Blood Stream Infections (BSIs) are one of the most common nosocomial infections (2 lakh cases per year), with mortality rate of 20–50%. Staphylococci are the most commonly encountered blood culture isolates [1]. 16% of it being Methicillin Resistant Staphylococcus aureus (MRSA). In India it is around 59% in adults with 29% mortality [2]. Time taken to identify and differentiate Staphylococci in blood cultures is critical to initiate empiric antibiotic therapy [3]. Identification methods should be economical and yield quick results, especially in a developing country like India. DTC is a tube coagulase tests done using the blood culture broth directly, reducing the turnaround time (TAT) by 24 hours [3]. It is simple and an inexpensive test. The potential for false positive test results have not been sufficiently studied [4]. Hence, this project was undertaken to study the efficiency of direct tube coagulase test (DTC) in comparison with slide/tube coagulase test for early detection of Staphylococcal bacteraemia in blood cultures.
Materials and Methods
Study Population
It was a prospective study conducted between January 2009 to December 2009 at Dr. B R Ambedkar Medical college & Hospital, Bangalore, India. The target population was patients admitted to a tertiary care hospital with a suspicion of Staphylococcal bacteremia. The clinical diagnosis of bacteremia was based on criteria of Bates & Herwaldt [5,6].
1. A temperature > 380C
(numbering).
Chills.
White blood cell count > 12,000 cells/mm2 with shift to the left
Initiation of specific antibiotic therapy.
Inclusion Criteria: Patients with suspected bacteremia fulfilling the above criteria for clinical diagnosis.
Exclusion Criteria: Patients already started on antibiotics were excluded from the study.
Sample Collection and Processing
Two blood cultures were collected from each patient. After taking informed consent, 5 ml of venous blood sample was collected under aseptic precautions for each blood culture and inoculated in 50 ml of BHI Broth. The two samples were drawn one hour apart from different venipuncture sites.
After 16 to 18 hours of incubation, blind subcultures were done onto Blood agar, Chocolate agar and MacConkey’s agar. Subcultures were performed by aseptically removing few drops from the culture bottle and spreading it onto agar and incubating it at 370 C overnight. Every suspicious colony was Gram stained and those showing Gram positive cocci in clusters (suggesting Staphylococci) were considered for further analysis. Culture negative bottles were then incubated for another 7 days before negative report was issued.
Direct tube Coagulase Test (DTC) [
3,
7]
The direct tube coagulase test was performed in 100 x 12-mm Pyrex glass tubes containing 1 ml of 10% pooled human plasma containing the anticoagulant EDTA. Blood culture broth which has been incubated for 18 hrs is taken and 1:10 dilution is prepared by suspending 10 drops (0.25 ml) of blood culture broth in 2.5 ml of 0.9% saline. 4 drops (0.1 ml) from a 1:10 dilution of the blood culture broth is added to the 1 ml of pooled plasma and incubated at 37°C. The tube was examined after 4 hours of aerobic incubation. It was then incubated overnight at room temperature and re-examined. The test was recorded as positive if a clot was observed at either time.
Identification of species was done by conventional biochemical tests: [8].
Slide coagulase test.
Tube coagulase test
Urea hydrolysis.
Mannitol fermentation.
Ornithine decarboxylase test.
Novobiocin (5μg) sensitivity.
Acid from mannose.
The data was recorded in Microsoft Excel Sheet and analyzed using standard statistical techniques. Sensitivity, specificity were calculated. Cohen’s kappa coefficient, a statistical measure of inter-rater agreement or inter-annotator agreement for qualitative (categorical) items, was calculated.
Result
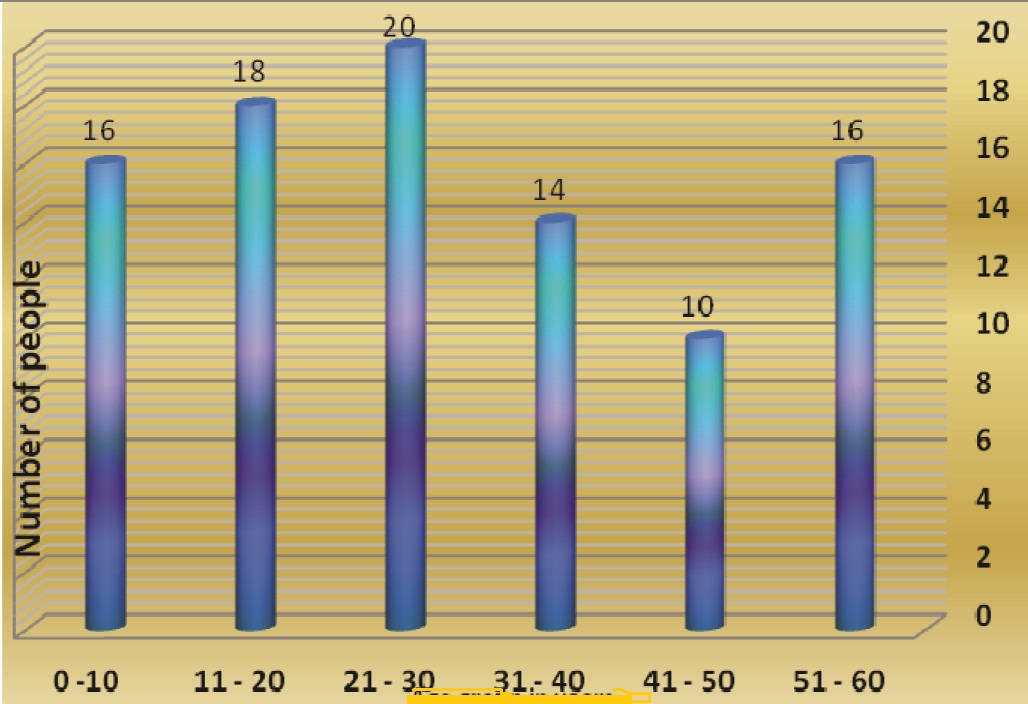
A total of 460 patients were included in the study. Of them, 94 yielded growth of Gram Positive cocci in clusters (suggesting Staphylococci) and were considered for further analysis. There were 52 males and 42 females giving a ratio of 1.2:1. The mean age was 29.6 years (SD = 16.9 years) with a range of youngest subject being 3 years to the oldest aged 60 years [Table/Fig-1]. The species of Staphylococci isolates are given in [Table/Fig-2] commonest being Staphylococcus aureus. The DTC was done on all these 94 samples. The results of this test are almost similar to the conventional tube coagulase test. The summary is presented in [Table/Fig-3]. The results of Cohen’s kappa coefficient comparison are presented in [Table/Fig-4] along with sensitivity and specificity. The coefficient of agreement is 95.6% indicating an almost perfect agreement between the conventional method and DTC.
