Atypical Carcinoids, Malignancy arising from neuroendocrine cells are among the non–Epidermoid cancers of larynx. The present study reports an interesting and rare case of atypical carcinoid of larynx. An 85-year-old male patient presented with a history of dysphagia. On clinical examination, a provisional diagnosis of cyst larynx was made. But during surgery, the Diagnosis had to be reviewed as benign lesion of the larynx. Histopathological diagnosis was atypical carcinoid. The present study discusses the unusual presentation and unusual clinical diagnosis of these neuroendocrine neoplasms of larynx.
Introduction
Non-epidermoid malignancies of Larynx represent an extremely diverse group of diseases, which are known to cause non-specific symptoms, pose complexity in clinical diagnosis, management and uncertain prognosis [1].
There is no universally accepted classification of non-epidermoid carcinoma. Among many other carcinomas SECRETORY and NONSECRETORY neuroendocrine carcinomas are described [2]. There are various synonyms such as carcinoids, well/moderately/poorly differentiated carcinoids, Atypical Carcinoids, large/small cell neuroendocrine Carcinomas. The true incidence of Atypical carcinoid is unknown. Male:Female ratio is 3:1, with an average age of presentation 60 years. 75% of patients are smokers. Common symptoms are hoarseness, dysphagia, and respiratory distress. Most of these cancers are non-encapsulated and endophytic or exophytic. 50% of malignancy may show local, regional and distant metastasis. Histologically these malignancies may be mistaken for paragangliomas, metastatic medullary carcinomas of thyroid [3].
In view of high incidence of metastasis, combined chemo and radiotherapy is indicated rather than surgical ablation [4].
Case Report
An 85-year-old man presented to ENT OPD of our Hospital, with chief complaints of dysphagia and voluminous speech since 3 months. No H/o respiratory distress or hoarseness of voice. He was a beedi smoker for more than 40 years.
