Introduction
Infectious diseases for ages have posed major challenge to human progress and survival and remain the leading cause of death and disability, especially in developing countries. Antimicrobials have saved countless lives and contributed immensely in the control of infectious diseases [1,2]. However, with the rise of antimicrobial resistance (AMR) many infections have started emerging and re-emerging with renewed strength. Diseases like malaria, tuberculosis, enteric fever, which were amenable to antimicrobial treatment, have started rising with development of multidrug resistant strains [3,4].Multidrug resistant enteric fever does not respond to chloramphenicol, cotrimoxazole or ampicillin treatment [1,5]. With increasing international travel and trade, medical tourism, AMR has become global problem [6].
As a result of development and spread of drug resistant pathogens, many antimicrobials, which were used successfully in the past, have fallen out of clinical use. Commonly used antimicrobials are losing efficacy to drug resistance. This review article focuses on ampicillin rise, fall and resurgence in enteric fever.
Ampicillin
Since discovery, penicillins were very effective against gram positive bacteria such as S.aureus; however, over a period of time, S.aureus acquired capacity to produce penicillin hydrolyzing enzyme, penicillinase. Attempts to extend antimicrobial activity of penicillins led to the development of ampicillin [4,7].
Ampicillin, an extended spectrum penicillin, is effective against gram positive as well as gram negative microorganisms. Also, being acid resistant, it can be given orally. It reports good minimum inhibitory concentration (MIC) against most of medically important microorganisms like S.aureus: 0.6-1 mg/L, Escherichia coli: 4 mg/L, H. influenzae: 0.25 mg/L, Streptococcus pneumoniae: 0.03-0.06mg/L. It has been used in the treatment of enteric fever, respiratory tract infections, urinary tract infections, skin and soft tissue infections [8].
Ampicillin is also been used in combination with other antimicrobials (aminoglycosides, β-lactamase inhibitor) in order to improve its efficacy, extend antimicrobial coverage and reduce development of drug resistance. These combinations are helpful in empirical treatment of wide range of complicated infection including aerobic, anaerobic and mixed infections [7].
However, following wide-spread clinical use, pathogens have acquired resistance to ampicillin. β-Lactam antibiotics bind to the penicillin-binding proteins (PBPs) of the susceptible bacteria. After a β-lactam antibiotic has attached to the PBP, the transpeptidation reaction is inhibited, peptidoglycan synthesis is blocked, and the cell dies. Pathogens can develop resistance to β-lactam antibiotics by modifying one of these steps. Various mechanisms of β-lactam resistance are reduced access to the PBPs, reduced PBP binding affinity, and destruction of the antibiotic through the expression of β-lactamase [7].
Ampicillin and Enteric fever
Enteric fever (typhoid fever), is caused by Salmonella enterica serovar Typhi (S. Typhi), a gram-negative bacterium. A very similar but often less severe disease is caused by S. Paratyphi A and rarely by S. Paratyphi B and S. Paratyphi C. It remains endemic in many developing countries. Developed countries too are reporting cases of typhoid mainly because of importation of disease by travelers. It is estimated that more than 21.7 million typhoid cases and more than 200,000 deaths occur annually, the vast majority in Asia. Additionally, an estimated 5.4 million cases due to paratyphoid occur each year [9].
Chloramphenicol was the initial antimicrobial used in the treatment of enteric fever. However, indiscriminate use of chloramphenicol over a period of time lead to development of resistant S. Typhi. Chloramphenicol resistant Salmonella typhi causing outbreaks were reported initially from Kerala, India and then from different parts of India as well as other parts of world [10].
Use of ampicillin and co-trimoxazole as an alternative to chloramphenicol in the treatment of enteric fever started in early 1970s [11]. Ampicillin provided safe and efficacious alternative to chloramphenicol, both for treatment of cases as well as carriers [4,11] and could safely be used in pregnancy and in pediatric age group also, both by oral as well as parenteral routes [4].
Widespread, non judicious use of ampicillin post chloramphenicol resistance resulted in development of multidrug-resistant Salmonella typhi (MDRST) strains. In MDRST, resistance to ampicillin was encoded by a plasmid of the H 1 incompatibility group, often in combination with resistance to co-trimoxazole, chloramphenicol, streptomycin, sulfonamides, and tetracyclines [9].
