Sphenoid sinus (SS) is most inaccessible paranasal sinus. It has got importance due to trans-sphenoid approach to the pituitary gland [1]. It is surrounded by internal carotid artery, optic nerve, maxillary nerve and vidian nerve. Injury to these structures gives rise to inevitable complications [2]. This study is an attempt to know the percentage to variations in North Karnataka population, through endoscopic and gross cadaveric dissection and CT scan study.
Most of the complications are due to wide variation in anatomy of sphenoid sinus like extent of pneumatisation, termination of inter-sinus septa, accessory septae and its termination, presence of onodi cells and protrusion or dehiscence of neuro-vascular structures into the sphenoid sinus [3].
Materials and Methods
Endoscopic examination of SS was carried out in 30 cadavers (3 females and 27 males) using 0°, 30°, 70° rigid endoscopes. In all cadavers, ostium of the sinus was located and the sinus was entered trans- nasally through its anterior wall. All areas of sphenoid sinus were explored and pertinent findings were recorded [4]. Sections were then made in the sagittal plane to confirm the anatomical findings and to take necessary measurements with millimeter strips. The size of SS was measured by drilling a hole in its roof and the sinus was filled with fluid, using a syringe, after occluding the ostium of the sinus with dental wax [5]. The volume of the fluid that completely filled the sinus was indication of the size of the sinus.
CT scan of 30 living subjects (16 females and 14 males) was taken in coronal, sagittal and axial planes. Contiguous slice CT technique was used with 2 mm section thickness. We studied the type of pneumatisation, protrusion or dehiscence of neurovascular structures, presence of accessory septa or crest and its attachment, termination of inter-sinus septa, etc. We also took various measurements of the SS.
Patients with previous sinus surgery and patients with sphenoid sinusitis were excluded from study.
Mean and standard deviation was calculated for each reading. p-value was calculated for CT scan measurements. Unpaired ‘t’ test was used to calculate the p-value.
Result
Endoscopic and gross anatomical findings: - We studied 30 cadavers; 27 male and three female. Our results are as follows:
The sinus ostium – The sphenoid sinus opens into the spheno-ethmoid recess near the midline. The ostia were oval or rounded. We found 32 rounded and 28 oval shaped ostia.
Types of sphenoid sinus – The sphenoid sinuses have been classified into conchal, pre-sellar, sellar and post-sellar types according to the extent of their posterior limits. Conchal type of sphenoid sinus was absent [Table/Fig-1].
The types of sphenoid sinus.
| Type | No. | Percent |
|---|
| Pre-sellar | 6 | 20 Percent |
| Sellar | 4 | 14 Percent |
| Post-sellar | 20 | 66 Percent |
| Total | 30 | 100 Percent |
Accessory septa and crests – Bony septa or crests were seen in 13 cadavers, out of which in four cadavers (32 Percent) they were bilateral and in remaining nine cadavers (69 Percent) they were unilateral. The septa terminated on internal carotid artery (ICA) in seven cadavers while in two cadavers they terminated on optic nerve (ON).
Inter-sinus septa – In 22 cadavers inter-sinus septum terminated at a site other than normal. In eight cadavers it terminated over ICA and in three cadavers it terminated on ON. In rest of the cadavers it terminated away from the midline. Insertion of septum away from the midline gives rise to right or left dominance.
Sphenoid dominance – In 14 cadavers we found right dominance and in eight cadavers left dominance.
Dimensions of sphenoid sinus – Dimensions of the sphenoid sinus were as shown in [Table/Fig-2].
Dimension of sphenoid sinus on gross cadaveric dissection.
| Dimension (cm) | Right | Left |
|---|
| Mean ± SD | Mean ± SD |
|---|
| Transverse | 2.2 ± 0.5 | 1.8 ± 0.4 |
| Antero-posterior | 2.5 ± 0.5 | 2.4 ± 0.6 |
| Vertical | 2.3 ± 0.6 | 2.1 ± 0.5 |
Size of sphenoid sinus – The average size of sphenoid sinus was as shown in [Table/Fig-3].
