Incidental Detection of Intra-Cranial Lipoma in Patient with Quadriparesis
Quraishi SMS1, Hussain Iqbal KM2
1 Assistant Professor, Department of Medicine, Kurnool Medical College, Andhra Pradesh, India.
2 Incharge Professor, Department of Medicine, Kurnool Medical College, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. S.M.S. Quraishi, H.NO-50/761/3, Devanagar Kurnool, Andhra Pradesh-518002, India.
Phone: 9985757063,
E-mail: safu53@yahoo.co.in
Magnetic Resonance Imaging (MRI) of brain is a non-invasive investigation which is performed frequently now-a-days in clinical neurological practice. Many incidental findings may be seen on MRI brain scans, which may be of little clinical significance. Knowledge on these entities is important, for a clinician to limit unnecessary further evaluations.
Here is a description of a case of an incidentally detected, posterior peri-callosal, intracranial lipoma (a rare entity) which had occurred in a patient with quadriparesis, followed by a brief discussion on the types of intracranial lipomas and their clinical significances.
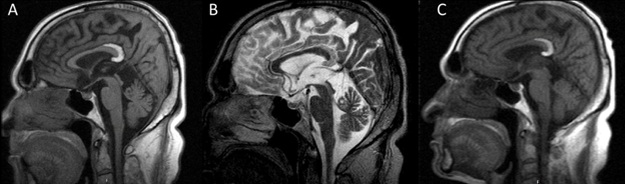
A 65-year-old male presented with weakness of both upper limbs and lower limbs of 6-months duration. On examination, his tone was found to be spastic, his deep tendon reflexes were exaggerated and he had bilateral plantar extensor. A provisional diagnosis of spastic quadriparesis was made. Magnetic Resonance Imaging of cervical spine revealed spondylosis with cord compression at the level of C4-C6 vertebral level, which explained the cause of quadriparesis. Interestingly, MRI of his brain revealed a homogenously hyperintense lesion which was noted in T1 weighted images (A), at posterior part of corpus callosum, around the splenium. The lesion was hypointense in T2 (B) images and hyper intense in FLAIR (C) images, which was suggestive of a peri-callosal curvilinear lipoma. Patient was referred to neurosurgery department and he got operated for cervical spondylosis, with significant clinical improvement after surgery.
Corpus callosum, Intracranial lipoma, Quadriparesis, Malformations
Case Report
A 65-year-old male presented with weakness of both upper limbs and lower limbs of 6 months duration. The weakness onset was insidious and it was gradually progressive, with involvement of both proximal and distal muscle weaknesses, along with stiffness. On examination, the patient was found to have normal higher mental functions. Examination of cranial nerves showed a normal picture. On doing a motor system examination, tone spasticity was noted in all the limbs and the power was found to be 4/5 and there was no clonus, with exaggerated deep tendon reflexes in all the four limbs and a bilateral plantar extensor response, with no cerebellar or autonomic nervous system involvements. A provisional diagnosis of spastic quadriparesis was made. His routine biochemistry and electrolyte panels were normal. As a part of work up, magnetic resonance imaging (MRI) of brain and cervical spine was performed. MRI of cervical spine revealed spondylosis with cord compression at the level of C4-C6 vertebral level, which explained the cause of quadriparesis. Interestingly, MRI of his brain revealed a homogenously hyperintense lesion which was noted in T1 weighted images (A), at posterior part of corpus callosum, around the splenium. The lesion was hypointense in T2 (B) images and hyper intense in FLAIR (C) images, which was suggestive of a peri-callosalcurvilinear lipoma [Table/Fig-1]. This was supposed to be an incidental finding, as the patient had no other associated symptoms or signs and as all the clinical features could be explained on basis of cervical cord compression. Patient was referred to neurosurgery department and he got operated for cervical spondylosis, with significant clinical improvement after surgery.
