Variation in Formation of Superficial Palmar Arches with Clinical Implications
Sheetal Bhimprasad Joshi1, P. Vatsalaswamy2, B.H. Bahetee3
1 Assistant Professor, Department of Anatomy, B.J. Government Medical College, Pune, Maharashtra, India.
2 Professor, Department of Anatomy, Dr. D.Y. Patil Medical College, Pune, Maharashtra, India.
3 Professor and Head, Department of Anatomy, B.J. Government Medical College, Pune, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sheetal Bhimprasad Joshi, Waterlily-B, Flat No. 1, Sukhawani Campus, Pimpri, Pune-18, Maharashtra, India.
E-mail: drsheetalbjoshi@rediffmail.com
Phone: 9049987004
Background: Knowledge of the variations in the arterial supply of hand has reached a point of practical importance with the advent of microvascular surgery for revascularization, replantation and composite tissue transfers. Arterial supply of hand is derived from two anastomotic arches, formed between two main arteries of forearm i.e. radial, ulnar and their branches, in the palm.
Objective: The superficial palmar arch shows variation in formation at the radial side. In the present study we have recorded its data which would help in its clinical and surgical implications.
Materials and Methods: In the present study we have studied the formation of superficial palmar arches and their variations in 100 cadaveric hands at Dr. D . Y. Patil Medical College, Pune and B.J. Government Medical College, Pune, India.
Result and Conclusion: According to Adachi’s classification the most predominant pattern obseved was of Ulnar type arch (66%). According to Coleman and Anson classification 82% showed complete (Group I) superficial palmar arches and a very low incidence (18%) of incomplete arches (Group II). This suggests that collateral circulation is present in majority of cases. This would result in least number of complications considering radial artery harvesting for coronary bypass. Sub-classification of arches according to Coleman and Anson 1961 indicates that the predominant type in the present study was of Group I (Type B) which is formed entirely by Ulnar Artery (56%). Median artery and ulnar artery forming an incomplete superficial arch under Group II (Type C) having an incidence of 4% was recorded. Thus in such cases radial artery harvesting for coronary artery bypass may prove to be less fatal. This study is an effort to provide data about the formation of superficial palmar arches which has been a centre of attraction for most of the surgical procedures and injuries of the hand.
Superficial palmar arch, Ulnar artery, Median artery
Introduction
Human hand is highly evolved in terms of its complexity and variation. It is beyond doubt that, in this medical era vascular anatomy of human hand is of importance in medical, surgical and radiological sciences [1].
Knowledge of the variations in the arterial supply of hand is essential in advent of microvascular surgery for revascularisation, replantation and composite tissue transfers.
Hand has derived its arterial supply, from two anastomotic arches, superficial and deep palmar arches which are formed between two main arteries of forearm i.e. radial, ulnar and their branches, in the palm.
The Vascular patterns of the palmar arches and their interconnecting branches present a complex and challenging study. Many attempts have been made to classify these variations. One of the first reports that presented a classification of palmar arches was the classic work of Coleman and Anson [1].
The superficial palmar arch is an anastomosis fed mainly by the ulnar artery. The later enters the palm with the ulnar nerve, anterior to the flexor retinaculum and lateral to the pisiform. It passes medial to the hook of the hamates, and then curves laterally to form an arch, convex distally and level with a transverse line through the distal border of the fully extended pollicial base. About a third of the superficial palmar arches are formed by the ulnar alone; a further third are completed by the superficial palmar branch of the radial artery and a third by the arteria radialis indicis, a branch of arteria princeps pollicis or the median artery. The superficial palmar arch is covered by palmaris brevis and the palmar aponeurosis and it is superficial to flexor digiti minimi, branches of the median nerve and to the long flexor tendons and lumbricals [2].
Classification of superficial palmar arch has been put forth by many researchers. Few to be noted are as follows.
Adachi 1928 [3], has described types of superficial palmar arches under three broad categories depending on the arteries contributing.
Huber 1930 [4], groups the superficial palmar arch into two classes, arches where in participating arteries form a complete arch (show anastomoses) and those that form incomplete arch (fail to anatomose).
