Early Universal Screening for Gestational Diabetes Mellitus
Ramya Neelakandan1, Prabhu Shankar Sethu2
1 Assistant Professor, Department of Medicine, Chennai Medical College Hospital & Research Centre, Tiruchirapalli, Tamil Nadu, India.
2 Professor, Department of Medicine, Chennai Medical College Hospital & Research Centre, Tiruchirapalli, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ramya Neelakandan, FF1, Abinaya Residency, A62, Sivaprakasam Salai, Thennur, Anna Nagar, Tiruchirapalli-620017, Tamil Nadu, India.
Phone: 9894835015,9944129767
E-mail: dr.ramyamd@yahoo.com
Objective: To study the prevalence of Gestational diabetes mellitus and to assess the impact of early universal screening to detect Gestational diabetes mellitus.
Materials and Methods: Consecutive 1106 pregnant women were screened for Gestational diabetes mellitus at their first prenatal visit during the study period of February 2012 to January 2013. All the women were screened with a initial 50 gram one hour glucose challenge test (GCT) and those women who tested positive were subjected to a standardized 75 gram oral glucose tolerance test(OGTT). The prevalence of Gestational diabetes mellitus and its association with age, infertility, obesity, hypertension, family history of diabetes was studied. The impact of early universal screening for GDM was assessed. American diabetic association (ADA) and International Association of Diabetes in Pregnancy Study Group (IADPSG) criteria for diagnosis of Gestational diabetes mellitus was used in our study.
Results: Of the total 1106 pregnant women who were screened with the initial 50 gram one hour glucose challenge test (GCT), 458 (41.4%) had their one hour plasma glucose value >130 gm/dl. Of the 440 women who responded to and underwent the subsequent 75gram OGTT, 158 (61.2%) had one abnormal value, 73(28.2%) had two abnormal values and 27 (10.5%) had three abnormal values. 64(24.8%) of them had fasting plasma glucose ≥ 92/dl. 36(13.9%) women were found to have GDM in the first trimester (12 weeks), 43 (16.7%) in the 13-18 weeks, 114 (44.1%) in the 19-28 weeks and 65 (25.2%) in the third trimester(28 weeks). The overall prevalence of GDM was 23.3%. There was increased association of GDM with increasing age, parity, family predisposition and infertility.
Conclusion: It is evident that there is increased prevalence of GDM in Indian population. Universal screening for GDM is better to routine risk factor based screening and it should be done at the first prenatal visit for early diagnosis of glucose intolerance in pregnancy especially in countries like India. There is increased association of GDM with infertility, advanced age, obesity, family predisposition and parity.
Gestational diabetes mellitus, Early universal screening, Prevalence, OGTT
Introduction
Gestational Diabetes Mellitus is defined as glucose intolerance of varying severity that has its onset or first recognition during pregnancy [1]. The prevalence of GDM is increasing globally [2] especially in Asian women [2] and in the whole world, India has the highest number of type 2 diabetes patients [3]. The common risk factors for GDM include family history of diabetes in first degree relative, higher age, overweight and history of delivery of large babies in previous pregnancy [4]. GDM increases the incidence of both maternal and fetal complications [5] and also predisposes the women for the future risk of diabetes mellitus [6]. In India, screening is essential universally in all women diagnosed to be pregnant, as they have 11 fold increased risk of developing glucose intolerance during pregnancy compared to Caucasian women [7]. The recent data on the prevalence of GDM in India was 16.55% [8]. In our study, we have studied the prevalence of GDM, the importance of early universal [9] screening for GDM at the first prenatal visit irrespective of presence of risk factors for GDM and we have also characterized the patients in relation to weight, age, family history of diabetes, parity, infertility.
