Introduction
Transposition is a unique and an extreme form of ectopic eruption in which a permanent tooth develops and erupts in the position which is normally occupied by other permanent teeth (Shapira et al.,1989) [1]. To avoid confusion, it may be made clear that ‘ectopic eruption’ refers to any aberrant or abnormal eruption path which is taken by a tooth and that the term, ‘transposition’ refers to an interchange in the position of two adjacent teeth which are located within the same quadrant of the dental arch [2]. Tooth transpositions are rare and they can be complete or incomplete. The difference between the two types is that in a complete transposition case, crowns and roots of the involved teeth are in the transposed position, whereas in an incomplete transposition case, the crowns may be transposed, although the root apices remain in their normal positions [1,3].
The aetiology of a transposition is still obscure. Transposition of tooth buds at anlage stage, migration of a tooth during eruption, heredity, and trauma have been proposed as the possible aetiologic factors [4,5].
Various populations have been studied to determine the prevalence of tooth transpositions and these include Indian Chattopadhyay et al., [6], African Burnette et al., [7], Swedish Thilander et al., [8], Saudi Arabian Ruprecht et al., [9], Turkish Yilmaz et al., [10] and Scottish Sandham et al., [11] populations.
Transpositions have been classified according to Peck and Peck [12] as:
Maxillary canine-first premolar (Mx.C.P1)
Maxillary canine-lateral incisor (Mx.C.I2)
Maxillary canine to first molar site (Mx.C to M1)
Maxillary lateral incisor-central incisor (Mx.I2.I1)
Maxillary canine to central incisor site (Mx.C to I1)
Mandibular lateral incisor-canine (Mn.I2.C)
Peck et al., [12] stated that 20% of the transpositions which occur on the maxillary arch involve the canine and the lateral incisor. Although they are rare, transpositions may involve the maxillary lateral and central incisors. Among all transpositions, Mn.I2.C is rare, with a prevalence rate of 0.03% [6,13].
Tooth transpositions can hinder aesthetic and functional aspects of dentition and accordingly, it is important to know the variables which are related to the aetiology and prevalence of this anomaly, in order to establish possible preventive measures [14].Various other factors have also been proposed regarding the aetiology of transposition abnormalities, which include a genetic interchange in the position of the developing tooth buds, lack of root resorption of primary canine, mechanical interferences which come in way of erupting permanent teeth, early loss and /or prolonged retention of deciduous teeth [15].
Tooth transpositions often coexist and they are related to other pathological entities or anomalies of the dental arch, a fact which suggests the presence of a syndromic condition. In some patients, one may also observe peg-shaped maxillary lateral incisors, congenitally missing teeth other than third molars, persistence of primary teeth, severe rotations and poor alignment of heterotopic teeth or of their neighbouring teeth, supernumerary teeth, ectopic eruption of non-neighbouring teeth and root ankylosis. Their prevalences vary, according to different authors and they were found to occur in 0.38% patients in Turkey, 0.13% patients in Saudi Arabia, 0.43% patients in India and in 0.14% patients in Nigeria [16].
Although various reports have been published on tooth transpositions, very few have noted the agenesis of teeth other than third molars in the mandibular arch. There is considerable evidence which suggests that genes play a fundamental role in the aetiology of tooth agenesis. A study was conducted on children with tooth agenesis and it reported that siblings and relatives more than 50% of patients had presented with hypodontia, which was a high prevalence as compared to the expected prevalence which was seen in the general population [17].
Inheritance on an autosomal dominant basis, has also been proposed Pirinen et al., [18]. Hypodontia of teeth may be caused by one major gene mutation, but it is very often heterogenic Arte et al., [19].
Peck et al., analyzed the pattern of hypodontia which was associated with a palatally displaced canine (PDC), Mx.C.P1 and other variations of canine transposition. The third molar (M.3) was found to be strongly associated with mandibular incisor-canine transposition (Mn.I1.C) and PDC. In view of this, the homeobox genes, MSX1 and PAX9, which are associated with posterior field hypodontia, have been suggested to be the candidate genes for the control of Mn.I2.C and PDC [20].
Peck et al., described the characteristics of early stage mandibular incisor canine (Mn.I2.C) transposition: distal tipping, coronal displacement, and severe mesiolingual rotation (from 60° to 120°) of the mandibular lateral incisor, which prompt the adjacent canine to become mesially transposed. In the later stages, eruption of the mandibular-canine and its transposition with the lateral incisor can be detected [21].
The main goal of treatment of all transposition abnormalities is to correct the positions of transposed teeth.
Shapira et al., proposed that the treatment of transposed teeth involved fixed orthodontic appliances and treatment modalities which depended on the types of the involved teeth and their eruption stages [22].
Canoglu et al., reported the management of a complete type of Mn.I2.C with use a removable appliance [15].
Clinical Case
A 11-year-old male child reported with chief complaint of decay in lower left back tooth region. The clinical examination showed that there was dental caries in relation to 75, with a mixed dentition which had an end-on molar relation with an increased over bite. [Table/Fig-1,2].