On examination, patient was edentulous. On indirect laryngoscopic examination, there was a pedunculated, smooth surfaced,grayish pink swelling seen occupying 3/4th of laryngeal inlet, moving with respiration. Vocal cords could not be visualized. No palpable lymph nodes in the neck was seen. Nose and Ears were within normal limits. Necessary investigations like Hb%, TC, DC, ESR, Blood Urea,Serum creatinine, FBS, PPBS were within normal limits. Chest X-ray (PA view) showed features of chronic bronchitis. No evidence of metastasis. On Soft tissue X-ray of neck (lateral view), a smooth surfaced circular opacity was seen at the supraglottic region [Table/Fig-1].
Showing X-ray of neck lateral view, a smooth surfaced circular opacity seen at the supraglottic region

ECG, 2D ECHO were within normal limits. Provisional Diagnosis of Laryngeal cyst was made. Pre-anaesthetic check up was done and accepted for surgical intervention. Elective tracheostomy was done. Anaesthetics were intubated through tracheostomy opening. Diagnostic direct Laryngoscopy was done. The swelling was attached to the right arytenoid with a pedicle [Table/Fig-2]. Vocal cords were visualized and free. Under microlaryngoscopy, the swelling was excised in Toto, sent for Histopathological examination.
Diagnostic direct Laryngoscopy showing the swelling attached to the right arytenoid with a pedicle

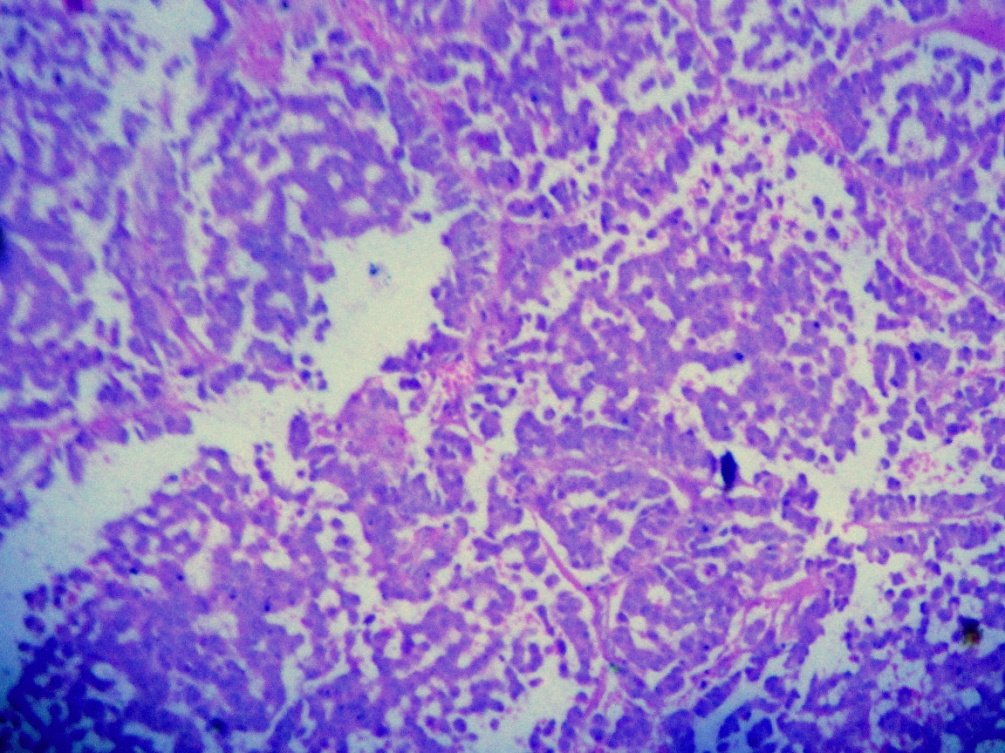
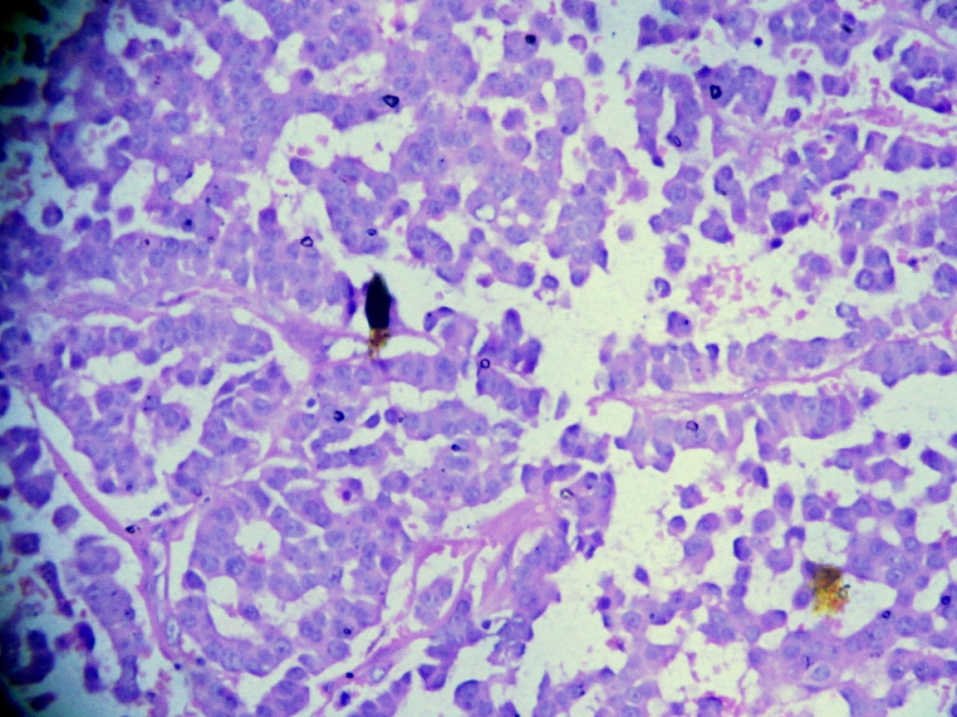
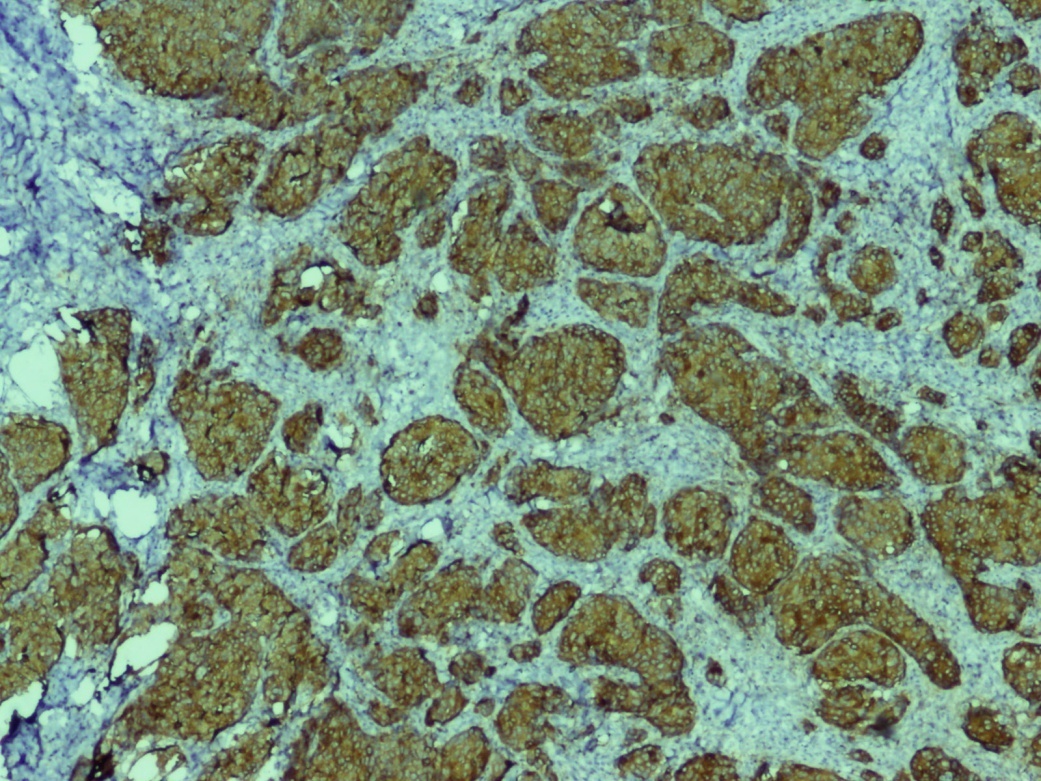
Post-operative period was uneventful. On 10th day after ascertaining the laryngeal airway by repeat Direct laryngoscopy, decannulation was done and the patient was discharged. Histopathological report was atypical carcinoid tumour [Table/Fig-3,4]. The diagnosis was confirmed by Immunohistochemistry for chromogranin, synaptophysin and cytokeratin. The Ki-67 index was 25% [Table/Fig-5].
Histopathology report – Atypical carcinoid tumour-Magnification -10X
Histopathology report – Atypical carcinoid tumour-Magnification -45X
Immunohistochemistry showing chromogranin positive
Discussion
Carcinoid tumours are derived from primitive stem cells in the gut wall but can be seen in other organs like lungs, larynx, bronchus, liver, pancreas, kidneys, ovaries, prostate and thymus [5].
Most carcinoid tumours are slow growing but aggressive and are known for metastasis. Carcinoid tumours are classified based on the location in the primitive gut i.e, foregut,midgut and hindgut that gives rise to the tumour [6].