Materials and Methods
This study was carried out in Tiruchirappalli, Tamilnadu, India during the period February 2012 to January 2013. A proper ethics approval from the Human Institutional ethics committee was obtained. Consecutive 1106 pregnant women attending the antenatal clinic were screened for Gestational diabetes mellitus immediately after diagnosis of pregnancy at their first prenatal visit. The details of age,height,weight, history of diabetes in the family, history of GDM in previous pregnancy, history of previous delivery of large babies, socio-economic status, history of infertility was obtained. The body mass index (BMI) of the subjects was calculated using the height and weight. Blood pressure of all the women was recorded. All the women were subjected to a 50 gram one hour glucose challenge test at their first antenatal visit and the venous blood was collected after one hour. All those women who had the 1 hour plasma glucose value >130 gm/dl [8,10] were requested to have an unrestricted regular diet and return after 72 hours in the morning with a overnight fasting of at least 8 hours for the standardized 75 gram oral glucose tolerance test (OGTT). Recent American diabetic association (ADA) [11] and International Association of Diabetes in Pregnancy Study Group (IADPSG) [12] which recommends any one value of the fasting plasma glucose (FPG) > or = 92 mg/ dl, 1-hour plasma glucose > or = 180 mg/dl or 2-hour plasma glucose > or = 153 mg/dl to diagnose GDM was used in our study. If found negative at the first antenatal visit, the screening test was performed again around 24 to 28 weeks [13] and finally around 32 to 34 weeks. HbA1c was not done in our study, as it is not recommended as routine screening tool in GDM. Women with previous history of diabetes were excluded from the study.
Results
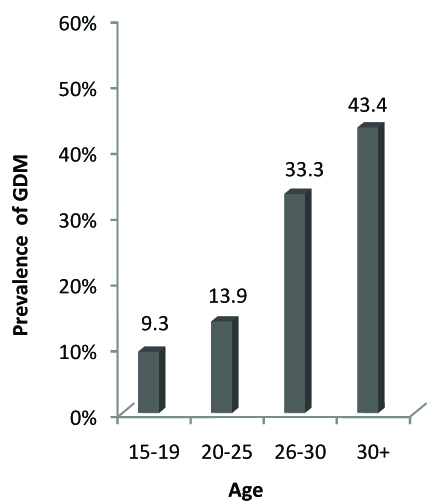
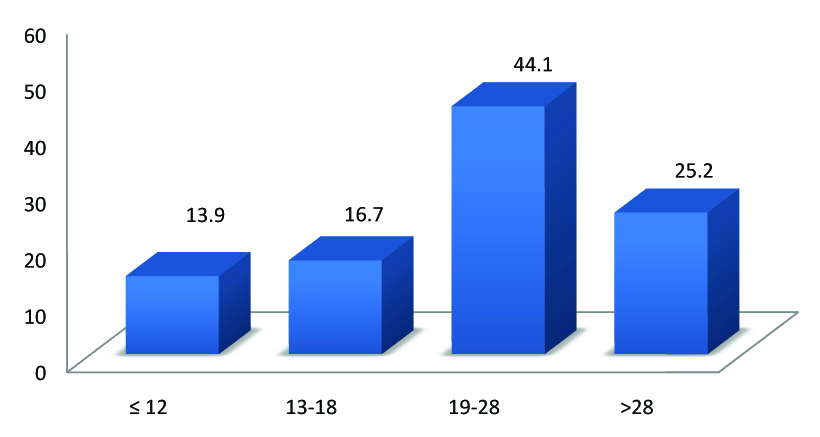
During the study period of 12 months, a total of 1106 pregnant women had the initial 50 gram-1 hour test (GCT). Of these, 458 (41.4%) had their one hour plasma glucose value >130 gm/dl. For the subsequent 75 gram-2 hour test, 440 women responded. Of the 440 women who underwent the 75g OGTT, 158 (61.2%) had one abnormal value, 73(28.2%) had two abnormal values and 27 (10.5%) had three abnormal values. 64(24.8%) of them had fasting plasma glucose ≥ 92/dl. Overall, a total of 258 women were diagnosed to have GDM and the overall prevalence of GDM was 23.3% The prevalence of GDM increased with age, from 9.3 % in the age group of 15-19 years to 43.4% for the age groups 30+ years [Table/Fig-1,2]. A total of 36 (13.9%) women were found to have GDM in the first trimester, 43 (16.7%) in the 13-18 weeks, 114 (44.1%) in the 19-28 weeks and 65 (25.2%) in the third trimester [Table/Fig-3,4].