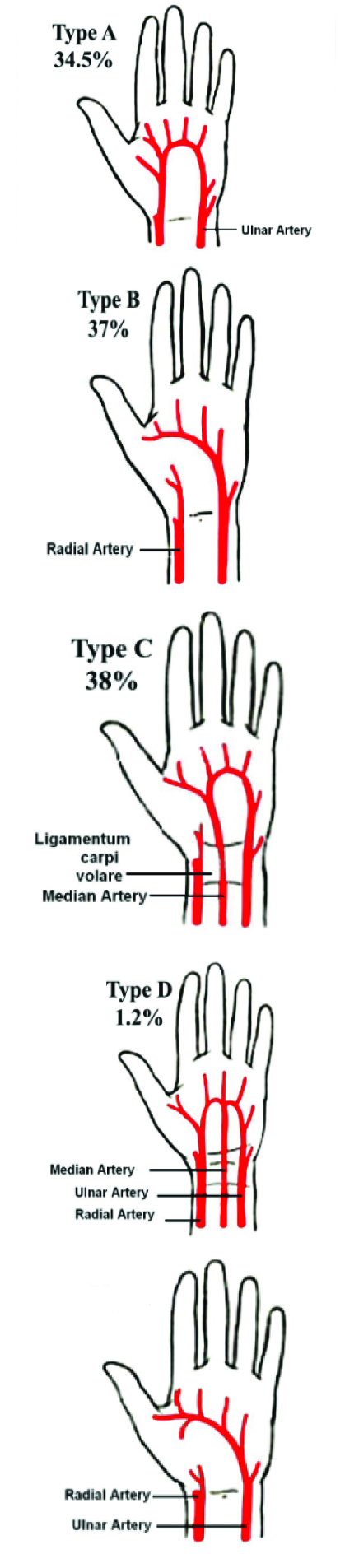
Coleman and Anson 1961 [1], Classified the superficial palmar arch in two groups, Group I and Group II as follows.
Group I Complete Arch: Contributing vessels anastomose with each other which are further divided into five types.
GroupII Incomplete Arch: Contributing vessels do not anastomose with each other which are further divided into four types that is, A, B, C, D similar to Group I (except Type E which has no representation in Group II) Refer [Table/Fig-1].
The superficial palmar arch classification by Coleman and Anson
Recent progress in hand surgery has engendered a need for precise knowledge of the frequency of anatomical variations in the superficial palmar arches [5].
Aims and Objectives
The present work was proposed to study the morphology of superficial palmar arch and variation in its formation.
Materials and Methods
The material for present study comprised of 100 upper limbs from 50 cadavers procured from the department of Anatomy of Dr. D.Y. Patil Medical College, Pimpri, Pune and B.J. Medical College, Pune. These cadavers were embalmed with 10% formalin and fixed. Palmar arches in them were dissected following classical incisions and dissection procedures of Cunninghams’ manual .
Variations from the normal classical pattern were observed. The observations were then recorded in a performa based on Adachi’s and Coleman and Anson classification of superficial palmar arches.
Observations
According to Adachi in Keen, [6] there are three types of superficial palmar arches as follows and their percentage recorded in present study have been denoted in the bracket.
Ulnar type: Minimum or absent contribution of the radial artery (66 percent) refer [Table/Fig-2].
Radio-ulnar type: (30%) refer [Table/Fig-3,4and5].
Median-ulnar type: Median artery is strong enough to irrigate the palm of the hand and to be part of the arch (4%) refer [Table/Fig-6].
Median-radial: Very rare type of superficial palmar arch, where the median artery anatomises with the radial artery, has a minimum or absent contribution of the ulnar artery.
