Spontaneous Discharging Umbilical Sinus Secondary to Infected Cystic Teratoma Ovary: An Atypical Presentation
Arpan Choudhary1, Samir Shukla2, Pragyey Nawlakhey3, Romil Jain4, Mahim Koshariya5
1 Resident, Department of Surgery, Gandhi Medical College & Associated Hamidia Hospital, Bhopal, Madhya Pradesh, India.
2 Assistant Professor, Department of Surgery, Gandhi Medical College & Associated Hamidia Hospital, Bhopal, Madhya Pradesh, India.
3 Resident, Department of Surgery, Gandhi Medical College & Associated Hamidia Hospital, Bhopal, Madhya Pradesh, India.
4 Resident, Department of Surgery, Gandhi Medical College & Associated Hamidia Hospital, Bhopal, Madhya Pradesh, India.
5 Associate Professor, Department of Surgery, Gandhi Medical College & Associated Hamidia Hospital, Bhopal, Madhya Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mahim Koshariya, D-102/10, Shivaji Nagar, Bhopal, Madhya Pradesh-462016, India.
Phone: 9826031583,
E-mail: mahimk2000@yahoo.co.uk
Mature cystic teratomas are the most common ovarian neoplasm in patients younger than 20 years. Its complications include torsion, rupture, infection and malignant degeneration. Infection of teratoma is an uncommon event. We are reporting the first ever case of infected mature cystic teratoma presented as a chronic discharging sinus via umbilicus. 30 years old young primipara presented with complaint of seropurulent discharge from umbilicus for 6 months. Ultrasonography showed right sided complex adnexal mass. Umbilical exploration revealed sinus tract travelling deep into the pelvis attached to right ovarian mass. Salpingo- oopherectomy was done on right side and sinus tract excised. Cut-section of specimen showed heterogeneous mass of soft tissue with intact capsule containing hairs, cheesy white purulent material, fat and cartilage. Biopsy was suggestive of mature ovarian cystic teratoma.