Age distribution of Patients
Species of Staphylococci isolated
| Species | Number of isolates | Percentage |
|---|
| S.aureus | 40 | 42.5 |
| S.epidermidis | 34 | 36.2 |
| S.haemolyticus | 8 | 8.5 |
| S.cohnii | 4 | 4.3 |
| S.lugdunensis | 2 | 2.1 |
| S.saprophyticus | 2 | 2.1 |
| S.capitis | 2 | 2.1 |
| S.warneri | 2 | 2.1 |
Comparison of Direct Tube Coagulase test (DTC) with conventional method
| Conventional Tube coagulase test | Direct Tube Coagulase test | Total |
|---|
| Positive | Negative |
|---|
| Positive | 38 | 2 | 40 |
| Negative | 0 | 54 | 54 |
| Total | 38 | 56 | 94 |
Results of the comparison between Direct Tube Coagulase test and conventional method
| Kappa coefficient | 95.6% |
| Sensitivity | 95.0% |
| Specificity | 100% |
| PPV | 100% |
| NPV | 96.4% |
Discussion
In the current study, a total of 460 patients were screened, out of which, 94 (20%) positive blood cultures were identified as Staphylococcal isolates by using the Standard culture and identification methods. This is in agreement with the prevalence rate as reported by Aygen and associates [9] and Mathur and colleagues [10].
It has been well documented that patient care is improved and costs are reduced if reliable rapid coagulase results are available for blood cultures containing Staphylococci [11,12] [Table/Fig-5]. Previous studies [13,14] have examined rapid methods of Staphylococcal identification from automated blood culture instruments other than the BacT/Alert, including DTC, with varying success. In this study, the efficiency of DTC for early detection of Staphylococcal bacteremia was evaluated using the conventional slide/ tube coagulase test as the comparator/ reference.
Comparison of sensitivity and specificity with other studies
| Author | Sensitivity | Specificity | PPV | NPV |
|---|
| Qian et al., [4] | 90% | 100% | - | - |
| Chapin et al., [3] | 84.1% | 100% | 100% | 88.9% |
| Diab et al., [1] | 96% | 100% | - | - |
| Ozen et al., [12] | 100% | 95% | 100% | 96% |
| Present study | 95.0% | 100% | 100% | 96.4% |
One of methods for evaluating efficiency is to check for the agreement of results between the methods of detection. The inter-rater agreement known as the Kappa coefficient was calculated. It was found that there is almost perfect agreement between the conventional method and DTC with kappa coefficient of 95.6%. Based on the sample of 94 positive blood cultures, it was found that the DTC has sensitivity of 95.5 % and specificity of 100%. This is in agreement with other studies as shown in [Table/Fig-4].
However, a lower sensitivity (84.1%) for DTC test using undiluted blood culture broth was reported by Chapin and Musgnug [3,7] which may be due to carryover of the inhibitors of coagulation used in blood culture media.
The study gives evidences indicating that DTC can be used routinely instead of conventional methods saving a lot of time in detection. Moreover the added advantage is that DTC test can be set up at any time without waiting to run samples in batches and it demands no additional technical skills for existing laboratory staff.
As a future prospect of this study, the DTC can be put to routine use to check if the same results can be obtained on a larger number of samples. Plasma obtained with different anticoagulants must be tried to find out interfering factors giving rise to false positive or false negative results.
Conclusion
The DTC can be used for early detection of Staphylococcal bacteremia. The test has a high sensitivity of 95.5% and specificity of 100% compared to the slide/Tube coagulase test. It shows almost perfect agreement with conventional slide/Tube coagulase test with kappa coefficient of 95.6%. The test can be set up at any time without batching samples and it creates no additional technical demands for existing laboratory staff.