| Age in years | No of GDM patients |
|---|
| 15-19 | 24 (9.3%) |
| 20-25 | 36 (13.9%) |
| 26-30 | 86 (33.3%) |
| 30+ | 112 (43.4%) |
Relationship between Age and Prevalence of GDM 2
Gestational week at Diagnosis of GDM
| Gestational week at Diagnosis of GDM | No of GDM patients |
|---|
| < 12 | 36 (13.9%) |
| 13-18 | 43 (16.7%) |
| 19-28 | 114 (44.1%) |
| >28 | 65(25.2%) |
Gestational week at diagnosis and Prevalence of GDM
Among the 258 women found to have GDM, 38 (14.7%) women had a BMI of <23, 96 (37.2%) had a BMI of 24-30 and 124 (48.0%) had BMI >30 [Table/Fig-5]. The prevalence of GDM increased from 14.7% for BMI <23 to 48% for BMI > 30. With regards to infertility,78 (30.2%) women had infertility and they have conceived after treatment for infertility [Table/Fig-5] and 103 (39.9%) women had a family history of diabetes mellitus in their first degree relatives, 56 (21.7%) had a history GDM in the previous pregnancy, 36(13.9%) had a history of abortions. 38 (14.7%) had a history of large babies in previous pregnancy.GDM increased with parity as 82(31.7%)women were primigravida and 176 (68.2%)women were multigravida [Table/Fig-5].
| Variables | No of GDM patients |
|---|
| BMI <23 | 38 (14.7%) |
| BMI 24-30 | 96 (37.2%) |
| BMI > 30 | 124 (48.0%) |
| Family history of diabetes | 103 (39.9%) |
| GDM in previous pregnancy | 56 (21.7%) |
| Large babies in previous pregnancy | 38 (14.7%) |
| Coexisting high BP | 49 (37.9%) |
| Infertility | 78 (30.2%) |
| Primigravida | 82 (31.7%) |
| Multigravida | 176 (68.2%) |
| History of miscarriage | 36 (13.9%) |
Discussion
Gestational Diabetes Mellitus is defined as glucose intolerance that has its onset or first recognition during pregnancy [1]. In India, screening is essential universally in all women diagnosed to be pregnant as they have a 11 fold increased risk of developing glucose intolerance during pregnancy compared to Caucasian women [7]. The usual recommendation for screening is between 24 and 28 weeks of gestation [13]. New concept is to screen for glucose intolerance in the first trimester [13] itself. Early universal screening [9,13] means screening all pregnant women soon after the diagnosis of pregnancy irrespective of presence of risk factors [14,15]. The data on the prevalence of GDM in India was 16.55% by WHO criteria of 2 hr PG ≥ 140 mg/dl [8]. The prevalence of GDM in our study was 23.3%, higher than reported in earlier studies [8,16] done in India, because in earlier studies routine screening was done at second or third trimester but, In our study we have done an early universal screening [14,15] at the first prenatal visit soon after diagnosis of pregnancy. The prevalence in the first trimester was 13.9% and in third trimester was 25.2%. The decrease in the prevalence in the third trimester when compared to earlier reports [8,16] was due to the early diagnosis of glucose intolerance in the first and second trimester due to early universal screening. There was an increased prevalence of GDM with advancing age, parity, body weight,and in women with family predisposition. In our study, we found an overall increased prevalence of GDM when using the ADA [11] and IADPSG [12] cut off values for diagnosis of GDM as in previous studies [17,16]. We also noted an increased prevalence of GDM in the first trimester(13.9%), and 56 women of the total 258 (21.7%) would not be identified, if the routine risk factor based screening[9,14,15] was used, as they did not have any of the common risk factors like age >25, overweight, family predisposition. With a good glycemic control in these GDM women, both the maternal and the fetal complications were avoided. Hence we stress the importance of screening all pregnant women in their first antenatal visit irrespective of the presence of risk factors, for early recognition and treatment of glucose intolerance in pregnancy, especially in India where diabetes is highly prevalent, so as to prevent the fetal and the maternal complications. We also want sensitize that all the patients with infertility should be screened for insulin resistance, as 78(30.2%) had infertility in our study.