Chronic discharging Sinus, Infected Cystic Teratoma, Umbilical sinus
Case Report
Case
A 30 yrs old young primipara presented to surgery department with complaint of seropurulent discharge from umbilicus for 6 months. There was no history of previous pain or swelling over umbilicus, trauma, abdominal operation, fever, abdominal pain or mass. Physical examination revealed soft abdomen with vague ill defined lump felt in right inguinal region. Per-rectal examination was unremarkable. On per-vaginal examination fullness was noted in right fornix. Routine investigations were normal. Ultrasonography showed right sided complex adnexal mass. Sinogram could not be obtained as the opening could not be negotiated.
Treatment
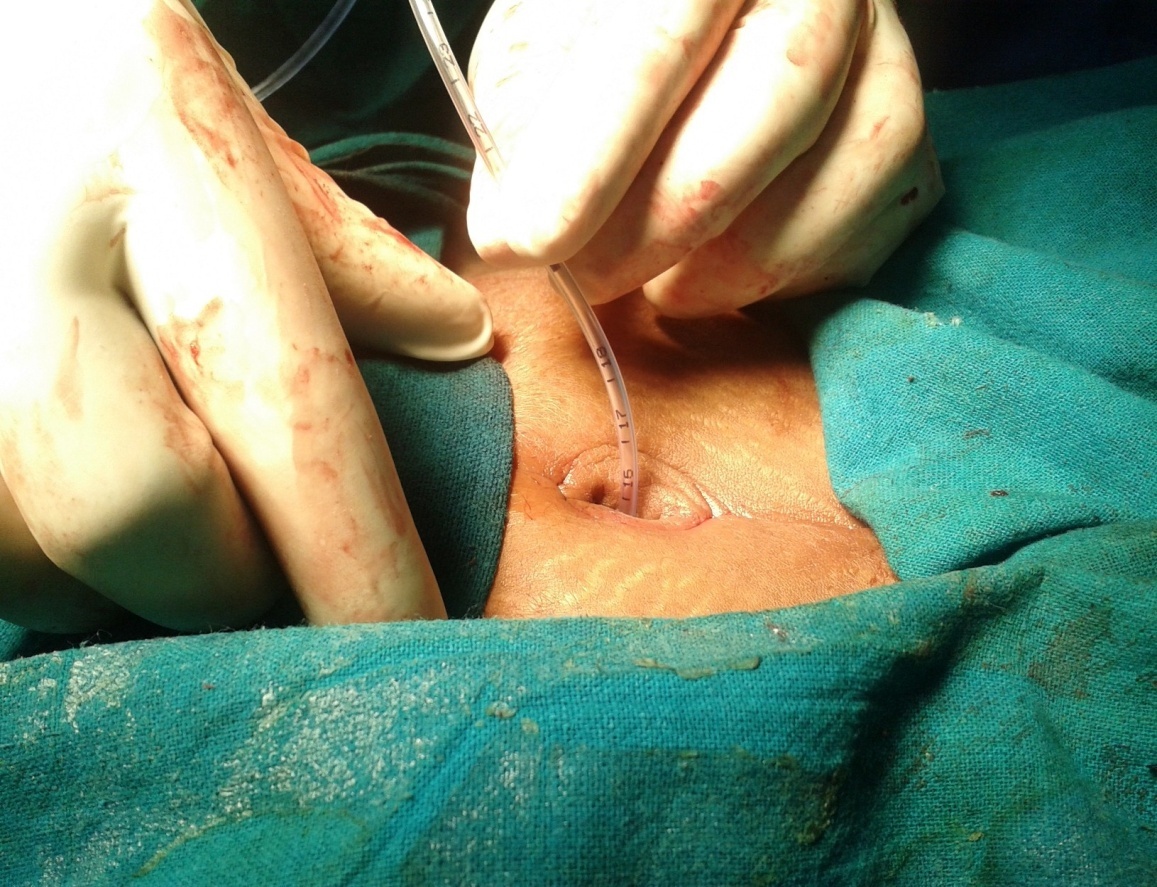
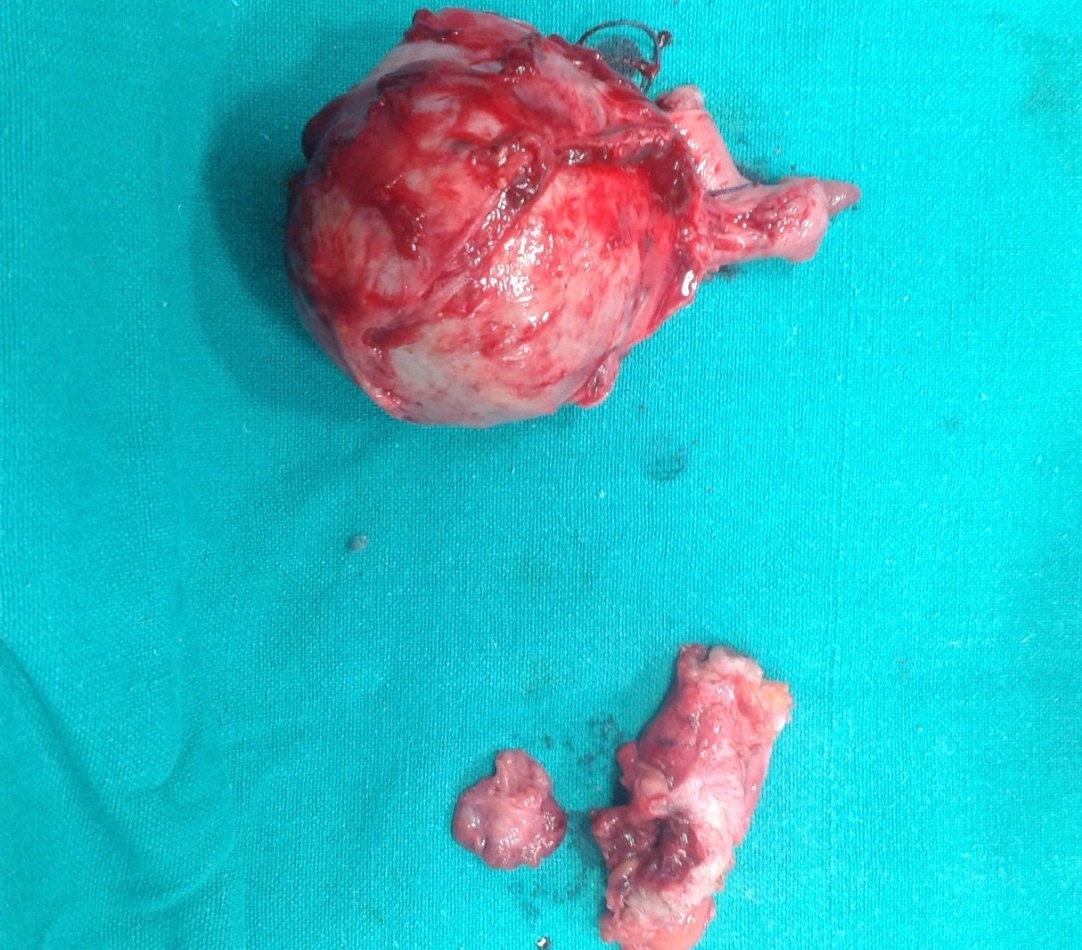
In ambiguity of diagnosis, umbilical exploration was planned. Under anaesthesia with local dilatation 6 Fr feeding tube was inserted via umbilicus [Table/Fig-1]. Further exploration revealed sinus tract travelling deep into the pelvis attached to right ovarian mass [Table/Fig-2]. Salpingo-oopherectomy was done on the right side and sinus tract was excised. Cut section of specimen showed heterogeneous mass of soft tissue with intact capsule containing hairs, cheesy white purulent material, fat and cartilage [Table/Fig-3, 4]. Post-operative period was uneventful. Biopsy was suggestive of mature ovarian cystic teratoma. At the 10 months of follow-up it was found that patient was doing well without any recurrence of sinus or any complaints.
