Giant Cervical Spine Osteochondroma in an Adolescent Female
N. Huda1, M. Julfiqar2, Ajay Pant3, Tariq Jameel4
1 Associate Professor, Department of Orthopaedics, Teerthanker Mahaveer Medical College and Research Centre, T.M.U. Moradabad U.P, India.
2 Assistant Professor, Department of Orthopaedics, Teerthanker Mahaveer Medical College and Research Centre, T.M.U. Moradabad U.P, India.
3 Professor and Head, Department of Orthopaedics, Teerthanker Mahaveer Mahaveer Medicl College and Research Centre, T.M.U. Moradabad U.P, India.
4 Assistant Professor, Department of Orthopaedics, Teerthanker Mahaveer Medical College and Research Centre, T.M.U. Moradabad U.P, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. M. Julfiqar, Assistant Professor, Department of Orthopaedics, Teerthanker Mahaveer Medical College and Research Centre, T.M.U. Moradabad U.P, India.
Phone: +91-8979949300,
E-mail: drzulfiqar1983@rediffmail.com
Osteochondroma or osteocartolaginous exostosis is by far the most common benign bone tumour, which accounts for 35% to 50% of benign bone neoplasms and 10% to 15% of all primary bone tumours. Osteochondroma represents a developmental enchondromatous hyperplasia which leads to formation of cartilage capped bony protrusions on bony surfaces. We present a case report of a 14-year- old female, who presented to us with a hard, gradually progressing, large painless swelling, over the left side of her neck. Swelling was nontender, extending from dorsal to ventral aspect, measuring 6 x 8 cm. Therefore, we are interested in introducing our case to medical fraternity, in which a giant lower cervical spine osteochondroma was seen in an adolescent female patient.
Cervical spine, Osteochondroma, Adolescent female, Surgical excision
Case Report
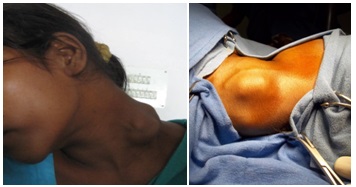
A 14-year-old female presented to the outdoor department at our institute, with a large painless and, gradually progressing hard swelling over the left side of her neck. The swelling increased upto the present status within four years. Local examination revealed a bony hard, nontender, globular mass measuring 6 x 8 cm and extending from dorsal to ventral aspect of the neck on the left side. The mass seems to be continuous with lower cervical vertebra, C5 and C6 [Table/Fig-1]. There was no history of trauma, fever, weight loss or loss of appetite. Movements of the neck, particularly the rotation towards left, were restricted due to mass effect of exostosis. There was no associated soft tissue swelling or oedema. There was no neurological deficit in the patient. Patient was hospitalized for further management.
Showing a hard large globular swelling on the left lateral aspect of the neck
Diagnostic work-up
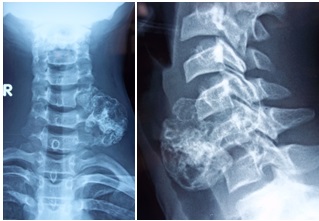
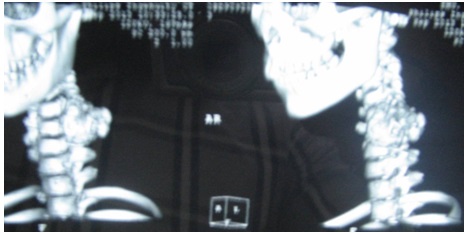
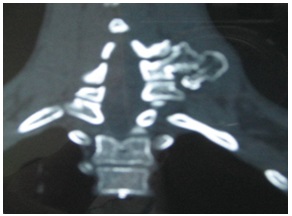
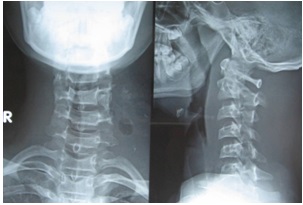
A plain radiograph of the cervical spine (AP and lateral view) showed an irregular calcified mass (exostosis) in left paravertebral region, at C5-C7 level [Table/Fig-2]. Computerized tomography scan of the cervical spine with 3D reconstruction was done, which showed a well defined, pedunculated fungating mass with a calcified cartilage cap, measuring about 4.3 x 3.7 x 2.3 cm,arising from the left transverse process of C6 Cervical vertebra [Table/Fig-3]. CT scan of the cervical spine also showed corticomedullary continuity with the C6 vertebra [Table/Fig-4]. There was no canal extension of the exostotic growth.
