An osteochondroma is a benign tumour of bone, which is located mainly in the metaphysis of long bones. It does not commonly occur in the scapula. On the ventral surface of the scapula, it can produce various manifestations due to mass effect. We are reporting a rare presentation of an osteochondroma at superomedial angle of ventral aspect of the scapula in a 31-year-old female. She initially presented with a painful shoulder and radiating pain in the arm. The scapular mass produced pseudo winging of the scapula and erosion of the ribs on the same side. The patient was successfully managed by open excision, using a parascapular approach. The patient had no evidence of recurrence at one year’s follow-up and is currently able to carry on her day to day activities without any discomfort.
Snapping scapula, Parascapular approach, Exostoses bursata
Case Report
A 31-year-old, right hand dominant female presented to our orthopaedic clinic, complaining of a continuous dull aching pain around right shoulder, of six months duration, which had been gradual in onset, which radiated to the ipsilateral arm, including the elbow and up to the wrist. Pain was aggravated by movements. There was an associated swelling over the right suprascapular region. She had first noticed the swelling accidentally, following a trivial injury. The swelling produced fullness over the supra scapular region. It gradually progressed in size over the duration of next six months and caused pseudo winging of the right scapula.
The right scapula was found at a slightly higher level than the left, with fullness over the superomedial angle. A non tender, cystic mass was felt over the supero medial angle of the right scapula. There was no associated regional lymph node enlargement or neurovascular deficit.
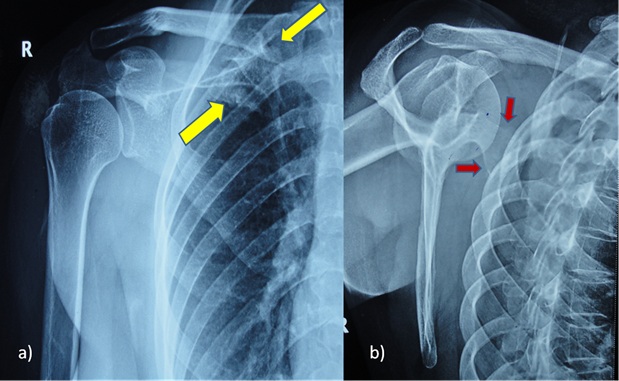
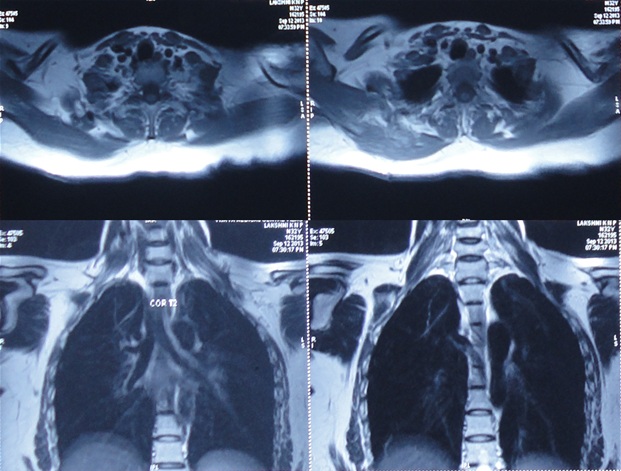
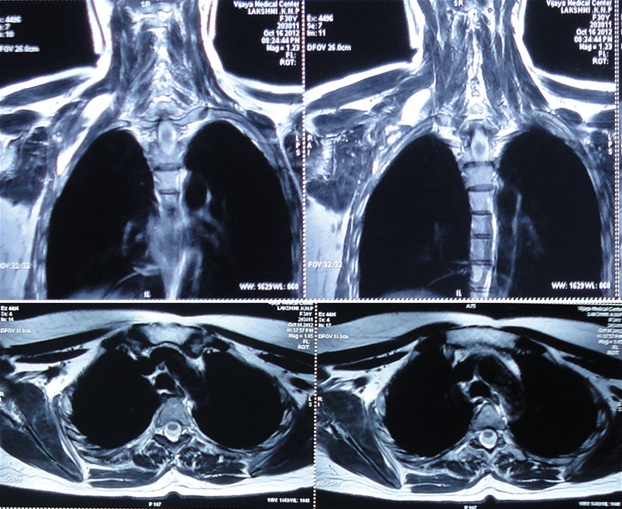
An anterio posterior view of the right shoulder joint failed to properly show the tumour mass [Table/Fig-1]. A standard Y view [Table/Fig-1] of the scapula clearly demonstrated the tumour as arising from the ventral aspect of the supreo medial border of the scapula. Ultrasound showed presence of a bursa (exostoses bursata) near the swelling. MRI showed the extent of the tumour over the superior angle of scapula [Table/Fig-2]. A diagnosis of ventral osteochondroma of the superomedial angle of the scapula was made and she was offered surgical excision [Table/Fig-3]. The surgery was primarily performed for cosmetic reasons.