Volume of sphenoid sinus.
| Type | Average volume (ml) |
|---|
| Pre-sellar | 2.2 |
| Sellar | 8.2 |
| Post-sellar | 9.4 |
Relations of sphenoid sinus – The cavernous part of the carotid artery frequently indents the lateral wall of the sinus producing a ‘carotid prominence’. This bulge we found in eight sinuses. The optic nerve is closely related to sphenoid sinus and it produces recognisable supero-lateral ridge. We found it identifiable in three sinuses [Table/Fig-4].
Dimensions of sphenoid sinus on CT scan examination.
| Dimension (cm) | Male (Mean ± SD) | Female (Mean ± SD) | t-value | DF | p-value |
|---|
| Antero-posterior Right | 2.7 ± 0.42 | 2.7 ± 0.53 | t = 0 | DF = 28 | p = 1 |
| Antero-posterior Left | 1.9 ± 0.76 | 2.7 ± 0.55 | t = 3.332 | DF = 27 | p < 0.005 |
| Transverse Right | 2.2 ± 0.53 | 2.1 ± 0.62 | t = 0.460 | DF = 28 | p > 0.05 |
| Transverse Left | 1.7 ± 0.56 | 2.1 ± 0.54 | t = 1.989 | DF = 27 | p > 0.05 |
| Vertical Right | 2.4 ± 0.33 | 2.3 ± 0.43 | t = 0.689 | DF = 27 | p > 0.05 |
| Vertical Left | 2.1 ± 0.61 | 2.2 ± 0.43 | t = 0.524 | DF = 28 | p > 0.05 |
CT Scan Findings
We studied 30 CT scans of sphenoid sinus (14 male and 16 female).
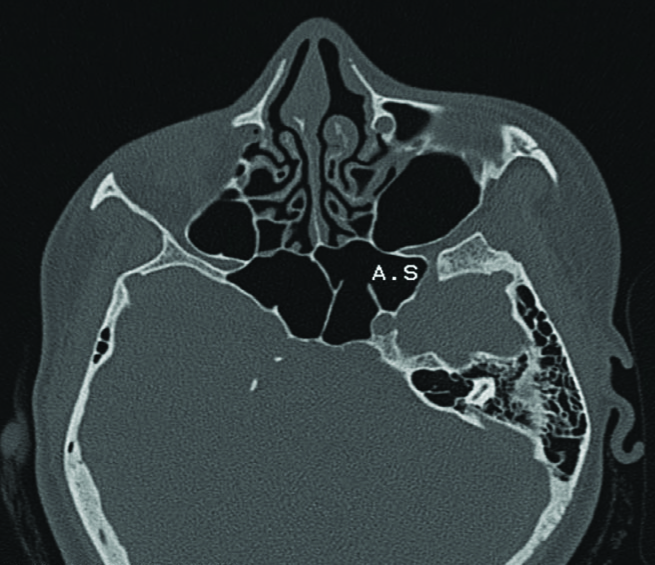
Accessory septa and its termination – Accessory septa were observed in 11 sinuses, multiple in 4 sinuses. In six sinuses these septa terminated over lateral wall of sinuses while in four sinuses they terminated over bony wall covering ICA and in one sinus on ON [Table/Fig-5].
CT scan showing accessory septum (AS) ending on internal carotid artery.
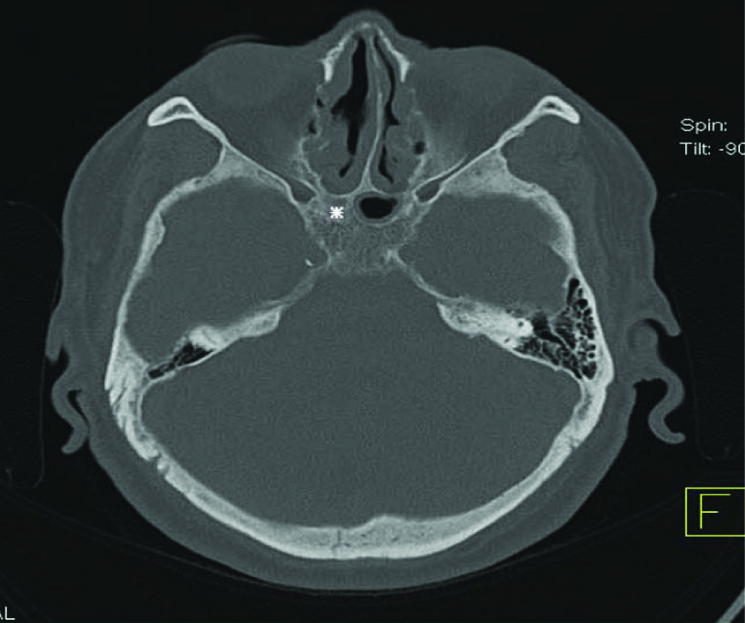
Termination of inter-sinus septum [Table/Fig-6] – In CT scan we found midline inter-sinus septum in 29 Percent of cases, in 20 Percent of cases it terminated on the bony wall covering the internal carotid artery and in 10 Percent of cases on bony wall covering optic nerve.