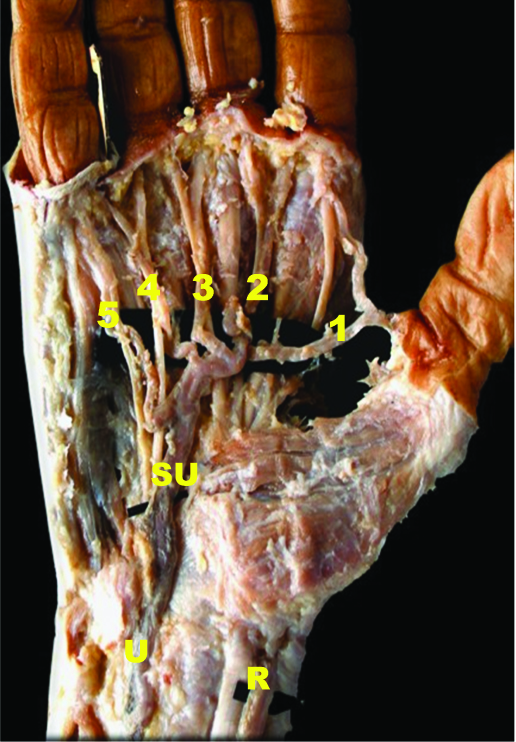
Shows complete arch-Group I Type B (ulnar) in left hand
Shows complete arch (Group I) – Type E in right hand where in the arch is completed on the lateral side by DMCA (refer Table/Fig-4])
R - Radial artery
U - Ulnar artery
SU - Superficial palmar branch of ulnar
1 to 5 - Digital arteries
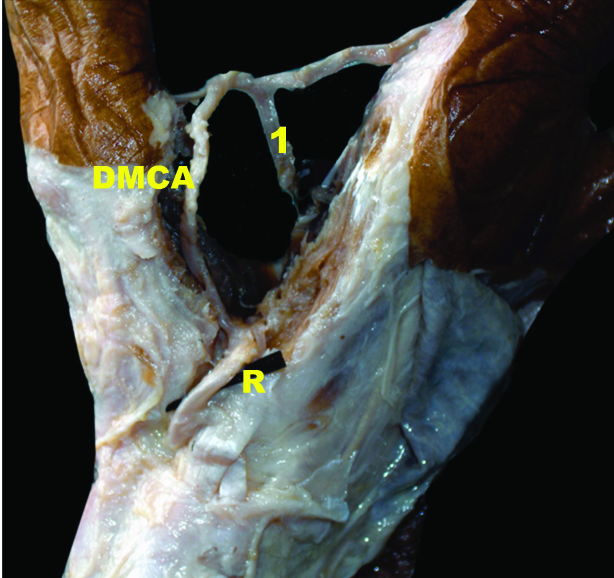
Shows that the superficial complete palmar arch (Group I) Type E is completed on the lateral side by DMCA in right hand (dorsolateral view)
DMCA - 1st dorsal metacarpal artery
R - Radial artery
1 - 1st common palmar digital artery
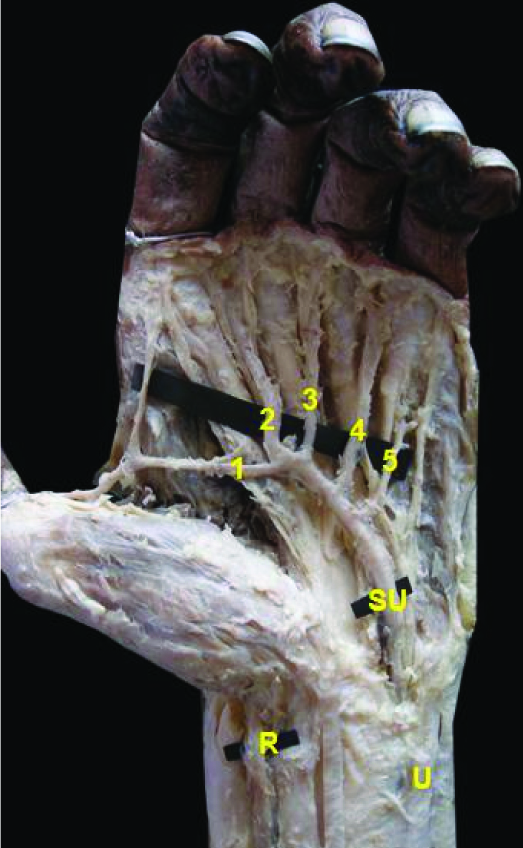
Shows the classical arch complete (Group I) – Type A
R - Radial artery
SR - Superficial palmar branch of radial artery
U - Ulnar artery
SU - Superficial palmar branch of ulnar artery
1 to 5 - Digital arteries

Shows mediano – ulnar arch that is incomplete arch (group II) type C
U - Ulnar artery
M - Median artery
SU - Superficial palmar branch of ulnar
1 to 5 - Digital arteries

According to Coleman and Anson 1961, [1] classification Complete superficial palmar arches [Group I] were observed to be 82 percent and Incomplete superficial palmar arches [Group II] were 18 percent in present study.
