Primary fibrosarcoma of the breast is a very rare tumor. However, amongst the Primary Breast Sarcoma (PBS), it is the most common subtype. We present a case of 28-year-old male with lump in right breast of 7 year duration. The unilateral multinodular mass showed well circumscribed but unencapsulated tumor composed of interlacing fascicles of spindle shaped cells with minimal atypia. Immunohistochemistry revealed positivity for vimentin in the tumor cells. Differential diagnoses and review of literature is discussed.
Male, Breast, Fibrosarcoma
Case Report
Breast sarcomas are rare tumors with an incidence of <1% of all breast malignancy [1]. Primary breast sarcoma (PBS) is defined as malignancy originating from mesenchymal tissue of the breast and does not include those arising from skin, muscle, and adjacent bones. They are similar to soft tissue sarcomas elsewhere in the body. These include fibrosarcoma, liposarcoma, alveolar soft part sarcoma, clear cell sarcoma, leiomyosarcoma, rhabdomyosarcoma, angiosarcoma, malignant fibrous histiosarcoma. Although, the most common breast sarcoma is cystosarcoma phyllodes, but it is not a true sarcoma (fibroepithelial lesion by definition) and is excluded from most recent studies on PBS. Primary fibrosarcoma of the breast is a very rare tumor described in literature, accounting for 16% of all soft tissue sarcomas of the breast [2].
A 28-year-old male presented with lump in right breast of 7 year duration. It was increasing in size since 2 months. There was no previous history of trauma to the chest wall, radiation exposure or family history of breast cancer. Also, there was no history of nipple discharge. On examination, it was unilateral multinodular mass measuring 10 × 8 cm in size. It was free from the skin surface and underlying tissue. Nipple and areola showed no changes. There was a 1×1 cm right axillary lymph node. Fine needle aspiration from the breast mass was suggestive of a spindle cell sarcoma with a possibility of malignant phyllodes tumour. Radical mastectomy with right axillary dissection was done.