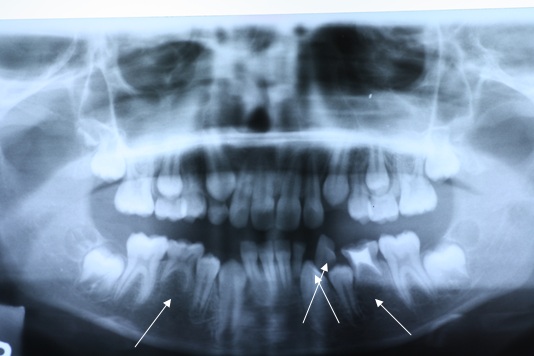
Further examination revealed 33 erupting buccally between 32 and retained 72 on the left quadrant. A mesio lingual rotation was noticed in 32 and 33. Ortho pantomographs (OPGs) [Table/Fig-3] and periapical [Table/Fig-4] and occlusal radiographs [Table/Fig-5] were advised. A radiographic examination confirmed the presence of an incomplete type of transposition, wherein there was superimposition of roots of both 32 and 33. OPG picture showed the agenesis of 35 and 45.


An orthodontic opinion was sought, following which it was decided to allow 33 to erupt in the transposed position. It was also decided to retain 75 and 85, as the second premolars were congenitally missing. Fixed appliance therapy was planned for the correction of the malocclusion, deep bite and teeth rotations. As a precursor to the planned treatment,72 was extracted to aid in the eruption of the involved teeth, followed by restoration of 75 and a crown placement on 85.The patient was recalled after 6 months for commencement of orthodontic therapy.
Discussion
Several factors have been proposed regarding the aetiology of transposition abnormalities. In recent years, research has attempted to determine the aetiologic factors of different transposition abnormalities. Peck et al., (1993) [23], suggested a genetic influence of the maxillary canine and the first premolar transposition. They also found a strong relationship between Mn.I2.C, tooth agenesis and a peg-shaped maxillary lateral incisor and concluded that the Mn.I2.C anomaly was genetically determined [21].It was also reported that the main cause of transposition in the maxilla was the displacement and migration of the canine, whereas in the mandible, it was caused by the distal migration of the lateral incisor [1].
Although the main goal of treatment of all transposition abnormalities is to correct the position of transposed teeth, several factors which include patient’s age, occlusion, aesthetics and treatment length, should be taken into consideration, in order to prevent any damage which can be caused to the teeth and supporting structures.Mn.I2.C is reported to be seen less often in the mandible than in the maxilla [6].
Keeping in mind the above mentioned factors, two treatment approaches have been suggested for Mn.I2.C: [1,21,24–27].
If the transposition is in an early stage, the position of the teeth can be corrected with the aid of fixed orthodontic treatment. However, one primary anterior tooth can be extracted to facilitate an early correction.
1. If the transposition is recognized after the transposed teeth have erupted in their transposed positions or where the roots of the involved teeth are parallel, it is not preferred to correct the position of the involved teeth. Because of the dense compact bone of the mandible, the teeth should be aligned in their transposed forms.
In our case, 32 had already erupted and 33 was erupting labially in the former’s position. The radiographic picture shows the roots of the transposed teeth to be almost parallel. In the present case, the start of the treatment differed mainly, owing to the following factors:
Age of the child
Hypodontia
Relatively intact roots of the mandibular second primary molars.
In the literature, all transposition cases were found to be treated with fixed orthodontic treatment, barring one, which was treated by using a removable appliance [15].
The present case was a case of transposition with associated hypodontia, which did not involve space problems during orthodontic treatment. Owing to these factors, it was decided to extract the retained 72, to allow 33 to erupt in its place and to retain the 75 and 85, owing to agenesis (hypodontia) of 35 and 45. The initiation of the fixed orthodontic therapy was planned after the exfoliation of other primary teeth present in the maxillary arch. The patient has been kept under regular observation.
Conclusion
Within the limits of the present case, we can conclude that this was a rare combination of Mnd.I2.C with hypodontia (agenesis of 35 and 45), which had led to the retention of 75 and 85, owing to agenesis of their successors. 33 could be allowed to erupt into the transposed space, to facilitate orthodontic therapy for correcting the malocclusion, deep bite and teeth rotations.
