Variations in Innervation of Muscles in Anterior Compartment of Arm – A Cadaveric Study
Parminder Kaur1, Rajesh Kumar2, Anjali Jain3
1 Associate Professor, Department of Anatomy, CMC & H, Ludhiana, India.
2 Associate Professor, Department of Immunohaematology and Blood Transfusion, DMC & H, Ludhiana, India.
3 Professor, Department of Anatomy, CMC & H, Ludhiana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Parminder Kaur, Associate Professor, Department of Anatomy, Christian Medical College & Hospital, Ludhiana – 141008, Punjab, India.
Phone: +919781815672,
E-mail: gskairon@yahoo.co.in
Aims and Objective: Study was undertaken to observe the variation in the innervation of muscles in the front of arm. The results were compiled. Embryological basis and clinical applications of encountered variations were tried to explain with the help of available literature.
Material and Methods: Thirty upper limbs from fifteen cadavers were dissected to observe the contents of front of arm. Musculocutaneous nerve, median nerve and innervation of the muscles of front of arm were observed.
Results: Variations were observed in 13% of cases. Commonly seen variation was the absence of musculocutaneous nerve and innervation of muscles of front of arm by branches of median nerve. This variation was seen bilaterally in 3.3% of cases and unilaterally in 6.6% cases. Bilateral presence of this variation in one out of fifteen cadavers is rare finding. Variation is more common on right side as compared to the left side.
Conclusion: Bilateral absence of musculocutaneous nerve and innervation of muscles of front of arm from the branches of median nerve is a rare variation. Knowledge of such anatomical variations is of interest to the anatomist and clinician alike. Variations assume significance during surgical exploration of the axilla and can even fail nerve block of infraclavicular part of brachial plexus. Surgeons who perform procedures involving neoplasm or repairing trauma need to be aware of these variations.
Musculocutaneous nerve, Median nerve, Innervation, Muscles
Introduction
Muscles in anterior compartment of arm i.e. coracobrachialis both heads of biceps and brachialis are supplied by musculocutaneous nerve. Small lateral part of brachialis also receives branches of radial nerve. Musculocutaneous nerve is the nerve of anterior compartment of arm. It arises from lateral cord (C5,6,7) opposite the lower border of pectoralis minor. Median nerve has no muscular branch for the flexor muscles of front of arm [1].
Knowledge of normal anatomy as well as variations is important particularly to the surgeons for carrying out surgical procedures [2].
Variations of peripheral nerves are important to orthopedic surgeon, neuron physician, physiotherapists and radiologists. Such comprehension is useful in nerve grafting and neuro physiological evaluation for diagnosing peripheral neuropathies [3].
Materials and Methods
Thirty upper limbs from fifteen formalin fixed adult human cadavers were dissected to see the innervation of muscles of anterior compartment of arm. The steps of dissection were followed from Cunningham’s Manual of Practical Anatomy Vol. I [4]. The skin from pectoral region, axilla & arm was incised and superficial fascia was reflected. Deep fascia was separated to see the contents of arm. The muscles were observed for their innervation. The variations were noted and photographs were taken.
Observation
Among the 30 limbs which were dissected from 15 preserved cadavers standard textbook pattern was observed in 86.7% limbs whereas in 13.3% of the limbs variation was seen as follows [Table/Fig-1].
Absence of musculocutaneous nerve right/left limbs
| Right | Left | Total |
|---|
| Total Number of limbs | 15 | 15 | 30 |
| Absent Musculocutaneous Nerve | 03 | 01 | 04 |
Musculocutaneous nerve was seen to be absent bilaterally in one cadaver and flexor muscles of arm were innervated by branches from median nerve. Same variation was seen in two other limbs belonging to right side whereas left limbs in those cadavers had typical innervation.
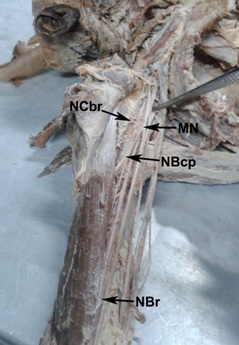
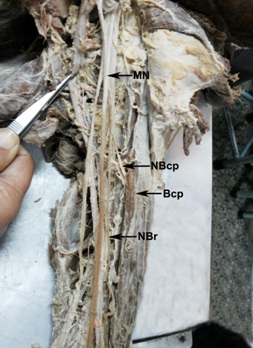
Bilateral variation was seen in one cadaver. In this musculocutaneous nerve was absent whereas median nerve had small lateral root and normal medial root in relation to the third part of the axillary artery. A small branch was seen coming from lateral root to supply coracobrachialis, later it joined median nerve after a few centimeters only. In this case rest of the flexor muscles (brachialis and biceps brachii) were innervated by median nerve [Table/Fig-2,3].