Macroscopically, two nodules protruding from the surface measuring 4.5 and 2.5 cm in diameter were seen in upper outer and lower outer quadrant respectively. The overlying skin was stretched but intact and not fixed to the nodules [Table/Fig-1].
Slice of serially sectioned mastectomy specimen showing a large nodule protruding from the surface

On serial sections another well circumscribed nodule was noted in the retro-areolar region measuring 4 cm in diameter. The cut surfaces of the nodules was firm grey white homogenous. Ten axillary lymph nodes measuring in size from 0.3 to 1 cm were also received in a separate container.
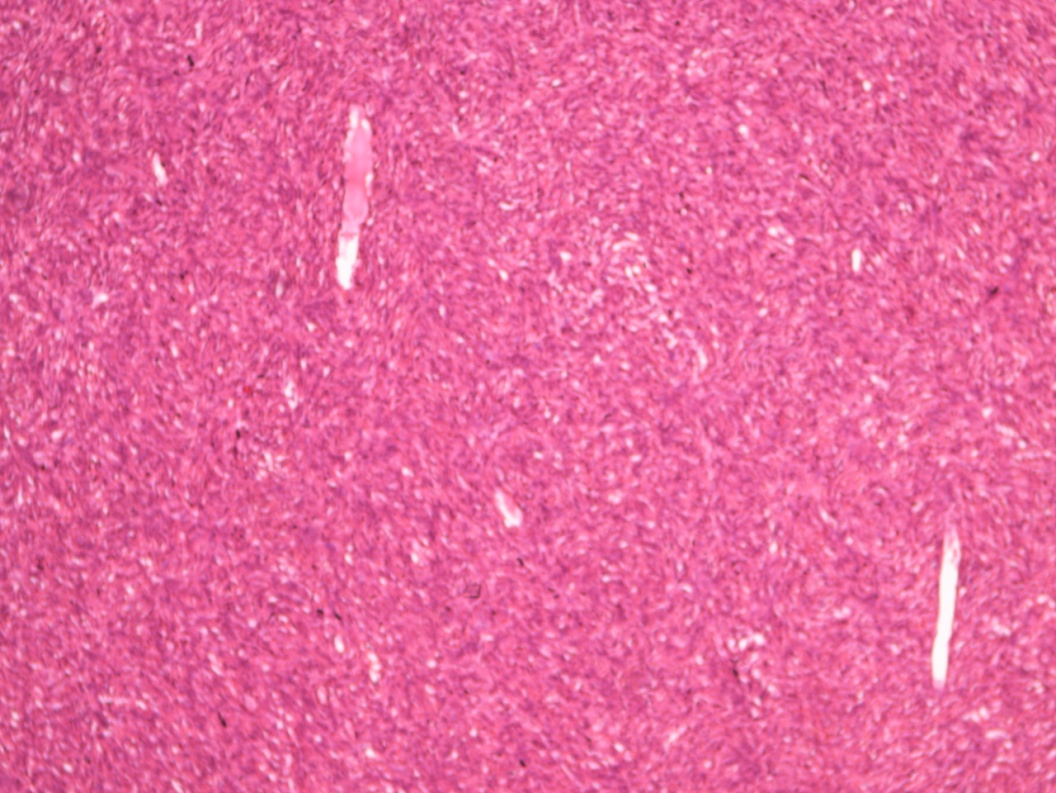
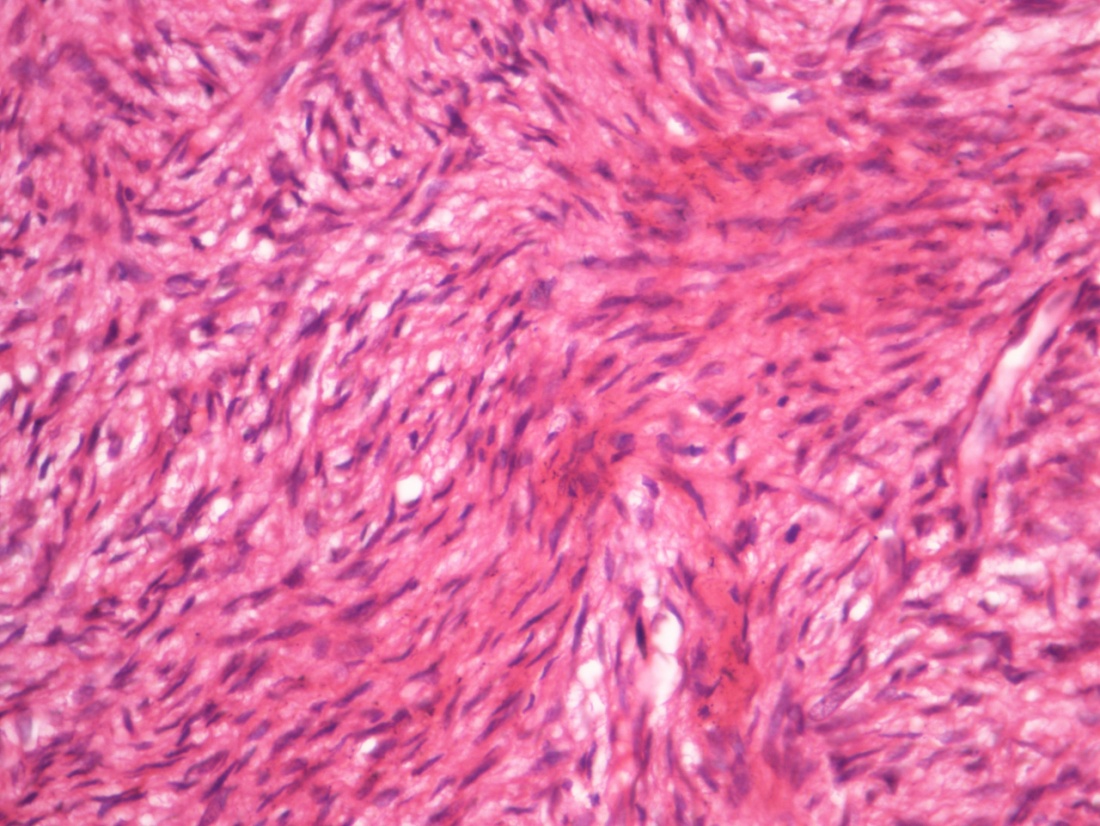
Microscopic examination of the hematoxylin and eosin (H&E) stained sections from all the nodules showed a well circumscribed but unencapsulated tumor composed of interlacing fascicles of spindle shaped cells with prominent herring bone pattern [Table/Fig-2a]. The tumor cells had scant cytoplasm and elongated nucleus with minimal atypia. Small foci of myxoid change were also noted. Mitotic activity was 1/10 HPF [Table/Fig- 2b]. The tumor had a pushing margin with normal breast parenchyma seen at the periphery of the tumor. No necrosis or heterologous elements were seen. Sections through the skin including the nipple and areola showed presence of tumor in subcutaneous tissue only with thinning of overlying epidermis. Underlying muscle was also not involved by the tumor. All lymph nodes were reactive. Since epithelial component was not appreciated in the sections from the tumor even after extensive sampling, cystosarcoma phyllodes with stromal overgrowth was excluded.