a) Pre operative Radiograph of the right shoulder, antero posterior view, showing bony mass arising from the supero medial region of the scapula. b) Pre operative Standard ‘Y ‘view or lateral view of the scapula provides better delineation of the tumour mass than the AP view
Pre operative MRI defining the boundaries of the tumour mass
a) Intra operative picture showing use of para scapular approach to reach the tumour mass. b), c), d) & e) Intra opeaitive images of resected tumour. f) & g) Intra operative images following resection of tumour, showing closure of the incision site
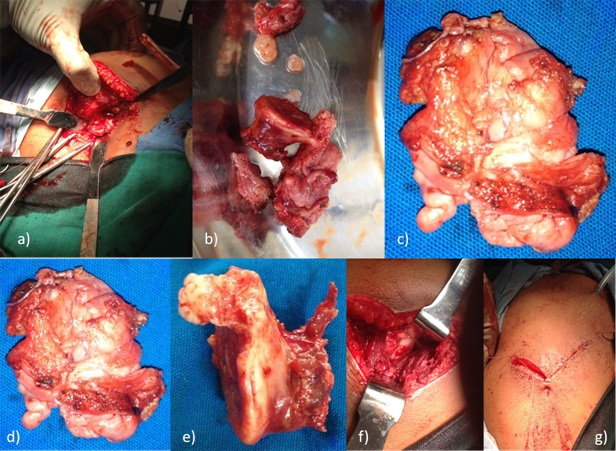
Procedure was performed under general anaesthesia with the patient in prone position. The shoulder was rotated internally, thereby lifting the medial border of the scapula away from the thoracic cage. An incision was made along the medial and superior border of the scapula (parascapular incision). A muscle splitting approach (of the trapezius and rhomboid) was used to reach the bone. No transverse cut was made in any muscle, to ensure a better, prompt post operative recovery without any functional loss.
A cauliflower shaped mass with flattening of the ventral surface, which faced the chest wall, was encountered. A pedunculated, irregular mass [Table/Fig-3] which was about 2x1x1 inches in dimension, caused erosion of the third and fourth ribs. A bursa surrounding the lesion, containing about 100 ml of straw coloured fluid, was noticed, along with two loose bodies. The mass along with its bursa was excised [Table/Fig-4]. Following excision, erosion of the third and fourth ribs was evident, which corresponded to the flattened region of the tumour.
Intra operative images showing key steps of surgery (en bloc resection of the tumour)

Macroscopically, it was a pearly white, nodular, hard mass, with its cut surface revealing spongy bone with a lobulated cartilaginous cap that was lost over the flattened region of the tumour. Microscopic examination revealed a neoplasm which was composed of bony trabeculae in which mostly fatty tissue and bone marrow intervened.
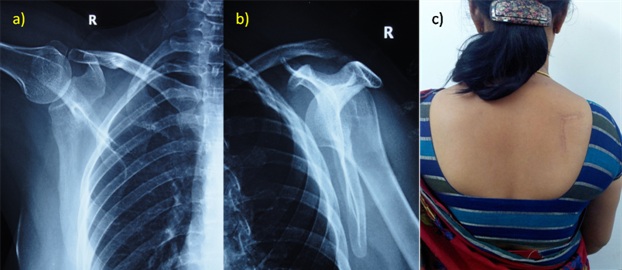
The arm was immobilized by putting it in an arm pouch for three weeks, during which period only pendulum exercises were permitted. She was later sent for a rehabilitation programme to improve her shoulder range of movements. Her symptoms resolved dramatically in the immediate post operative period. There was no recurrence of any symptoms or swelling over the course of the next one year. There was no clinical or radiological evidence [Table/Fig-5] of the tumour, following its excision. Functional range of movement of the right shoulder was found to be normal as compared to its counterpart. The patient was pain free following surgery. At one year’s follow up, the patient was symptom free and there was no evidence which suggested recurrence of the tumour [Table/Fig-6].
a) Post Operative radiograph of the right shoulder (AP view) taken following tumour resection. b) Post Operative radiograph of the right shoulder (Standard Y view) taken following tumour resection. c) Post operative clinical image of the patient showing incision scar (Para scapular incision) extending along the medial and superior border of the right scapula
Follow up MRI scan images reveal no sigs suggestive of recurrence
Discussion
Osteochondroma is the most common benign bone tumour * [1]. There are only few reports on osteochondromas which occurred at the superomedial angle of the ventral surface of the scapula [2]. Ventral osteochondromas may lead to snapping of the scapula, painful crepitus, pseudo winging and bursa formation [3] (They may present as masses). They are commonly seen in young patients, usually in those who are below 30 years of age, with male:female ratio of >1.5:1. Although proximal humerus, distal femur and proximal tibia are the commonest sites seen so far (90%), involvement of the flat bones has been reported and scapular lesions account for 4% of all described osteochondromas. Very few tumours arise from the ventral surface of the scapula and they can result in painful limitation of shoulder abduction and pseudowinging of the scapula.