Each of these entities are distinctive. Foregut carcinoids are ARGENTAFFIN negative and have low SEROTONIN content but secretes 5-hydroxy tryptophan (5-HTP). Midgut carcinoids are ARGENTAFFIN positive can produce high levels of SEROTONIN(5 Hydroxy Tryptamine-5-HT). Hindgut Carcinoids are ARGENTAFFIN negative and rarely secrete 5-HT or 5-HTP [7].
Histopathologically, carcinoid tumours are of NeuroEndocrine origin and are derived from primitive stem cells. The latest WHO classification [8] of tumours of upper respiratory tract divides the NEUROENDOCRINE neoplasma of Larynx into two types. 1) EPITHELIAL and 2) NERVOUS. First includes both typical and Atypical carcinoid tumour also called as Small cell neuroendocrine Tumour whereas the second includes Paragangliomas. Classic carcinoid tumours are ARGENTAFFINIC AND ARGYROPHILIC. At present immunostaining and hormonal markers are used for diagnosis [9].
Carcinoids may have SOMATOSTATIN receptors. Five identified somatostatin receptors are members of G Protein receptor family. Five distinct genes on chromosomes 11,14,16,17 and 20 encode somatostatin receptors. Somatostatin receptors are used as advantage for diagnosing and treating this disease [7].
Carcinoid tumours have high potential for metastasis. These cells produce amounts of beta–catenin which enables the tumour adhesion, thus promoting metastasis. Induction of RAF-1 results in decreased adhesion of carcinoid cells and may be important in the metastatic process [10].
Incidence
Though they are very rare, incidence reported from USA (0.15%) [7], England (0.79%), Scotland (1.46%) are noteworthy. No such reports are available from India [11].
Diagnosis and Differential Diagnosis
Signs and symptoms of carcinoid tumours vary greatly and depend upon the size of the tumour and metastasis. Clinical features ranges from no tumour related findings to all symptoms of carcinoid syndrome. Anatomic prevalence of the tumour is found in various locations including lungs, trachea, bronchus, thymus, liver, appendix, rectum, kidneys, prostate, testes and ovary. In the present case it is Larynx. Diagnosis and differential Diagnosis may not be simple as the signs and symptoms may or may not be related to the tumour and symptoms related to the anatomical site may be misleading. Many a times the symptoms may be related to the chemical secretions(5-HT, 5-HTP), secreted by the tumour [7].