Interlacing fascicles of spindle shaped cells (H&E:100X)
Spindle cells show elongated nuclei with minimal atypia (H&E: 400X)
Immunohistochemistry (IHC) revealed positivity for vimentin in the tumor cells. It was negative for cytokeratin, EMA, desmin, S-100, CD-10 and CD-34, HMB-45, ER and PR; thus ruling out epithelial, muscular, neural differentiation of the tumor.
A diagnosis of Well-differentiated Multicentric Primary Fibrosarcoma of the breast was rendered (Grade I according to French Federation of Cancer Centers Sarcoma Group grading system) [3].
Discussion
Pure sarcomas of the breast are rarely described and review of literature revealed less than 1% of all the breast malignancies comprised of soft tissue sarcomas. C. Adem et al have quoted an incidence of 0.0006% [4]. Sammy Al-Benna reviewed English literature and found that 98.5% of breast sarcoma occurred in women and 1.5% in men [5].
Male breast sarcomas comprise <1% of all breast cancers [1]. 24% of the 25 cases of breast sarcomas were fibrosarcoma in series studied by C Adem et al., [4]. Pollard et al., found incidence of fibrosarcoma to be 16% amongst the 25 cases studied [2]. Twenty-two out of the 32 cases of breast sarcomas turned out to be fibrosarcoma in series described by Norris et al., [6]. Male breast fibrosarcoma have been described rarely in these case series. Callery et al., reported single male fibrosarcoma out of a total of 9 in their 25 case series as PBS [7]. The incidence of fibrosarcoma reported by them is higher at 32% as they excluded angiosarcomas from PBS in the series. The only study exclusively on male breast malignancies by Kidmas et al., reported an incidence of 7.7% amongst all male breast cancers including infiltrating duct carcinoma and lymphoma [8].
Review of literature from India revealed few case reports [9–11].However, none of them have been reported in male.
Although rare, it is important to accurately diagnose the sarcomas of the breast as its mimic namely, malignant phyllodes or metaplastic carcinoma carry different prognosis and need different therapeutic interventions. Absence of epithelial components on extensive sectioning ruled out the possibility of cystosarcoma phyllodes in this case. The absence of cytokeratin reactivity on IHC ruled out the possibility of metaplastic carcinoma.
Stromal sarcomas of the breast were first described by Berg et al., [12]. Breast sarcomas are usually painless, mobile and large without nipple discharge, or skin involvement. Sarcomas rarely involve axillary lymph nodes. Callery et al., reviewed 25 patients with breast sarcomas, all were negative for regional lymph node metastasis [7]. Pollard et al., found only 7 cases with regional lymph node involvement and one with lymph node metastasis out of the 25 cases they studied [2]. The present case too did not show any lymph node involvement by the tumor.
Age incidence is higher than Invasive Duct Carcinoma breast involving 5th-6th decade [8]. Prognosis of these tumors depends upon the type of margin, degree of cellularity, atypia, and mitotic figures. Less than 5 cm tumors usually have better prognosis [13]. Metastasis from the primary soft tissue sarcoma of the breast can involve lung, peritoneum, retroperitoneal lymph nodes, bone, skin, rib cage, brain, liver, pleura. Mainstay of treatment is surgery with few subgroups opting for adjuvant radiotherapy [9]. Confavreux et al., divided and compared three groups: (1) phyllodes tumour (2) primary breast sarcoma and malignant phyllodes tumour and (3) angiosarcoma and found the 3-year disease-free survival of, 57, 45 and 7% respectively [14]. In the present case, local recurrence or distant metastasis did not occur even after more than one year post surgery.