Percentage distribution of different types of superficial palmar arches according to Coleman and Anson’s classification, 1961 [1] is shown in [Table/Fig-1].
Discussion
Researchers which followed the broader way of Adachi [5] classification are Keen [6], Karlsson and Niechajev [7], Sílvia Regina Arruda de Moraes et al., [8]. Comparison with their work indicates that the present study coincides with them except, the work of Sílvia Regina Arruda de Moraes et al., [8], refer [Table/Fig-7].
Showing the classification of superficial palmar arches according to Coleman and Anson, 1961 with the percentage of samples observed in present study in brackets
| Group | Types according to Coleman and Anson [1] |
|---|
| A | B | C | D | E |
|---|
| Complete Arch (I) (contributing vessels anastomose) | Superficial palmar branch of radial artery + larger ulnar artery (4%) [Table/Fig-5] | Entirely by ulnar artery (56%) [Table/Fig-2] | Ulnar artery + enlarged median artery. | Radio-mediano-ulnar arch | Ulnar artery + large sized vessel derived from deep arch. (22%) [Table/Fig-3,4] |
| Incomplete Arch (II) (contributing vessels do not anastomose) | Superficial palmar branch of the radial artery + ulnar artery. (4%) | Ulnar artery only (does not supply the thumb and the index finger). (10%) | Superficial vessels of median + ulnar arteries. (4%) [Table/Fig-6] | Superficial vessels of Radial + median + ulnar arteries. | - |
Comparison with work of researchers like Ikeda et al., [9], Patnaik et al., [10], M. Chimmalgi et al., [11], Bilge O [12], Tagil [13], Madhyastha S. [14], Umapathy Sembian et al., [15], which followed Coleman and Anson’s [1] classification of palmar arterial arches indicates that the classical palmar arch, that is Group I (Type A) of Superficial Palmar Arch is having a higher incidence. This was not in correlation with present study where in the predominant pattern was observed to be of Group I (Type B) only ulnar type, refer [Table/Fig-8].
Shows comparsion between workers which followed Adachi’s, 1928 classification
| Sr. No. | Type | Adachi [5] | Keen [7] | Karlsson and Niechajev [8] | Sílvia Regina Arruda de Moraes et al., [9] | Present Study 2013 |
|---|
| 1 | Ulnar type | 59% | 59% | 64% | 23.34% | 66% |
| 2 | Radio-ulnar type | 32% | 32% | 32% | 63.33% | 30% |
| 3 | Mediano-ulnar type | 9% | 9% | 4% | 13.33% | 4% |
Double superficial palmar arch was not reported in present study.
High incidence of Group I (Complete arch) 82% signifies collateral circulation in hand [Table/Fig-9].
Studies which followed Coleman and Anson,1961 classification of superficial palmar arches.