Conclusion
In our study, it is evident that there is increased prevalence of GDM in Indian population. Universal screening for GDM is better to routine risk factor based screening and it should be done at the first prenatal visit for early diagnosis of glucose intolerance in pregnancy especially in countries like India. There is increased association of GDM with infertility, advanced age, obesity, family predisposition and parity.
[1]. Metzger BE, Coustan DR, Proceedings of the Fourth International Workshop Conference on Gestational Diabetes MellitusDiabetes Care 1998 21(Suppl 2):B1-B167. [Google Scholar]
[2]. Ferrara A, Increasing prevalence of gestational diabetes mellitus: a public health perspectiveDiabetes Care 2007 30(Suppl. 2):S141-6. [Google Scholar]
[3]. Wild S, Roglic G, Green A, Sicree R, King H, Global prevalence of diabetes estimates for the year 2000 and projections for 2030Diabetes Care 2004 27:1047-53. [Google Scholar]
[4]. American Diabetes Association.Gestational diabetes mellitusDiabetes Care 2003 26:s103-5. [Google Scholar]
[5]. Metzger BE, Lowe LP, Dyer AR, HAPO Study Cooperative Research Group. Hyperglycemia and adverse pregnancy outcomesN Engl J Med 2008 358:1991-2002. [Google Scholar]
[6]. Bellamy L, Casas JP, Hingorani AD, Williams D, Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysisLancet 2009 373:1773-9. [Google Scholar]
[7]. Dornhost A, Paterson CM, Nicholls JS, Wadsworth J, Chiu DC, Elkeles RS, High prevalence of GDM in women from ethnic minority groups Diabetic Med 1992 9:820-2. [Google Scholar]
[8]. Seshiah V, Balaji V, Madhuri S Balaji, Sanjeevi CB, Green A, Gestational Diabetes Mellitus in IndiaJ Assoc Physic of India 2004 52:707-11. [Google Scholar]
[9]. Hayes L, Bilous R, Bilous M, Brandon H, Crowder D, Emmerson C, Universal screening to identify gestational diabetes: A multi-centre study in the North of EnglandRecent Diabetes Research and Clinical Practice 2013 Apr 2 pii:S0168-8227.(13)00097-1. doi: 10.1016/j.diabres.2013.03.019 [Google Scholar]
[10]. Cheng YW, MnLaughlin Gb, Esakoff TF, Block-Kurbisch I, Glucose challenge test: screening threshold for gestational diabetes mellitus and associated outcomesJournal of Maternal Fetal Neonatal Medicine 2007 20(12):903-8. [Google Scholar]
[11]. Screening for and diagnosis of GDMDiabetes care 2013 36(suppl 1):S73Table 4 [Google Scholar]
[12]. Metzger BE, Gabbe SG, Persson B, International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancyDiabetes Care 2010 33:676-82. [Google Scholar]
[13]. Nahum GG, Wilson SB, Stanislaw H, Early-pregnancy glucose screening for gestational diabetes mellitusJ Reprod Med 2002 47:656-62. [Google Scholar]
[14]. Graziano Di Cianni, Volpe L, Lencioni C, Miccoli R, Prevalence and risk factors for gestational diabetes assessed by universal screeningDiabetes Research and Clinical Practice 2003 62(2):131-7. [Google Scholar]
[15]. Griffin M. E, Coffey M, Johnson H, Scanlon P, Universal vs. risk factor-based screening for gestational diabetes mellitus: detection rates, gestation at diagnosis and outcomeDiabetic Medicine 2000 17(1):26-32.:44 [Google Scholar]
[16]. Seshiah V, Balaji V, Shah Siddharth N, Shashank Diagnosis of Gestational Diabetes Mellitus in the CommunityJAPI 2012 :60 [Google Scholar]
[17]. Wery E, Vambergue A, Le goueff F, Vincent D, Deruelle P, Impact of the new screening criteria on the gestational diabetes prevalenceJ Gynecol Obstet Biol Reprod. (Paris) 2013 25:S0368-2315.(13) [Google Scholar]