Fibrosarcoma of the breast is a rare tumor. However, amongst the PBS, it is one of the common ones. The present case is unique in many respects. The tumor presented in a very young male at 28 years of age. (Most PBS reported in women >40 years of age). The tumor was multicentric (very few PBS are multicentric; that too mostly angiosarcoma). In PBS including fibrosarcoma, adequate surgical excision of the tumor, tumor size, and histological grade are the most important prognostic factors. Wide local excision is usually sufficient for low grade tumors <5 cm in size. Mastectomy may be required for larger tumors. Multicentric tumors like the present case may even warrant radical mastectomy. Axillary dissection is usually not required unless palpable lymph nodes are present. Even then, metastasis in lymph nodes is frequently from sarcomatoid carcinoma rather than from PBS. The role of radiation and CT in the treatment of PBS is unclear.
In conclusion, a breast lump that is clinically benign but has undergone recent rapid growth should alert the clinician to the possibility of an underlying sarcoma.
[1]. Pathology & Genetics. Tumours of the breast and female genital organsWorld Health Organization Classification of Tumours 2003 LyonIARC press [Google Scholar]
[2]. Pollard SG, Marks PV, Temple LN, Thompson HH, Breast sarcoma. A clinicopathologic review of 25 casesCancer 1990 66(5):941-4. [Google Scholar]
[3]. Guillou L, Coindre JM, Bonichon F, Nguyen BB, Terrier P, Collin F, Comparative study of the National Cancer Institute and French Federation of Cancer Centers Sarcoma Group grading systems in a population of 410 adult patients with soft tissue sarcomaJ Clin Oncol 1997 15(1):350-62. [Google Scholar]
[4]. Adem C, Reynolds C, Ingle JN, Nascimento AG, Primary breast sarcoma: clinicopathologic series from the Mayo Clinic & review of literatureBr J Cancer 2004 91(2):237-41. [Google Scholar]
[5]. Al-Benna S, Poggemann K, Steinau HU, Steinstraesser L, Diagnosis and management of primary breast sarcomaBreast Cancer Res Treat 2010 122(3):619-26. [Google Scholar]
[6]. Norris HJ, Taylor HB, Sarcomas and related mesenchymal tumors of the breastCancer 1968 22(1):22-8. [Google Scholar]
[7]. Callery CD, Rosen PP, Kinne DW, Sarcoma of breast. A study of 32 patients with reappraisal of classification & therapyAnn Surg 1985 201(4):527-32. [Google Scholar]
[8]. Kidmas AT, Ugwu BT, Manasseh AN, Iya D, Opaluwa AS, Male breast malignancy in Jos University Teaching HospitalWest Afr J Med 2005 24(1):36-40. [Google Scholar]
[9]. Afroz N, Zaheer S, Khan N, Khan MA, Primary fibrosarcoma of breast: a case report and review of literatureIranian Journal of Pathology 2010 5:204-7. [Google Scholar]
[10]. Biswas S, Chakraborty J, Biswas RKR, Rahman QM, Sanyal S, Pal G, Primary breast sarcomas – report of two casesIndian J Pathol Microbiol 2002 45(1):93-7. [Google Scholar]
[11]. Deodhar SD, Khope SS, Kinare SG, Fibrosarcoma of the breast (a case report)J Postgrad Med 1983 29(2):123-4. [Google Scholar]
[12]. Berg JW, Decrosse JJ, Fracchia AA, Farrow J, Stromal sarcomas of the breast. A unified approach to connective tissue sarcomas other than cystosarcoma phyllodesCancer 1962 15:418-24. [Google Scholar]
[13]. Zelek L, Llombart-Cussac A, Terrier P, Pivot X, Guinebretiere JM, Le Pechoux C, Prognostic factors in primary breast sarcomas: A series of patients with long-term follow upJ Clin Oncol 2003 21(13):2583-8. [Google Scholar]
[14]. Confavreux C, Lurkin A, Mitton N, Blondet R, Saba C, Ranchère D, Sarcomas and malignant phyllodes tumours of the breast—a retrospective studyEur J Cancer 2006 42(16):2715-21. [Google Scholar]