MRI brain shows a homogenously hyperintense lesion in T1 weighted images at posteror part of corpus callosum, around the splenium (B)- The lesion Is hypointense in T2 images (C)- The lesion is hyperintense in FLAIR Image
Discussion
Intracranial lipomas are rare tumours and they represent only about 0.1% of all intracranial tumours [1]. Intracranial lipomas can be completely asymptomatic or they may be associated with a wide variety of signs and symptoms. Asymptomatic intracranial lipomas are usually incidentally detected on computed tomography (CT) or MRI. Imaging plays a crucial role in their detection, in classifying the type of lipoma on the basis of its location and nodularity, thereby determining its clinical significance. Also, imaging is essential to detect the associated spectrum of brain malformations, the most important being those seen in the corpus callosum and the septum [2]. Corpus callosum agenesis or dysgenesis is the most frequent brain anomaly which is associated with intracranial lipoma [3]. Though lipomas, are considered to be tumours, the intracranial ones are thought to be malformations; as multiplication of lipoma cells and mass effect caused by lipomas are never observed in them [4]. Most commonly, intracranial lipomas are located in interhemisperic or pericallosal locations (45%), followed by cerebello-pontine angle (9%) and sylvian (5%) cisterns [4,5]. Pericallosal lipomas can be divided into two subgroups based on relevance of their locations and severity of associated malformations. The tubulonodular type is the first type which is characterized by nodular lesions and it can be associated with fronto-fascial abnormalities [6]. The second subgroup is the curvilinear type. Curvilinear lipomas are usually asymptomatic and they can be small or extensive. Usually, they are located posteriorly, they are of sizes which are less than 1 cm and they can be associated with hypoplasia of corpus callosum [6]. In our patient, the type of lipoma was peri-callosal curvilinear posterior lipoma with mild hypoplasia of splenium of corpus callosum. As has been suggested in the literature, there were no associated major abnormalities or any symptoms which were attributable to this lesion and therefore, it was purely a co-incidentally detected finding [7,8]. All the symptoms and signs were explained by cervical spondylosis with cord compression.
Conclusion
To conclude, our case suggests that lipomas are incidentally detected intracranial lesions among which posterior curvilinear lipomas are asymptomatic and that hence, they do not require any treatment in general.
[1]. Eghwrudjakpor PPO, Kurisaka M, Fukuoka M, Mori K, Intracranial lipomas: current perspectives in their diagnosis and treatmentBr J Neurosurg 1992 6:139-44. [Google Scholar]
[2]. Friedman RB, Segal R, Latchaw RE, Computerized tomographic and magnetic resonance imaging of intracranial lipomaJ Neurosurg 1986 65:407-10. [Google Scholar]
[3]. Macpherson RI, Holgate RC, Gudeman SK, Midline central nervous system lipomas in childrenJ Can Assoc Radiol 1987 38:264-70. [Google Scholar]
[4]. Truwit CL, Barkovich AJ, Pathogenesis of intracranial lipoma: an MR study in 42 patientsAm J Roentgenol 1990 155:855-65. [Google Scholar]
[5]. Yildiz H, Hakyemez B, Koroglu M, Yesildag A, Baykal B, Intracranial lipomas: importance of localizationNeuroradiology 2006 48(1):1-7. [Google Scholar]
[6]. Macpherson RI, Holgate RC, Gudeman SK, Midline central nervous system lipomas in childrenJ Can Assoc Radiol 1987 38:264-27. [Google Scholar]
[7]. Sommet J, Schiff M, Evrard P, Blanc R, Elmaleh-Bergès M, Pericallosal lipoma and middle cerebral artery aneurysm: a coincidencePediatr Radiol 2010 Aug 40(8):1417-20.doi: 10.1007/s00247-009-1534-9. Epub 2010 Feb 12. PubMed PMID:20151118 [Google Scholar]
[8]. Yildiz H, Hakyemez B, Koroglu M, Yesildag A, Baykal B, Intracranial lipomas: importance of localizationNeuroradiology 2006 48(1):1-7.Epub 2005 Oct 20. PubMed PMID: 16237548 [Google Scholar]