Right Arm: Median nerve supplying muscles of front arm NCbr: Nerve to Coracobrachialis, MN: Median Nerve, NBcp: Nerve to biceps brachii NBr: Nerve to brachialis
Left Arm: Absent Musculocutaneous nerve, Median nerve innervating muscle of front of arm. MN: Median Nerve, NBcp: Nerve to biceps brachii, Bcp: Biceps, NBr: Nerve to brachialis
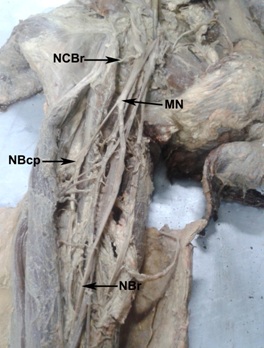
In rest of the two cases also musculocutaneous nerve was absent whereas the formation of median nerve was seen normal after the union of two roots. Nerve to coracobrachialis was given off immediately after the union then it gave branches to biceps and brachialis. Variation was confined unilaterally to right limbs of two cadavers [Table/Fig-4].
Right Arm: Absent Musculocutaneous nerve, Median nerve innervating muscle of front of arm. NCbr: Nerve to Coracobrachialis, MN: Median Nerve, NBcp: Nerve to biceps brachii NBr: Nerve to brachialis
Discussion
Musculocutaneous nerve is the main nerve of flexor muscle of arm that arises from lateral cord of brachial plexus in axilla. Prasada Rao [5] reported 2 cases of absence of musculocutaneous nerve whereas Ihunwo et al., [6] has reported bilaterally absence of musculocutaneous nerve. In the present study we have also observed musculocutaneous nerve absent bilaterally in one cadaver whereas unilateral absence was seen in 2 right limbs. Complete absence of musculocutaneous nerve and innervation of flexor muscles by median nerve is uncommon variation of brachial plexus [7–9] [Table/Fig-5].
Comparison of reported cases of absence of musculocutaneous with previous authors
| Authors | Year | No. of reported cases |
|---|
| Ihunwo et al. | 1997 | 1 |
| Prasada Rao | 2001 | 2 |
| Present study | 2014 | 3 |
Variants of branching pattern of musculocutaneous nerve and median nerve has been described by many authors [3]. Le minor [10] has classified the variations into five types.
Type I: No communication between median nerve and musculocutaneous nerve.
Type II: The fibres of medial root of median nerve pass through the musculocutaneous nerve and join the median nerve in the middle of the arm.
Type III: The fibres of lateral root of median nerve pass along the musculocutaneous nerve and after some distance leave it to form the lateral root of median nerve.
Type IV: The musculocutaceous fibres join the lateral root of the median nerve and after some distance musculocutaneous nerve arises from the median nerve.
Type V: The musculocutaneous nerve is absent and the entire fibres of musclocutaneous nerve branch out directly from the median nerve. Present study indicate the presence of [10] type V variation.
As the roots of musculocutaneous nerve and lateral root of median nerve are same, in the absence of musculocutaneous nerve the muscles of front of arm get motor innervations by median nerve [11].
Understanding the embryologic development of the brachial plexus is important in explaining such anatomic variations. The human upper limb bud appears at about 26-27 days of embryonic life and axons of motor neurons of the spinal cord enter the limb buds during the fifth week. Formation of the brachial plexus is evident at about 34-35 days as a single radicular cone in the upper limb. Between 38th and 40th days, the major branches of the brachial plexus such as median, radial and ulnar nerves are visualized which are seen to enter the hand plate. The musculocutaneous nerve arises as an offshoot of median nerve. At about 46th -48th days, the upper limb nerve attain definitive adult pattern [12]. The need of brachial plexus arises for ease of distribution from several spinal segments and one spinal segment can be distributed to several peripheral nerves [13]. Plexus is a complex of branching, reunion and reseparation of nerve fibres that usually happens near the root of limbs, which is axilla for the upper limb. The complex network is sometimes extending in to the arm. The roots of musculocutaneous nerve and lateral root median nerve are same, i.e. C5, C6 and C7. In the absence of musculocutaneous nerve the same root travel through the lateral root median nerve and are distributed in the muscles of the front of arm via median nerve [11].
