Balantidiosis: A Rare Accidental Finding in the Urine of A Patient with Acute Renal Failure
Ankit Khanduri1, Sapna Chauhan2, IVA Chandola3, BS Mahawal4, VK Kataria5
1 Assistant Professor, Department of Microbiology, Shri Guru Ram Rai Institute of Medical & Health Sciences, Patel Nagar, Dehradun, Uttahakhand, India.
2 Junior Resident 2nd Year, Department of Microbiology, Shri Guru Ram Rai Institute of Medical & Health Sciences, Patel Nagar, Dehradun, Uttahakhand, India.
3 Junior Resident 1st Year, Department of Microbiology, Shri Guru Ram Rai Institute of Medical & Health Sciences, Patel Nagar, Dehradun, Uttahakhand, India.
4 Professor & HOD, Department of Microbiology, Shri Guru Ram Rai Institute of Medical & Health Sciences, Patel Nagar, Dehradun, Uttahakhand, India.
5 Professor, Department of Microbiology, Shri Guru Ram Rai Institute of Medical & Health Sciences, Patel Nagar, Dehradun, Uttahakhand, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ankit Khanduri, Assistant Professor, Department of Microbiology, Shri Guru Ram Rai Institute of Medical & Health Sciences, Patel Nagar, Dehradun, Uttahakhand-248001, India.
Phone: 9761695633,
E-mail: drankitkhanduri@gmail.com
Balantidium coli is the only ciliated protozoan which is known to infect human and nonhuman primates. Route of infection is faecal-oral route. It is actively motile and causes mostly asymptomatic infections, or it may develop dysentery which is similar to that which is caused by Entamoeba histolytica. Here, we are describing a case of an accidental finding of B.coli in the urine of a patient who presented with acute renal failure, based on its characteristic morphology and motility which were seen on light microscopy. This is the third case of Urinary Balantidiosis which has been reported from India.
Case Report
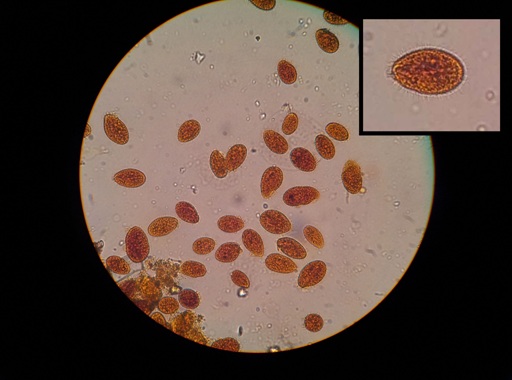
A 55-year-old female presented to Emergency Department of Shri Guru Ram Rai Institute of Medical and Health Sciences, Dehradun. Uttahakhand, with fever, malaise, anorexia of 20 days duration and oliguria of 24 hrs duration. Her fresh mid stream urine (MSU) sample was sent for routine and microscopic examinations. The urine physically appeared as smoky and mildly turbid and microscopic examination of its sediment showed a few red cells with 2-4 pus cells per HPF. Also, many ovoid to oblong ciliated parasites which were approximately 70 x 50 μm, were seen swimming rapidly across the slide [Table/Fig-1] The organism had a mouth that was located at its tapering anterior end (cystosome) and a rounded posterior end (cytopyge). Several food vacuoles, macronuclei and a few ingested RBCs were present within cytoplasm. Its body was covered with short, delicate cilia which were all of uniform length. The cilia which lined the mouth part, appeared to be longer than others. The morphology and swimming pattern were characteristic of B. coli. A few motile trophozoites of Trichomonas vaginalis were also seen. A repeat MSU sample taken from the patient showed similar organisms.
Microscopic examination showing few red cells and ovoid to oblong ciliated parasites
A complete haemogram showed microcytic hypochromic anaemia with an Hb level of 6.3 gm%. Serology done for HIV and HbsAg were negative. Her kidney functions were found to be deranged, with urea -274 mg/dl and creatinine -16.8 mg/dl. Her LFT and blood sugar were found to be within normal limits.
Her first morning faecal samples were examined for ova cysts and parasites for 3 consecutive days, all of which were found to be negative.
The patient was started on oral metronidazole and was discharged after 3 days. She was subsequently lost to follow up.
Discussion
Balantidiosis is a zoonotic disease which is caused by Balantidium coli (B. coli) and it is acquired by humans via the faecal-oral route. B. coli is the only ciliated protozoan which is known to infect humans though it is uncommon, despite its potential to have a worldwide distribution. Its worldwide prevalence is estimated to be 0.02 to 1%. Humans as well as pigs (reservoir hosts) may remain asymptomatic, or they may develop dysentery which is similar to that caused by Entamoeba histolytica. It is cosmopolitan in nature, but is mostly found in developing countries, where water sources may be contaminated with porcine or human faeces [1].