| Sr. No. | Features | Colemen & Anson [1] | Ikeda et al., | Patnaik et al., Study[24] | M. Chimmalgi et al., | Bilge O | Tagil | Madhyastha S. et al., | Umapathy Sembian et al., | Present Study 2013 |
|---|
| Sample size | 650 | 220 | 50 | - | 50 | 20 | 48 | 50 | 100 |
| 1 | Group I | 78.5% | 96.4% | 78.0% | 88% | 86% | 75% | | 78.5% | 82% |
| Type A | 34.5% | 55.9% | 76.0% | 46% | 34% | 40% | 93.75% | 37.5 | 4% |
| Type B | 37.0% | 25.5% | 2.0% | 26% | - | 35% | 2.08% | 37 | 56% |
| Type C | 3.8% | - | - | 8% | - | - | | 3.8 | - |
| Type D | 1.2% | - | - | 2% | - | - | | 1.2 | - |
| Type E | 2.0% | - | - | 6% | - | - | | 2 | 22% |
| 2 | Group II | 21.5% | 3.6% | 16.0% | 12% | 14% | 25% | | 21.5 | 18% |
| Type A | 3.2% | - | 12.0% | 4% | - | - | 2.08 | 3.2 | 4% |
| Type B | 13.4% | - | - | 2% | - | - | | 13.4 | 10% |
| Type C | 3.8% | - | 4.0% | 4% | - | - | | 3.8 | 4% |
| Type D | 0% | - | - | 2% | - | - | | 1.1 | |
| 3 | Total | 100.0% | - | 94.0%* | 100% | - | - | 97.91† | 100 | 100% |
* In the rest of 6% the superficial palmar arch was double.
† In the remaining 2.09% the superficial palmar arch was a variant of classical arch
Some authors like Ozkus et al., [16] have also reported absence of superficial palmar arch but such a scenario is quite a rare finding which suggests that the superficial palmar arch is always present.
The present study predominantly shows complete type of superficial palmar arches which is in correlation with studies of Mozersky et al., [17] Higgins and Hayden [18] (On acronecrosed hands) Al Turk and Metcalf [19] except the works of Lippert H [20] and Mc Minn and Hutchings [21].
Persisting median artery is known to take part in the supply of the hand participating in the formation of superficial palmar arch. In the present study 4% showed mediano-ulnar type of incomplete arch. Jaschtschinsky [22] called this an atavistic characteristic because the median artery is normally round in the palmar arch of certain lower animals. Singer [23] describes the persistence of median artery to be due to cessation of development at fourth stage as described by him.
The presence of persisting median artery is not bilateral in the present study. It is likely that, the factors responsible for these variations could be acting unilaterally.
Ottone N. E, et al., [24] had their unique way of classification into arch and non arch pattern The Existing Arch Type, corresponding to the presence of a proper arch, is found in 58.0 percent of cases. The Non-Arch type was found with a significant frequency, in 42.0 percent of cases. The most commonly found pattern of the superficial palmar arterial system is the ulnar one, in 44.1% of cases. This pattern can be defined as the “normal” disposition. Coleman & Anson found [1] this pattern in 37% dominantly which is also in correlation with present study (56%).
Conclusion
The findings suggest that majority of hands showed complete arch which implies that collateral circulation is present in majority of cases. This would result in least number of complications considering radial artery harvesting for coronary bypass.
In the present study four specimens showed unilateral presentation of mediano-ulnar type of incomplete superficial arch. Thus in such cases radial artery harvesting for coronary artery bypass may prove to be less fatal.
It is interesting to note that many authors have tried to explore the anatomy and morphology of the superficial Palmar arches and very few have reported similar results and percentages. Ethnic and gender differences, sample size and different classification, interpretation could be some of the reasons that the results are not uniform. However, it is important to note that this study is representative of a small subset of the human population, and only serves to illustrate the many variations in the anatomy of the palmar arch.
* In the rest of 6% the superficial palmar arch was double.
