteronephrosis, IVP
Case Report
A 45-years-old lady presented with right lumbar pain and dysuria since one year. On per abdominal examination, tenderness was found to be present on right side, with no palpable lump. The clinical diagnosis was renal colic with UTI.
On further evaluation, her haematological and biochemical profiles were found to be normal. Ultrasonography revealed a right sided, moderate to severe pelvicalyceal dilatation, with a proximal 1/3rd hydroureter. IVP showed hydronephrosis with a proximal third hydroureter, with dilated segment showing a typical ‘S’ shaped or a fish hook deformity [Table/Fig-1]. Diagnosis was Type 1 [Table/Fig-2] Right Sided Retrocaval Ureter and the patient was planned for surgery.
Pre-operative IVP-‘S’ shaped deformity

classification of retrocaval ureter
| Type 1 | Type 2 |
|---|
| More common. | Less common. |
| Ureter crosses at the level of 3rd lumbar vertebra. | Ureter crosses at the level of renal pelvis. |
| ‘S’ shaped or fish hook deformity. | Sickle shaped deformity. |
| Marked hydronephrosis. | Less hydronephrosis. |
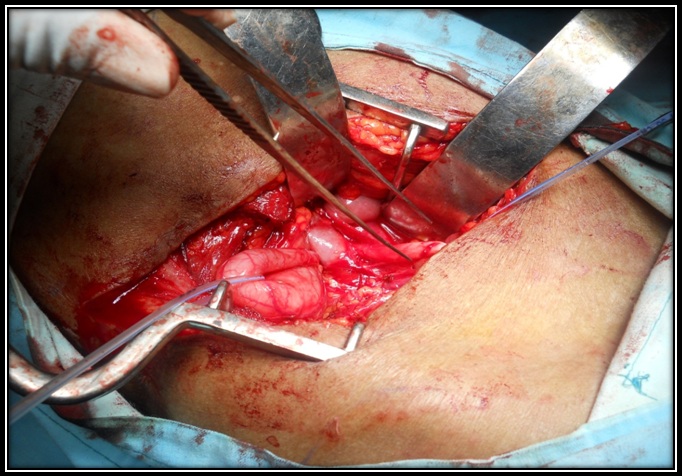
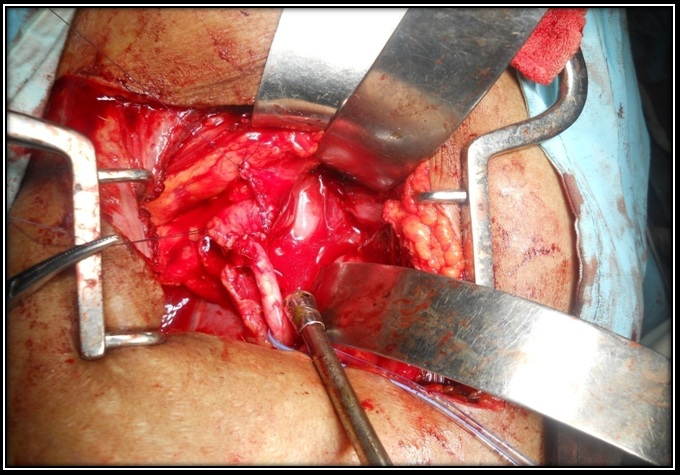
Abdomen was opened by making a retroperitoneal approach. Evidence of dilated pelvis and & ‘S’ shaped deformity of ureter was found, which was passing dorsal to IVC [Table/Fig-3]. Ureter was transected and it was brought anterior to IVC. Anterior transposition of ureter, with ureteroureterostomy, was done by using vicryl 4-0 [Table/Fig-4]. A double ‘J’ stent was placed across the anastomosis. A tube drain was placed and wound was closed in layers.
Ureter passing dorsal to IVC
Ureteroureterostomy done with vicryl 4-0
Post-operatively, the drain was removed on 4th post-operative day. Patient was discharged on 9th post-operative day after suture removal. Post-operative KUB confirmed the position of stent. Cystoscopy with double J stent removal was done after six weeks. An IVP which was done after stent removal showed regression of hydroureter and a hydroureter with no ureteric obstruction.
Discussion
A retrocaval ureter is a rare, congenital, urologic anomaly [1]. Although it is commonly referred to as a ‘retrocaval or a circumcaval ureter’, a more appropriate term would be ‘preureteral vena cava’, as it occurs as a consequence of the persistence of the posterior cardinal veins during embryologic development of vena cava. It was first described by Hochstteter in 1893 [1]. Its incidence is 1 in 1100 [1,2]. The M:F ratio is 2.8 :1 [1,2]. The A majority of the patients show involvement of the right ureter [3], which typically deviates medially behind the vena cava, winding about and crossing in front of it, to resume a normal course, distally, to the bladder.
A retrocaval ureter, may be asymptomatic or it may usually do not show symptoms until 3rd or 4th decades of life [4]. Flank pain, recurrent UTI, haematuria and hypertension are the initial symptoms and signs. Diagnosis is confirmed by USG and IVP. Spiral CT and MRI help to in delineatinge the anatomy clearly and non invasively. Even though CT scan is the investigation of choice today, MRI can be advantageous over CT scan, because of an accurate multiplanar analysis of the retroperitoneal structures, lack of radiation and avoidance of using an iodinated contrast [5].
Treatment is ureteroureterostomy with anterior transposition of ureter, which has been performed by using open, laparoscopic [7] and retroperitoneoscopic [8] approaches. If there is severe hydronephrosis, Anderson Hynes pyeloplasty has been advocated. Occasionally, nephrectomy may be required in the presence of a thinned out cortex, poor function or severe infection.
Conclusion
Retrocaval ureter is a congenital anomaly which presents clinically late, in the third and fourth decades of life, with very few patients developing clinical symptoms, or it may remain undiagnosed. Imaging studies are sufficient for making an accurate diagnosis of a retrocaval ureter. Treatment is surgical, which allows for correction of the anomaly, with resolution of symptoms. With advances in surgical technique and surgical equipments, great progress has been made in its diagnosis and treatment. Minimally invasive surgery may be the major trend in the future.
[1]. Walsh PC, Retik AB, Vaughan ED, Jr. Campbell’s Urology 2003 8th edPhiladelphiaW.B.Saunders:2044-8. [Google Scholar]
[2]. Heslin JE, Mamonas C, Retrocaval ureter. Report of four cases and review of literatureJ Urol 1951 65:212-4. [Google Scholar]
[3]. Sasai K, Sano A, Imanaka K, Right pelviureteric venous ring detected by CTJ Comput Assist Tomogr 1986 10:349 [Google Scholar]
[4]. Bateson EM, Atkinson D, Circumcaval ureter. A new classificationClinical Radiol 1969 20:173-7. [Google Scholar]
[5]. Uthappa MC, Anthony D, Allen C, Retrocaval ureter: MR appearancesThe British Journal of Radiology 2002 75(890):177-9. [Google Scholar]
[6]. Kenawi MM, Williams DI, Circumcaval ureter. A case report of four cases in children with review of literature and new classificationBr J Urol 1976 48:183 [Google Scholar]
[7]. Ramalingam M, Selvarajan K, Laparoscopic transperitoneal repair of retrocaval ureter: report of two casesJ Endourol 2003 17:85-7. [Google Scholar]
[8]. Gupta NP, Hemal AK, Singh I, Khaitan A, Retroperitoneoscopic ureterolysis and reconstruction of retrocaval ureterJ Endourol 2001 15:191-3. [Google Scholar]