Its usual mode of transmission is ingestion of its infective cysts through water which is contaminated with porcine faeces, although a human to human transmission may also occur, but it is rare. Ingested cysts liberate trophozoites which reside and replicate by binary fission in the large bowel [1]. This patient had no history of contact with pigs, but she had a history of bathing in a pond; hence, she might have been infected through contaminated water of the pond. Many patients remain asymptomatic but some have persistent diarrhoea and a few develop dysentery. Genitourinary sites of infection, including uterine infection, vaginitis, and cystitis, are thought to occur via direct spread from the anal area or as secondary to rectovaginal fistulas which are created due to infection with B. coli [1].
The organism in this case may have invaded the urinary bladder through the colonic mucosa to or directly through the anal area. The stool examination was not contributory, probably because the patient was also suffering from diarrhoea since past 1 year, for which she had been taking metronidazole infrequently. Although in immuno compromised individuals, malnutrition and alcoholism are important risk factors for balantidiosis, our patient was HIV negative and there was no history of either malnutrition or alcoholism [2,3].
Making a lab diagnosis is relatively easy, because of its large size and spiral motility. Balantidial cysts are 40-60 microns in diameter and they are binucleate, in contrast to E. histolytica cysts which are smaller 10-20 microns and are quadrinucleate [1]. In this patient, excellent morphology of the parasite could be demonstrated in the urine sample by light microscopy. The only other ciliated parasite which has a similar morphology is Paramecium, which is non pathogenic and it can be found in contaminated water. It has also been reported to colonize urinary tracts of dialysis patients [4]. As our patient was symptomatic the organism was more likely to be B.coli in our case. Tetracycline and Metronidazole are drugs of choice for B.coli.
Not much data is available on the prevalence of urinary Balantidiosis in India or worldwide. An internet search revealed only four cases which were reported, one each from Italy and Tehran and two from India [5–8]. Though many cases of B. coli infection in stool have been reported from India, both in humans and animals, urinary balantidiosis is still a rare entity [9,10]. To the best of our knowledge this is the third case report of urinary Balantidiosis from India.
Conclusion
To conclude, B.coli is a rare urinary pathogen that can be found throughout the world. Microscopic examination of fresh urine sediments can help in easily diagnosing this large parasite, based on its characteristic morphology and rapid spiralling motility. Clean water and hygienic sanitary conditions are the most efficient strategies which can be ensured, to prevent human infections.
[1]. Schuster FL, Ramirez-Avila L, Current World Status of Balantidium coliClin Microbiol Rev 2008 21(4):626-38. [Google Scholar]
[2]. Anargyrou K, Petrikkos GL, Suller MT, Skiada A, Siakantaris MP, Osuntoyinbo RT, Pulmonary Balantidium coli infection in a leukemic patientAm J Hematol 2003 73(3):180-3. [Google Scholar]
[3]. Cermeno JR, Hernandez De Cuesta I, Uzcategui O, Paez J, Rivera M, Baliachi N, Balantidium coli in an HIV-infected patient with chronic diarrhoeaAIDS 2003 17(6):941-2. [Google Scholar]
[4]. Singh S, Dash SC, Paramecium colonizing urinary tract of a patient on dialysis: a rare entityNephron 1992 62(2):243-4. [Google Scholar]
[5]. Bandyopadhyay A, Majumder K, Goswami BK, Balantidium coli in urine sediment: report of a rare case presenting with hematuriaJ Parasit Dis 2013 37(2):283-5. [Google Scholar]
[6]. Maino A, Garigali G, Grande R, Messa P, Fogazzi GB, Urinary balantidiasis: diagnosis at a glance by urine sediment examinationJ Nephrol 2010 23:732-7. [Google Scholar]
[7]. Umesh S, Balantidium coli on urine microscopyNatl Med J India 2007 20:270 [Google Scholar]
[8]. Maleky F, Case report of Balantidium coli in human from south of Tehran, IranIndian J Med Sci 1998 52:201-2. [Google Scholar]
[9]. Singh NK, Singh H, Jyoti Haque M, Rath SS, Prevalence of parasitic infections in cattle of Ludhiana district, PunjabJ Parasit Dis 2012 36(2):256-9. [Google Scholar]
[10]. Kaur R, Rawat D, Kakkar M, Uppal B, Sharma VK, Intestinal parasites in children with diarrhea in Delhi, IndiaSoutheast Asian J Trop Med Public Health 2002 33(4):725-9. [Google Scholar]