† In the remaining 2.09% the superficial palmar arch was a variant of classical arch
[1]. Coleman SS, Anson BJ, Arterial patterns in the hand based upon a study of 650 specimensSurgery Gynaecology and Obstetrics 1961 113:409-24. [Google Scholar]
[2]. Gray’s Anatomy: The anatomical basis of clinical practice, wrist and hand 2006 39th edSusan Standring LondonElsevier Churchill Livingstone:926-31. [Google Scholar]
[3]. Adachi B, Das arterien-systemder Japaner, KenkyushaKoyoto 1928 1:365:368:389 [Google Scholar]
[4]. Huber GC, Piersol’s Human Anatomy: the vascular system 1930 Vol 19th edPhiladelphiaJ B Lippincott Co.:767-91. [Google Scholar]
[5]. Jelicic N, Gajisin S, Zbrodowski A, Arcus Palmaris SuperficialisActa Anat 1988 32:187-90. [Google Scholar]
[6]. Keen JA, Study of arterial variations in the limbs, with the reference to simetry of vascular patternAmerican journal of anatomy 1961 108:245-61. [Google Scholar]
[7]. Karlsson S, Niechajev IA, Arterial anatomy of the upper extremityActa Radiologica Diagnosis 1982 23:115-21. [Google Scholar]
[8]. Sílvia Regina Arruda de Moraes, Tâmara Nunes de Araújo, Alexandre Roque da Silva, Amanda Rodrigues de Paula, Juliana Larocerie Salgado, Morphologic variations of the superficial palmar arcActa Cirurgica Brasileira São Paulo 2003 18(3) [Google Scholar]
[9]. Ikeda Ugava Kazihara Hamada Arterial patterns in the hand based on a three-dimensional analysis of 220 cadaver handsAm Journal of Hand Surgery 1988 13(4):501-09. [Google Scholar]
[10]. Patnaik VVG, Kalsey G, Singla Rajan K, Palmar arterial arches - A morphological studyJournal of Anatomical society of India 2002 51(2):7-12. [Google Scholar]
[11]. Chimmalgi M, Sant SM, Chhibber SR, Humbarwadi RS, A study of superficial and deep palmar arches in human handsAnatomica Karnataka 2004 1(5):90-97. [Google Scholar]
[12]. Bilge O, Pinar Y, Ozer MA, Govsa F, A morphometric study on the superficial palmar arch of the handSurg Radiol Anat 2006 28(4):343-50. [Google Scholar]
[13]. Süleyman Murat Tagýl, Aynur Emine Çiçekcibaþý, Tunç Cevat Ögün, Mustafa Büyükmumcu, Ahmet Salbacak, Variations and Clinical Importance of the Superficial Palmar ArchSDÜ Týp Fak Derg 2007 14(2):11-16. [Google Scholar]
[14]. Madhyastha S, Murlimanju BV, Jiji PJ, Saralaya VV, Rai A, Vadgaonkar R, orphological variants of the human superficial palmar arch and their clinical implicationsJ. Morphol. Sci 2011 28(4):261-64. [Google Scholar]
[15]. Umapathy Sembian, Kamala E, Muhil M, Nalina Kumari, A Study of variations in the formation of superficial palmar arch in the rural population of southern tamilnaduInternational Journal of Anatomy Radiology and Surgery 2012-June Vol-1(1):7-11. [Google Scholar]
[16]. Ozkus K, Pestelmaci T, Soyluoglu AI, Akkin SM, Ozkus HI, Variations of the superficial palmar archFolia Morphol [Warsz] 1998 57(3):251-55. [Google Scholar]
[17]. Mozersky DJ, Bucklery CJ, Hazord CO Jr, Capps WF Jr, Dannemiller FJ Jr, Ultrasonic evalution of Palmar Circulation: A useful adjunct to Radial artery cannulationAmerican J of Surg 1973 126:810-12. [Google Scholar]
[18]. Higgins CB, Hayden WG, Palmar arteriography in acronecrosisRadiology [United States] 1976 119(1):85-90. [Google Scholar]
[19]. Al Turk M, Metcalf WK, A study of the superficial palmar arteries using the Doppler ultrasonic FlowmeterJ Anat [England] 1984 138:27-32. [Google Scholar]
[20]. Lippert H, Variability of hand and foot arteriesHandchir Plast Chir [German West] 1984 16(4):254-58. [Google Scholar]
[21]. Mc Minn RMH, Hutchings Colour Atlas of Human Anatomy 1988 2nd edChicagoBook Publishers:133 [Google Scholar]
[22]. Jaschtschinski SN, Morphologie and Topograohie des Arcus Volaris Sublimis und ProfundusAnat Hefte 1897 7:163-88. [Google Scholar]
[23]. Singer E, Embryological patterns persisting in the arteries of the armAnatomical record 1933 55:406-13. [Google Scholar]
[24]. Ottone NE, Prum N, Dominguez M, Blasi E, Medan C, Shinzato S, Analysis and clinical importance of superficial arterial palmar irrigation and its variants over 86 casesInt. J. Morphol 2010 28(1):157-64. [Google Scholar]