[1]. Shapira Y, Kuftinec MM, Maxillary Canine – Lateral Incisor Transposition- Orthodontic ManagementAmerican Journal of Orthodontics and Dentofacial Orthopaedics 1989 95:439-44. [Google Scholar]
[2]. Shapira Y, Kuftinec MM, Tooth Transpositions- A Review Of The Literature And Treatment ConsiderationsAngle Orthodontics 1989 59:271-6. [Google Scholar]
[3]. Shapira Y, Kuftinec MM, Maxillary Tooth Transpositions: Characteristic Features And Accompanying Dental AnomaliesAmerican Journal of Orthodontics and Dentofacial Orthopaedics 2001 119:127-34. [Google Scholar]
[4]. Joshi MR, Bhatt NA, Canine TranspositionOral Surgery Oral Medicine Oral Pathology 1971 31:49-54. [Google Scholar]
[5]. Shapira Y, Transposition Of CaninesJournal of American Dental Association 1980 100:710-2. [Google Scholar]
[6]. Chattopadhyay A, Srinivas K, Transposition of Teeth And Genetic EtiologyAngle Orthodontics 1996 66:147-52. [Google Scholar]
[7]. Burnett SE, Prevalence Of Maxillary Canine-First Premolar Transposition In A Composite African SampleAngle Orthodontics 1999 69:187-9. [Google Scholar]
[8]. Thilander B, Jakobsson SO, Local Factors In Impaction Of Maxillary CaninesActa Odontologica Scandinavica 1968 26:145-68. [Google Scholar]
[9]. Ruprecht A, Batniji S, El-Neweihi E, The Incidence Of Transposition Of Teeth In Dental PatientsJournal of Pedodontics 1985 9:244-9. [Google Scholar]
[10]. Yilmaz HH, Turkkahraman H, Sayin MO, Prevalence Of Tooth Transpositions And Associated Dental Anomalies In A Turkish PopulationDentomaxillofacial Radiology 2005 34:32-5. [Google Scholar]
[11]. Sandham A, Harvie H, Ectopic Eruption Of The Maxillary Canine Resulting In Transposition With Adjacent TeethTandlaegebladet 1985 89:9-11. [Google Scholar]
[12]. Peck S, Peck L, Classification Of Maxillary Tooth TranspositionsAmerican Journal of Orthodontics and Dentofacial Orthopaedic 1995 107:505-17. [Google Scholar]
[13]. Jarvinen S, Mandibular Incisor-Cuspid Transposition: A SurveyJournal of Pedodontics 1982 6:159-63. [Google Scholar]
[14]. Beatriz Silva CM, Jose Carlos MC, Marcio M, Ana Paula Pereira PA, Tooth Transposition-A Litreature Review And A Clinical CaseBrazilian Journal of Oral Sciences 2006 5(16):953-7. [Google Scholar]
[15]. Canoglu E, Kocadereli I, Turgut MD, Alignment Of Transposed Mandibular Lateral Incisor And Canine Using Removable AppliancesAustralian Dental Journal 2009 54:266-70. [Google Scholar]
[16]. Maria Hatzoudi, Moschos A.Papadopoulos, Prevalence Of Tooth Transposition In Greek PopulationHellenic Orthodontic Review 2006 9(1):11-22. [Google Scholar]
[17]. Daniela GG, Peck S, Gomes SC, Increased Occurrence Of Dental Anomalies Associated With Second-Premolar Agenesis 2009 79(3):436-41. [Google Scholar]
[18]. Pirinen S, Arte S, Apajalahti S, Palatal Displacement Of Canine Is Genetic And Related To Congenital Absence Of TeethJournal of Dental Research 1996 75:1742-46. [Google Scholar]
[19]. Arte S, Nieminen P, Apajalahti S, Haavikko K, Thesleff I, Pirinen S, Characteristics Of Incisor-Premolar Hypodontia In FamiliesJournal of Dental Research 2001 80:1445-50. [Google Scholar]
[20]. Peck S, Peck L, Kataja M, Concomitant Occurrence Of Canine Malposition And Tooth Agenesis:Evidence Of Orofacial Genetic FieldsAmerican Journal of Orthodontics and Dentofacial Orthopaedics 2002 122:657-60. [Google Scholar]
[21]. Peck S, Peck L, Kataja M, Mandibular Lateral Incisor-Canine Transposition, Concomitant Dental Anomalies And Genetic ControlAngle Orthodontics 1998 68:455-66. [Google Scholar]
[22]. Laptook T, Silling G, Canine Transposition – Approaches To TreatmentJournal of American Dental Association 1983 107:746-8. [Google Scholar]
[23]. Peck L, Peck S, Attia Y, Maxillary Canine-First Premolar Transposition, Associated Dental Anomalies And Genetic BasisAngle Orthodontics 1993 63:99-109.Discussion 110 [Google Scholar]
[24]. Shapira Y, Kuftinec MM, The Ectopically Erupted Mandibular Lateral IncisorAmerican Journal of Orthodontics 1982 82:426-9. [Google Scholar]
[25]. Taner T, Uzamis M, Orthodontic Management Of Mandibular Lateral Incisor-Canine Transpositions: Report Of CasesASDC Journal of Dentistry for Children 1999 66:110-5. [Google Scholar]
[26]. Weeks EC, Power SM, The Presentations And Management Of Transposed TeethBritish Dental Journal 1996 181:421-4. [Google Scholar]
[27]. Payne GS, Bilateral Transposition Of Maxillary Canines And Premolars. Report of Two CasesAmerican Journal of Orthodontics 1969 56:45-52. [Google Scholar]