Primary Failure of Eruption- A Case Report with Cone Beam Computerized Tomographic Imaging
U. Aruna1, P.R. Annamalai2, Sanjna Nayar3, S. Bhuminathan4
1 Reader, Department of Prosthodontics, Sree Balaji Dental College and Hospital, Chennai, India.
2 Reader, Department of Orthodontics, Chettinad Dental College and Hospital, Chennai, India.
3 Professor & HOD, Department of Prosthodontics, Sree Balaji Dental College and Hospital, Chennai, India.
4 Professor, Department of Prosthodontics, Sree Balaji Dental College and Hospital, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. U. Aruna, Reader, Department of Prosthodontics, Sree Balaji Dental College and Hospital, Pallikaranai, Chennai- 600100, India.
Phone: +91 9444534018,
E-mail: arunayou@gmail.com.
Tooth eruption is an intricate and complex process which can fail to occur due to several reasons. Failure of tooth eruption in the absence of any systemic condition or any obstruction in the eruptive pathway can be attributed to lack of inherent eruptive potential of the tooth, termed as Primary Failure of Eruption (PFE). This is a rare condition and usually has a genetic etiology. Here we report a rare case in which there is Primary Failure of Eruption in the mandibular right quadrant. There is also mechanical failure of eruption of maxillary right canine and supernumerary teeth palatal to the maxillary central incisors. This association of supernumerary teeth and mechanical failure of eruption along with primary failure of eruption has not been reported so far. Proper diagnosis is very important in cases of Primary Failure of Eruption. There are several diagnostic criteria to identify these cases. Since these cases do not respond to orthodontic force, early diagnosis is of essential importance.
Primary failure of eruption, CBCT, Path of eruption
Case Report
An 18-year-old male patient was referred for orthodontic opinion because of multiple unerupted posterior teeth. The patient’s primary complaint however was unesthetic appearance because of overlapping of upper front teeth. His medical history was unremarkable and he did not have a familial history of non-eruption of posterior teeth. No apparent physical abnormality was present.
Intra-oral examination revealed proclination of anterior teeth and overlapping of maxillary central incisors. Third molars in all the four quadrants had not erupted and the right mandibular molars had not erupted, leading to a posterior open bite in the right side. Two supernumerary teeth were present palatal to the maxillary incisors. The upper right deciduous canine was retained and its permanent successor was missing. A bulge was seen buccally in the canine region suggestive of the permanent canine [Table/Fig-1,2a,2b,3,4–5]. A lateral Cephalogram and a Orthopantomogram was advised initially.
Intra- oral Photographs of the patient Frontal View (a) Frontal View (b) Right Lateral View (c) Left lateral View




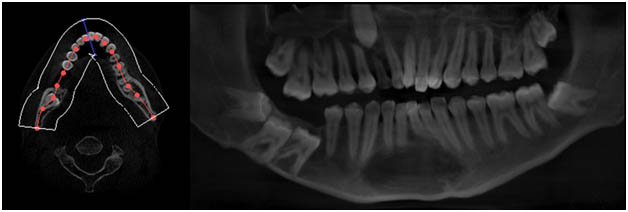
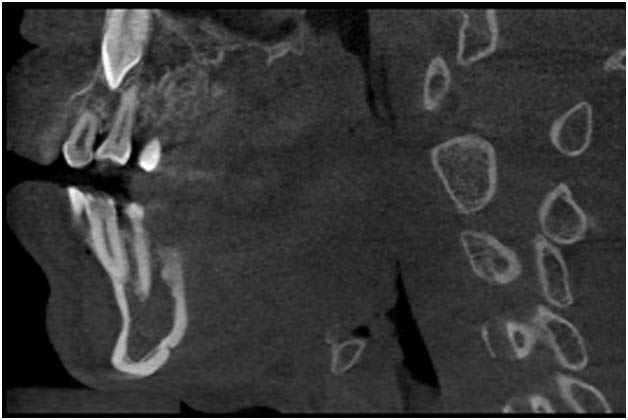
Figure showing root resorption in the distal root of right mandibular first molar.
Radiographic Examination
Orthopantomogram revealed impacted right mandibular first, second and third molars and also the left mandibular third molar. In the maxillary arch both the right and left third molars were impacted. The maxillary right permanent canine was impacted and the corresponding deciduous canine was retained. The supernumerary teeth in the anterior palatal region were not clear, because of overlapping structures. The distal root of the mandibular right first molar was not evenly radiopaque suggestive of root resorption in mandibular right first molar.