In recent past, clinical studies reported dramatic changes in occurrence of MDR Typhi strains. Even though multi-drug resistance is still common in S. Typhi, it is declining with rampant use of fluroquinolones and 3rd generation cephalosporin for the treatment [Table/Fig-1] [12].
Changing trends in incidence pattern of MDR typhi isolates over 2000-06 [12]
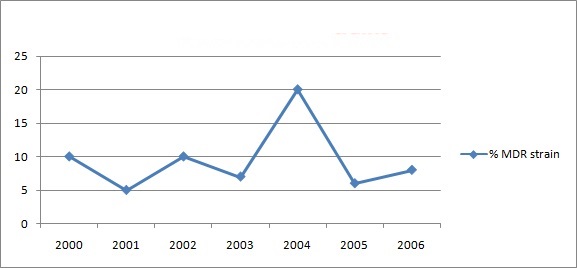
Similarly another study also reported significant decline in the MDR strains (12%) in comparison with earlier reports, indicating up to 92% of multi-drug resistance [13].
Resurgence of ampicillin in management of enteric fever
From being first line drug, ampicillin lost its efficacy due to widespread development of MDRST. However, there are reports of a remarkable reversal in the resistance pattern to ampicillin. This is reassuring in the time when there is dread of resistance development to most of the antimicrobials and dearth of development of new antimicrobials [2].
Reduction in minimum inhibitory concentration (MIC) could be an initial indicator of antimicrobial sensitivity. There are several studies, reporting reduction in MIC values of ampicillin from various parts of India indicating re-emergence of S. Typhi sensitivity to ampicillin [13–15].
Initial reports of increasing susceptibility of S. Typhi to ampicillin were published in late 1990s. In a study conducted at Bangalore, Karnataka; sensitivity of S. Typhi was found significantly higher in 1996 when compared to 1991 (63% and 80% respectively) [14].
A study conducted as a part of prospective surveillance of typhoid fever at Pondicherry, India, reported fall in ampicillin resistant Salmonella isolates to 24% from 53% in a period from 2002 to 2009 [15].
In the study conducted on isolates of S. Typhi, from 14 hospitals of Central-West India during year 2008-09, 94.5% isolates were found sensitive to ampicillin [16]. Studies from other parts of India have reported similar findings of increasing S. Typhi sensitivity to ampicillin. Reported evidence suggests that ≥90% Salmonella typhi have regained susceptibility to ampicillin [17,18].
The exact mechanism of re-emergence of sensitivity of S. Typhi to ampicillin is not known. Certain theories have been speculative. With fall in use of ampicillin in the treatment of enteric fever, selection pressure of resistant mutants was relieved. As a result of lack of exposure, S. Typhi might have lost molecular mechanisms responsible for ampicillin resistance. Ampicillin resistance in Salmonella is plasmid mediated drug resistance. The loss of high molecular weight plasmids responsible for development of resistance might have resulted in re-establishment of sensitivity. Emergence of de novo susceptible strains might be another explanation for re-emergence of the susceptibility [16].
Ampicillin has been widely used in therapeutics and as a result many microorganisms show resistance to it. Ampicillin is regaining efficacy against enteric fever pathogens [4,7]. But there are no such reported studies in other infections and may be it has not been studied systematically. Routine surveys of ampicillin sensitivity in other pathogens might show the changing sensitivity pattern. It might pave way for renewed clinical use of ampicillin.
Conclusion
Injudicious use of antimicrobials has resulted in the development of anti-microbial resistance among Salmonella pathogens. Multidrug resistant S. Typhi became non responsive to chloramphenicol, ampicillin and co-trimoxazole. Currently fluoroquinolones, cephalosporins and azithromycin are used in the therpy of enteric fever.
Decreased use of ampicillin in the treatment of enteric fever has perhaps led to the re-emergence of susceptibility of pathogens to ampicillin. Ampicillin has an excellent safety profile through vast experience of therapeutic use. Further its low cost and availability in the developing countries are added advantages. Re-emerging efficacy, undisputed safety, common availability at low cost favor use of ampicillin in the therapy of uncomplicated enteric fever. This re-emergence offers an opportunity to evaluate alternative regimens and combination therapies for treatment of drug resistant typhoid. However this requires systematic evaluation of this molecule in different infection through clinical trials or in vitro sensitivity testing.