Umbilical sinus with feeding tube in situ
Umbilical sinus tract travelling down into pelvis attached to ovarian mass

Excised specimen of ovarian mass along with sinus tract
Cut section of ovarian mass containing hair, cheesy material, cartilage and fat

Discussion
Mature cystic teratomas account for 10-20% of all ovarian neoplasms. They are the most common ovarian germ cell tumor and also the most common ovarian neoplasm in patients younger than 20 years [1,2]. Its complications include torsion, rupture, infection and malignant degeneration. Infection is uncommon and occurs in less than 1-2% of cases, usually presents as abdominal pain and enlarging lump, but never as a sinus [3,4].
Teratomas are made up of a variety of parenchymal cell types representing more than 1 germ layer and often all 3. By far, the most common gonadal location is the ovary. Cells differentiate along various germ lines, essentially recapitulating any tissue of the body. Examples include hair, teeth, fat, skin, muscle, and endocrine tissue. Mature cystic teratomas account for 10-20% of all ovarian neoplasms. They are bilateral in 8-14% of cases [1]. Cystic teratoma affects women during reproductive years. Most are asymptomatic to start with, later on an enlarging mass produces vague abdominal lump, pain or abnormal uterine bleeding. Pain is usually dull aching, moderate to severe in intensity and remains constant. Torsion and hemorrhage present as acute abdomen and confer surgical emergency. Other complications include infection, adhesions, malignant regeneration and hemolytic anemia. Symptoms of infections include fever, pain abdomen, dysuria and vaginal discharge, but presentation as spontaneously discharging sinus has never been reported.
Workup includes abdominal and transvaginal USG, CT and MRI abdomen and pelvis [5]. Tumor marker such as AFP and hCG are normal in benign variety [6]. FNAC and core needle biopsy may be done to differentiate the malignant degeneration. Histologically, tumor wall is lined by native ovarian tissue containing different tissues arising from 3 germ lines. Ectodermal tissue encountered may include brain, glia, neural tissue, retina, choroids, and ganglia. Mesodermal tissue is represented by bone, cartilage, smooth muscle, and fibrous tissue [7]. Intraperitoneal extension ensues dense intra-abdominal adhesions.
Treatment should include salpino-oopherectomy with complete removal of mass, and spillage of content should be avoided. If immature elements are found, then patient should undergo standard staging procedure [8]. Laparoscopy is a good alternative to open surgery. Risk of recurrence and malignant degeneration should be foretold.
Conclusion
Infection of mature cystic teratoma is an uncommon event. It should be considered as a differential diagnosis in a young female with mass per abdomen, pain abdomen, fever and discharging sinus. Prompt surgery and antibiotic coverage is the treatment of choice. Here we are reporting first ever case of infected mature cystic teratoma presented as a chronic discharging sinus via umbilicus treated successfully.
[1]. Pantoja E, Noy MA, Axtmayer RW, Colon FE, Pelegrina I, Ovarian dermoids and their complications. Comprehensive historical reviewObstet Gynecol Surv Jan 1975 30(1):1-20. [Google Scholar]
[2]. Comerci JT Jr, Licciardi F, Bergh PA, Gregori C, Breen JL, Mature cystic teratoma: a clinicopathologic evaluation of 517 cases and review of the literatureObstet Gynecol Jul 1994 84(1):22-8. [Google Scholar]
[3]. Benjapibal M, Boriboonhirunsarn D, Suphanit I, Sangkarat S, Benign cystic teratoma of the ovary : a review of 608 patientsJ Med Assoc Thai Sep 2000 83(9):1016-20. [Google Scholar]
[4]. Ayhan A, Bukulmez O, Genc C, Karamursel BS, Ayhan A, Mature cystic teratomas of the ovary: case series from one institution over 34 yearsEur J Obst et Gynecol Reprod Biol 2000 88(2):153-7. [Google Scholar]
[5]. Outwater EK, Siegelman ES, Hunt JL, Ovarian teratomas: tumor types and imaging characteristicsRadiographics 2001 21(2):475-90. [Google Scholar]
[6]. Billmire DF, Grosfeld JL, Teratomas in childhood: analysis of 142 casesJ Pediatr Surg 1986 21(6):548-51. [Google Scholar]
[7]. Talerman A, Germ Cell Tumors of the Ovary. In: Kurman RJ, edBlaustein’s Pathology of the Female Genital Tract 2002 5th edNew York, NYSpringer-Verlagchap 20 [Google Scholar]
[8]. Templeman CL, Fallat ME, Lam AM, Perlman SE, Hertweck SP, O’Connor DM, Managing mature cystic teratomas of the ovaryObst et Gynecol Surv 2000 55(12):738-45. [Google Scholar]