Since CBCT has become the standard for three dimensional imaging, where we can have a three dimensional view of the unerupted teeth, their anatomic location and relation to the inferior alveolar canal, chances of ankylosis, and bone resorption which clears a path for eruption, a Cone Beam Computerised Tomography (CBCT) was taken for the patient.
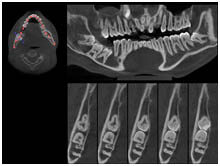
The presence of retained deciduous canine, impacted permanent canine, supernumerary teeth in the maxillary arch palatal to the central incisors, unerupted right mandibular molars which were near the lower border of the mandible were further confirmed through the CBCT images [Table/Fig-6]. CBCT also clearly showed root resorption in the distal root of right mandibular first molar [Table/Fig-7], breach of mandibular canal in relation to right mandibular first, second and third molars, and presence of resorptive area above the mandibular right first permanent molar [Table/Fig-8]. The presence of permanent canine directly above the retained deciduous canine was also clearly seen.
Image showing mandibular canal in relation to Right posterior teeth.
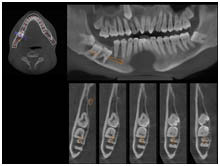
Image showing resorptive area above the mandibular right first permanent molar.
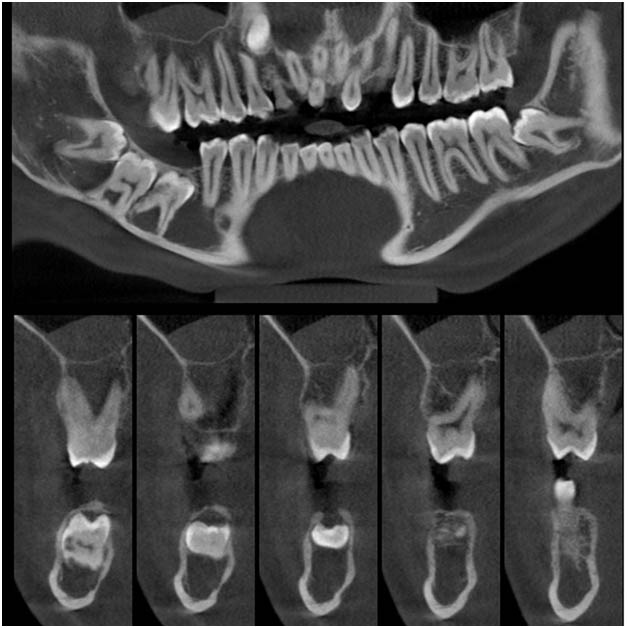
Image showing the permanent canine directly above the retained deciduous canine
The findings of unilaterally unerupted mandibular molars in the right side with no asasociated syndromes and no mechanical obstruction were suggestive of Primary Failure of Eruption in this patient.
Discussion
The patient was diagnosed to have Primary Failure of Eruption (PFE) in the right mandibular posterior region. The following characteristics present in this patient were suggestive of PFE,
Unilateral involvement.
Posterior tooth affected.
All the teeth distal to the first molar were affected.
No associated syndromes.
The second and third molars were at a higher occlusal level than the first molar - characteristic feature of Type II PFE.
The associated failure of eruption of permanent canine cannot be considered as a case of primary failure of eruption. The presence of mechanical impediment, that is retained deciduous canine and the non involvement of teeth distal to it were suggestive of a mechanical failure of eruption.
The genetic analysis for the PTH1R gene could have additionally aided in the diagnosis of Primary Failure of Eruption [1-3].
This patient did not have a familial history of occurrence of primary failure of eruption. Frazier Bowers et al have found that there appears to be no obvious difference in the types of PFE expressed by family members vs the isolated cases [4]. Profitt & Vig have also shown that their patients did not have similarly affected close relatives [5]. This could be because of the variable expressivity of the gene [6]. Though recent literature is suggestive more of a familial tendency for PFE, it does occur as isolated cases as in our case.
Genetic studies have suggested that PTH1R is an ideal candidate gene for analysis of an eruption failure phenomenon. Further studies should analyse the specific role of PTH1R in the understanding of eruption failure and whether additional genes are involved in familial eruption failure. The presence of supernumerary teeth is an additional finding, which has not been reported so far in the previous literature. This could be suggestive of a related genetic defect other than PTH1R, or could be a mere coincidence. Though it is becoming clearer that PTH1R gene is affected in these patients, the reason why it is localised, affecting usually unilaterally and only posteriors is not clear. The temporal and spatial specificity of the gene expression is still not clearly understood.[6] The presence of supernumerary teeth in our case suggests PFE could be a part of wider spectrum of a genetic problem. It is also possible that PTH1R, though is primarily involved in the regulation of tooth eruption, may also have a role in tooth bud formation and morphogenesis.