This changing antimicrobial sensitivity pattern of Salmonella opens new avenues for future research on evaluation of current efficacy and sensitivity pattern of ampicillin in various approved indications. There is hope that other resistant pathogens may follow similar pattern and old antimicrobials will find their way in therapeutics again.
[1]. Park K, Park’s textbook of preventive and social medicine 2009 20th editionJabalpurM/s Banarsidas Bhanot Publishers [Google Scholar]
[2]. Aminov RI, A brief history of the antibiotic era: lessons learned and challenges for the future. Frontiers in MicrobiologyFront Microbiol 2010 1:134 [Google Scholar]
[3]. Cassell GH, Mekalanos J, Development of antimicrobial agents in the era of new and reemerging infectious diseases and increasing antibiotic resistanceJAMA 2001 285(5):601-5. [Google Scholar]
[4]. Brunton LL, Chabner BA, Knollmann BC, Goodman & Gilman’s The Pharmacological Basis Of Therapeutics 2011 12th edNew YorkMcGraw Hill Medical [Google Scholar]
[5]. Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, Harrison’s principles of internal medicine 2012 18th editionNew YorkMcGraw Hill Publishers [Google Scholar]
[6]. Memish ZA, Venkatesh S, Shibl AM, Impact of travel on international spread of antimicrobial resistanceInt J Antimicrob Agents 2003 (2):135-42. [Google Scholar]
[7]. Katzung BG, Masters SB, Trevor AJ, Basic & Clinical Pharmacology 2012 12th edNew DelhiTata McGraw Hill Education Private Limited [Google Scholar]
[8]. Finch RG, Greenwood D, Norrby SR, Whitley RJ, Antibiotic and Chemotherapy: Anti-infective agents and their use in therapy 2003 8th editionEdinburg LondonChurchill Livingstone [Google Scholar]
[9]. Saga T, Yamaguchi K, History of Antimicrobial Agents and Resistant BacteriaJMAJ 2009 52(2):103-08. [Google Scholar]
[10]. Rowe B, Ward LR, Threlfall EJ, Multidrug-Resistant Salmonella typhi: A Worldwide EpidemicClinical Infectious Diseases 1997 24(Suppl 1):S106-9. [Google Scholar]
[11]. Herzog C, Chemotherapy of typhoid fever: a review of literatureInfection 1976 4(3):166-73. [Google Scholar]
[12]. Verma S, Thakur S, Kanga A, Singh G, Gupta P, Emerging Salmonella Paratyphi A enteric fever and changing trends in antimicrobial resistance pattern of Salmonella in ShimlaIndian Journal of Microbiolgy 2010 28(1):51-3. [Google Scholar]
[13]. Krishnan P, Stalin M, Balsubramanian S, Changing trends in antimicrobial resistance of Salmonella enterica serovar Typhi and Salmonella enterica serovar paratyphi A in ChennaiIndian Journal of Pathology and Microbiology 2009 52(4):505-8. [Google Scholar]
[14]. Ranju C, Pais P, Ravindran GD, Singh G, Changing pattern of antibiotic sensitivity of Salmonella typhiNatl Med J India 1998 Nov-Dec 11(6):266-7. [Google Scholar]
[15]. Harish BN, Menezes GA, Preserving efficacy of chloramphenicol against typhoid fever in a tertiary care hospital, IndiaRegional Health Forum, WHO South-East Asia Region 2011 15:92-6. [Google Scholar]
[16]. Kumar Y, Sharma A, Mani KR, Re-emergence of susceptibility to conventionally used drugs among strains of Salmonella typhi in central west IndiaJ Infect Dev Ctries 2011 21(5 3):227-30. [Google Scholar]
[17]. Dutta S, Sur D B, Manna B, Bhattacharya SK, Deen, Clemens JD. Rollback of Salmonella enterica serotype Typhi resistance to chloramphenicol and other antimicrobials in Kolkata, IndiaAntinicrobail Agents and Chemotherapy 2005 49(4):1662-3. [Google Scholar]
[18]. Choudhary A, Gopalakrishnan R, Nambi PS, Ramasubramanian V, Ghafur KA, Thirunarayan MA, Antimicrobial susceptibility of Salmonella enterica serovars in a tertiary care hospital in southern IndiaIndian J Med Res 2013 137(4):800-2. [Google Scholar]