The upper limb buds lie opposite to the lower five cervical and upper two thoracic segments. As soon as buds form, the ventral primary rami of the spinal nerves penetrate into the mesenchyme of limb bud and establish intimate contact with differentiating mesodermal condensations. The early contact between nerve and muscle cell is a prerequisite for their complete functional differentiation [14,15]. The variation could arise from circulatory factors at the time of fusion of brachial plexus cord. In human, the forelimb muscles develop from the mesenchyme of the para-axial mesoderm during fifth week of embryonic life [15]. The axon of spinal nerve grows distally to reach the limb bud mesenchyme. The peripheral process of the motor and sensory neurons grows in the mesenchyme in different directions. Once formed any developmental differences would obviously persist postnatally [14]. As the guidance of the developing axons is regulated by expression of chemo-attractants and chemo-repellants in a highly coordinated site specific fashion, any alteration in signaling between mesenchymal cells and neuronal growth cones can lead to significant variations [16].
Conclusion
Bilateral absence of musculocutaneous nerve and innervation of muscles of front of arm from the branches of median nerve is a rare variation. Knowledge of such anatomical variations is of interest to the anatomist and clinician alike. Variations assume significance during surgical exploration of the axilla and can even fail nerve block of infraclavicular part of brachial plexus. Surgeons who perform procedures involving neoplasm or repairing trauma need to be aware of these variations. Meticulous knowledge of possible variations of musculocutaneous nerve and median nerve may endow us with valuable help in the management of traumatology of the shoulder joint, specifically constructive shoulder arthroplasty and shoulder dislocations as well as in circumventing iatrogenic damage during repair operations of these regions [3]. These variations may also help in interpretation of nervous compression having unexplained clinical symptoms [17].
[1]. Standring S, Gray’s Anatomy 2008 40th editionPhiladelphiaElsevier Churchill Livingstone:821 [Google Scholar]
[2]. Satyanarayana N, Vishwakarma N, Kumar GP, Guha R, Dattal AK, Sunitha P, Rare variations in the formation of median nerve – embryological basis and clinical significanceNepal Med Coll J 2009 11(4):287-90. [Google Scholar]
[3]. Yogesh AS, Joshi M, Chimurkar VK, Marathe RR, Unilateral variant motor innervations of flexure muscle of armJ Neruosci Rural Pract 2010 1(1):51-3. [Google Scholar]
[4]. Romanes GJ, Cunningham’s Manual of Practical Anatomy 1986 15th editionLondonOxford University Press [Google Scholar]
[5]. Rao Prasada PVV, Chaudhary SC, Absence of the musculocutaneous nerve: Two case reportsClin Anat 2001 14:31-5. [Google Scholar]
[6]. Ihunwo AO, Osinde SP, Mukhtar AU, Distribution of median nerve to the muscles of the anterior compartment of the armCent Afr J Med 1997 43:359-60. [Google Scholar]
[7]. William PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, Nervous systemIn: Gray’s Anatomy 1995 38th editionEdinburgh, LondonChurchill Livingstone:1267-72. [Google Scholar]
[8]. McMinn RMH, Last’s Anatomy: Regional and Applied 1994 9th editionLondonChurchill Livingstone:78-80. [Google Scholar]
[9]. Moore KL, Clinically oriented anatomy 1992 3rd editionBaltimoreWilliams and Wilkins:513-16. [Google Scholar]
[10]. Le Minor J.M., A rare variant of the median and musculocutaneous nerve in manArchieves Anatomy Histology Embryology 1990 73:33-42. [Google Scholar]
[11]. Sontakke BR, Tarnekar AM, Waghmare JE, Ingole IV, An unusual case of asymmetrical formation and distribution of median nerveInternational Journal of Anatomical Variations 2011 4:57-60. [Google Scholar]
[12]. Moore KL, Parsaud TVN, The Developing HumanClinically Oriented Embryology 2004 7th editionPhiladelphiaSaunders:408-23. [Google Scholar]
[13]. Sinnatamby CS, Last’s Anatomy. Regional and Applied 2008 11th editionNew YorkChurchill Livingstone Elsevier:1-34. [Google Scholar]
[14]. Brown MC, Hopkins WG, Keynes RJ, Essentials of neural development 1991 CambridgeCambridge University Press:46-66. [Google Scholar]
[15]. Larsen WJ, Human Embryology 1997 2nd editionEdinburgChurchill Livingstone:311-39. [Google Scholar]
[16]. Samnes DH, Reh TA, Harris WA, Development of nervous system 2000 New YorkAcademic Press:27-28. [Google Scholar]
[17]. Budhiraja V, Rastogi R, Asthana AK, Anatomical variations of median nerve formation: Embryological and Clinical correlationJ Morphol Sci 2011 28(4):283-6. [Google Scholar]