Treatment of patients with Primary Failure of Eruption:
An interdisciplinary approach is required in this condition. The various treatment options considered earlier include [5].
Orthodontic extrusion of un-erupted teeth.
Surgical repositioning of the affected dento alveolar segment with the teeth.
Prosthodontic management for the unerupted teeth and overlay crowns in mild case.
Orthodontic extrusion of unerupted teeth is not considered as the treatment of choice anymore as they were not successful in erupting the teeth. Application of orthodontic force leads to ankylosis of the teeth, and it also worsens the open bite.
Orthodontic force is helpful only when the eruptive mechanism is intact, i.e., helpful in erupting the teeth in Mechanical Failure of Eruption (MFE), but not in Primary Failure of Eruption (PFE), where the mechanism is itself at fault. The fact that orthodontic force is not able to move the teeth, suggests that the fault in the eruptive mechanism is permanent and not a temporary one, seen during root formation. The defect in the eruptive process is irreversible and permanent. So, orthodontic treatment is no more a treatment option for PFE cases, rather when the diagnosis is confirmative of PFE it is better not to subject the teeth to orthodontic force [2,5].
The problem in treating patients with primary failure of eruption lies in the disruption of eruption potential of tooth. Multidisciplinary treatment options can be discussed for patients with severe posterior open-bite.
Surgical repositioning of the teeth along with the alveolar segment is a viable treatment. Care should be taken to avoid trauma to the inferior alveolar nerve, as most of the affected teeth are nearer to the lower border of the mandible [4].
Conclusion
Prosthodontic rehabilitation is most often the only treatment available for these patients. When the severity of the condition is mild and the crowns are seen in the oral cavity overlay crowns or overlay removable partial denture can be given. Definitive restoration should not be placed before completion of vertical growth [7,8]. It can be concluded by quoting Wise et al., [9] that, Tooth eruption appears to be a programmed, localized event whereby a given tooth erupts at its appointed time. The molecules that initiate eruption, their localization, and their regulation of the cellular events of eruption—all must fit within the context that each tooth erupts independently.
[1]. Decker E, Stellzig-Eisenhauer A, Fiebig BS, Rau C, Kress W, Saar K, PTHR1 loss-of-function mutations in familial, nonsyndromic primary failure of tooth eruptionAm J Hum Genet 2008 83(6):781-6. [Google Scholar]
[2]. Frazier-Bowers SA, Simmons D, Timothy Wright J, Proffit WR, Ackerman JL, Primary eruption failure and PTH1R: The importance of a genetic diagnosis for orthodontic treatment planningAm J Orthod Dentofacial Orthop 2010 137:160.e1-160.e7. [Google Scholar]
[3]. Stellzig-Eisenhauer A, Decker E, Meyer-Marcotty P, Rau C, Fiebig BS, Kress W, Primary Failure of Eruption (PFE) – Clinical and Molecular Genetics AnalysisJ Orofac Orthop 2010 71:6-16. [Google Scholar]
[4]. Frazier-Bowers SA, Koehler KE, Ackerman JL, Proffit WR, Primary failure of eruption: further characterization of a rare eruption disorderAm J Orthod Dentofacial Orthop 2007 131(5):578.e1-11. [Google Scholar]
[5]. Proffit WR, Vig KWL, Primary failure of eruption: a possible cause of posterior open biteAm J Orthod 1981 80:173-90. [Google Scholar]
[6]. Frazier-Bowers SA, Puranik CP, Mahaney MC, The etiology of eruption disorders – further evidence of a ‘genetic paradigm’Semin Orthod 2010 16(3):180-5. [Google Scholar]
[7]. Siegel SC, O’Connell A, Oral rehabilitation of a child with primary failure of eruptionJ Prosthod 1999 8:201-7. [Google Scholar]
[8]. Castillo R.D, LaMar Jr F, Ercoli C, Maxillary and mandibular overlay removable partial dentures for the treatment of posterior open-occlusal relationship: A Clinical ReportJ Prosthet Dent 2002 87:587-92. [Google Scholar]
[9]. Wise GE, Frazier-Bowers S, D’Souza RN, Cellular, molecular, and genetic determinants of tooth eruptionCrit Rev Oral Biol Med 2002 13:323-34. [Google Scholar]