X-rays of the cervical spine AP and lateral views showing exostosis arising from left paravertebral region at C5-C7 level
CT scan of cervical spine showing a well delineated, pedunculated fungating mass with calcified cartilage cap arising from the left transverse process of the C6 vertebra
Axial CT scan cut showing corticomedullary continuity between exostosis and the parent vertebra from which it is arising
Treatment
We planned total excision of the exostosis and the excised specimen was subjected to a histopathological examination. Patient was operated under general anaesthesia and the exostotic growth was approached by a transverse skin incision which was made directly over the growth [Table/Fig-5]. After operation, the neck movements of the patient began to improve. A check X-ray of the cervical spine, including AP and lateral views, was done in the postoperative period, which showed complete removal of the exostosis [Table/Fig-6]. Histopathological examination of the excised specimen confirmed it to be an osteochondroma. At the time of last follow-up examination one year after the surgery, no clinical or radiological sign of recurrence of the tumour growth in the cervical spine was seen.
Exostotic growth was exposed throgh a transverse skin incision directly over the growth

Postoperative x-rays of the cervical spine showing complete removal of the exostosis from the vertebra
Discussion
Osteochondromas occur more frequently in men with a M:F ratio of 2.5:1, and patients are generally under the age of 20 years [1,2,3]. Among the spinal exostosis, the osteochondromas usually localize in the upper cervical spine. However, our case was a bit different in both its gender occurrence as well as its location in the lower cervical spine. The noted complications of cervical osteochondromas include, compressions of vertebral artery, subclavian artery and the common carotid artery [1,4,5] as well as other neurological complications. In our case, there was no neurological deficit. However, there was a limitation in neck movements caused by the effect which arose from the large mass of the osteochondroma. Computerized Tomography scan is helpful in differentiating the cartilaginous and bone components of the tumour, and also its relationship with the surrounding peripheral structures, including the neural tissues can be also determined [1,6,7] by CT scan. Magnetic resonance imaging (MRI) is also helpful for the demonstration of spinal cord or nerve root compressions [7]. Exostoses are thought to arise as a result of aberrations which occur in the normal epiphyseal growth. An intralesional excision of a osteochondroma is associated with a high recurrence rate. However, once a osteochondroma is removed along with its cartilage cap, its recurrence can be prevented.
Conclusion
Cervical spine osteochondromas can be successfully managed by complete surgical excisions, including removal of their cartilage caps, to prevent their recurrences.
[1]. Arasil E, Erdem A, Yuceer N, Osteochondroma of the upper cervical spine: A case reportSpine 1996 21:516-8. [Google Scholar]
[2]. Ratliff J, Voorhies R, Osteochondroma of the C5 lamina with cord compression: case report and review of literatureSpine 2000 25:1293-5. [Google Scholar]
[3]. Albrecht S, Crutchfield JS, Se Gall GK, On spinal osteochondromasJournal of Neurosurgery 1992 77(2):247-52. [Google Scholar]
[4]. Resnick D, Kyriakos M, Gerenway GD, Bone and joint imaging 1989 PhiladelphiaSaunders:1107-81. [Google Scholar]
[5]. Wortler K, Linder N, Gosheger G, Brinkschmidt C, Heindel W, Osteochondroma: MR imaging of tumor related complicationsEur Radiol 2000 10:832-40. [Google Scholar]
[6]. Cook RS, Cumming WJ, Cowie RA, Osteochondroma of the cervical spine: case report and review of literatureBr J Neuosurg 1994 8:359-63. [Google Scholar]
[7]. Cirak B, Karabulut N, Plaoglu S, Cervical Osteochondroma as a cause of spinal cord compression in a patient with hereditary multiple Exostosis: Computed tomography and magnetic resonance imaging findingsAustralas Radiol 2002 46:309-11. [Google Scholar]