The etiology of carcinoid tumours is not exactly known. But genetic abnormalities are suspected. Reported chromosomal abnormalities include changes in the chromosome such as loss of heterogeneity and numerical imbalances [7].
Laboratory Diagnosis of these tumours depends on the identification of the characteristic BIOMARKERS of the diseases, measurement of BIOGENIC AMINE levels, (eg., SEROTONIN, 5HTP, CATECHOLAMINES and HISTAMINE) and their metabolites in the platelets, plasma and urine of the patient can be helpful in the diagnosis. Tumour imaging modalities have been used to detect carcinoid tumours. Depending upon the location of the tumour, the necessary modalities may be combined. Treatment options are surgical and chemotherapy for metastatic carcinoids. Surgical treatment of choice is the surgical excision. Historically surgical removal of the lesion along with the metastatic nodes have been established as the main stay of therapy in those individuals without distant disease, whether conservative or Total laryngectomy [12].
Atypical carcinoid tumour of the larynx treated with CO2 laser excision and repeated CO2 laser excision for recurrence after 18 months. The patient was healthy after 7 years of follow up [13]. Radiotherapy in a retrospective analysis is not found satisfactory [12].
Conclusion
Neuroendocrine Carcinomas are rarest among the rare Non–Squamous carcinomas of Larynx. As there is no specific symptoms and or signs, biopsy may help to throw some light. It should be kept in mind that carcinoid tumours may be histologically mislabeled as paragangliomas or metastatic carcinomas of thyroid. If the lesion exhibits symptoms related to its secretions (5HT, 5-HTP), IMMUNOSTAINS and Hormonal markers are used for diagnosis. Although most of the presently reported ones are post-operative, still a ray of suspicion should be borne in mind when diagnosing suspicious laryngeal disorders.
[1]. Browne J. Dale, Management of non epidermoid cancer of the larynx In: W. Frederick McGuirt, (ed). Current Concepts in Laryngeal Cancer IIThe Otolaryngologic Clinics of North America 1997 30(2):215-29. [Google Scholar]
[2]. Batsakis JG, el-Naggar AK, Luna MA, Neuroendocrine tumors of larynxAnn. Otol. Rhinol. Laryngol 1992 101:710-14. [Google Scholar]
[3]. Woodruff JM, Huvos AG, Erlandson RA, Shah JP, Gerold FP, JournalAm J Surg Pathol 1985 Nov 9(11):771-90. [Google Scholar]
[4]. Batsakis JG, Luna MA, Byers RM, Metastases to the larynxHead Neck Surg 1985 7:458-60.[PubMed] [Google Scholar]
[5]. Broaddus RR, Herzog CE, Hicks MJ, Neuroendocrine tumors (carcinoid and neuroendocrine carcinoma) presenting at extra-appendiceal sites in childhood and adolescenceArch Pathol Lab Med Sep 2003 127(9):1200-3. [Google Scholar]
[6]. Tebbi CK, Carcinoid Tumor K, Sakamoto M, Windle T, Cripe S, Gross M, In eMedicine Journal 2007 8(2) [Google Scholar]
[7]. Tebbi CK. Carcinoid Tumor. http://emedicine.medscape.com/article/986050-overview [Google Scholar]
[8]. Shanmugaratnam K, Sobin LH, World Health Organization. International histological classification of tumoursHistological typing of tumours of the upper respiratory tract and ear 1991 2nd edBerlinSpringer-Verlag [Google Scholar]
[9]. Wilander E, Portela-Gomes G, Grimelius L, Argentaffin and argyrophil reactions of human gastrointestinal carcinoidsGastroenterology 1977 73:733-36. [Google Scholar]
[10]. Greenblatt DY, Kunnimalaiyaan M, Chen H, Raf-1 activation in gastrointestinal carcinoid cells decreases tumor cell adhesionAm J Surg Mar 2007 193(3):331-5. [Google Scholar]
[11]. Newton JN, Swerdlow AJ, dos Santos Silva IM, The epidemiology of carcinoid tumours in England and ScotlandBr J Cancer Nov 1994 70(5):939-42. [Google Scholar]
[12]. Woodruff JM, Senie RT, Atypical carcinoid tumor of the larynx. A critical review of the literatureORL J Otorhinolaryngol Relat Spec 1991 53:194-209. [Google Scholar]
[13]. Piazza C, Giudice M, Berlucchi M, Peretti G, Antonelli AR, Atypical carcinoid tumour of the larynx treated with CO2 laser excision: case reportActa Otorhinolaryngol Ital 2003 23:43-46. [Google Scholar]