The first description of a snapping scapula which was given, has been credited to Boinet, who in 1867, presented the case of a 19-year-old man who faced discomfort during scapular movements. Since then, sporadic case reports on painful scapular osteochondromas which were associated with large bursa formations have come up [4]. Around 6% of scapulae may show a hook-shaped prominence which is known as “Luschka tubercle”, at the superomedial angle [5].
The superior and inferior angles and the medial border are poorly cushioned, and osteochondromas which occur at these locations can lead to bursal irritation caused by repeated mechanical abrasion, with active shoulder motion. Large bursa formations which are associated with osteochondromas are termed as ‘exostosis bursata’, a term which was coined by Orlow [6].
A winged scapula or scapula alata is defined as a prominence of the medial border of the scapula. Winging of the scapula may be either dynamic or static. The most common tumour which is associated with static winging of the scapula is an osteochondroma. Scott et al., reported intermittent scapular winging in a teenage patient after an initial injury, that was diagnosed as an osteochondroma about a year later.
As osteochondroma may arise from the ventral surface of the scapula, it may be difficult to identify it or it may be missed on plain radiographs. Doing early advanced imaging studies with either CT or MRI scanning is imperative, to establish a diagnosis. The onset of pain in such a lesion could be caused by bursitis which overlies the osteochondroma, fracture of the stalk after a trauma or rarely by a malignant transformation. A malignant transformation should be suspected when a previously quiescent lesion seen in an adult grows rapidly; it usually takes the form of a low-grade chondrosarcoma. In such cases, the cartilage cap is usually more than 2 cm thick. A malignant transformation can be best evaluated by CT or MRI.
Surgery (an en bloc resection) is indicated when the lesion is large enough to be unsightly or when it produces symptoms caused by pressure exerted on surrounding structures or when imaging features suggest a malignancy. A tumour relapse is very rarely seen and it usually occurs when unclear resection margins are left.
Bony anomalies or radiographic abnormalities respond well to surgical interventions, with removal of the lesions. Physical therapy after surgery begins with passive motion, followed by active motion and then, strengthening exercises. Use of scapulothoracic arthroscopy is well documented for bursectomy in the treatment of a snapping scapula and in resection of the superomedial angle of the scapula.
Although it is rare, an osteochondroma of the scapula should always be sought as a possible cause of static winging of the scapula and a surgical treatment should be offered, because of possibility of occurrence of a malignant transformation later. Severe winging is a contraindication to surgical resection of the superomedial scapula.
Conclusion
Osteochondroma of the ventral surface of scapula usually presents with a wide variety of symptoms. This case report describes a rare presentation of an osteochondroma which led to pseudowinging of the scapula and it highlights the importance of including this kind of pathology in the differential diagnosis for any presentation of pseoduwinging of scapula. Presentation of the tumour at the superomedial angle of the ventral surface in an adult female is unusual, with regards to both the site and age group. The patient was free of most of the common symptoms which are encountered in such presentations. So, we infer that all cases may not have these symptoms and that rarely, if the tumour is large enough and in proximity to the ribs, it can cause unusual pressure effects like erosion, as it was seen in this case. Three main indications which we saw for undertaking surgery in this case were cosmetic concern, large bursa and pressure effects on ribs. Patient showed significant relief of symptoms following surgical resection and there was no recurrence.
[1]. Saglik Y, Altay M, Unai VS, Basari K, Yildiz Y, Manifestaitons and management of osteochondroma: a retrospective analysis of 382 aptientsActa Orthop Belg 2006 72:748-755. [Google Scholar]
[2]. Porter DE, Simpson AHRW, The neoplastic pathogenesis of solitary and multiple osteochondromasJ Pathol 1999 188:119-125. [Google Scholar]
[3]. Khurana J, Adbul-Karim F, Bovee JVMG, OsteochondromaIn: World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of Soft Tissue and Bone 2002 Lyon, FranceIARC:234-236.Fletcher CDM, Unni KK and Mertens F (eds.) [Google Scholar]
[4]. Bovee JVMG, Hogendoom PCW, Multiple OsteochondromasIn World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of Soft Tissue and Bone 2002 Lyon, FranceIARC:360-362.Fletcher CDM, Unni KK and Mertens F (eds.) [Google Scholar]
[5]. Canella P, Gardin F, Borriani S, Exotosis: Development, evolution and relationship to malignant degenerationItal J Orthop Traumatol 1981 7:293-298. [Google Scholar]
[6]. Kitsoulis Panagiotis Osteochondromas: review of the clinical, radiological and pathological features. in vivo 22.5 2008 :633-46. [Google Scholar]