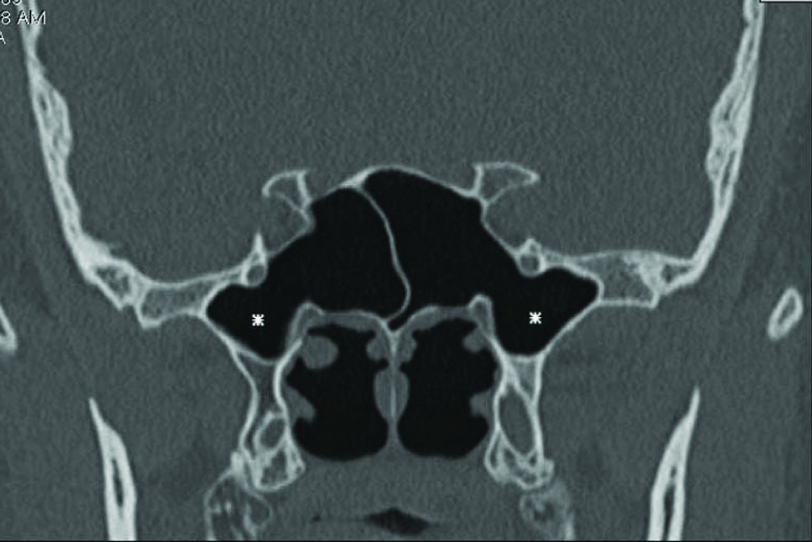
CT scan showing right conchal (*) type of pneumatization.
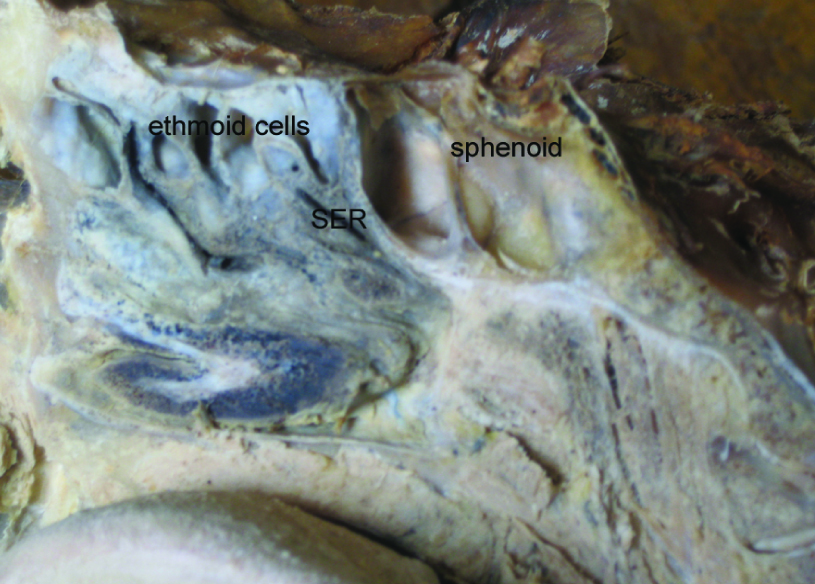
Extent of sphenoid sinus pneumatisation – Out of 60 sinuses, pre-sellar (8), sellar (14) and post-sellar (37) and in one subject right side sinus was conchal [Table/Fig-4]. Pneumatisation of greater wing of sphenoid was observed in two sinuses, of pterygoid process in four sinuses and of clinoid process in two sinuses [Table/Fig-7]. We also found onodi cell in one sinus [Table/Fig-8].
Relations of sphenoid sinus and spheno-ethmoid recess (SER).
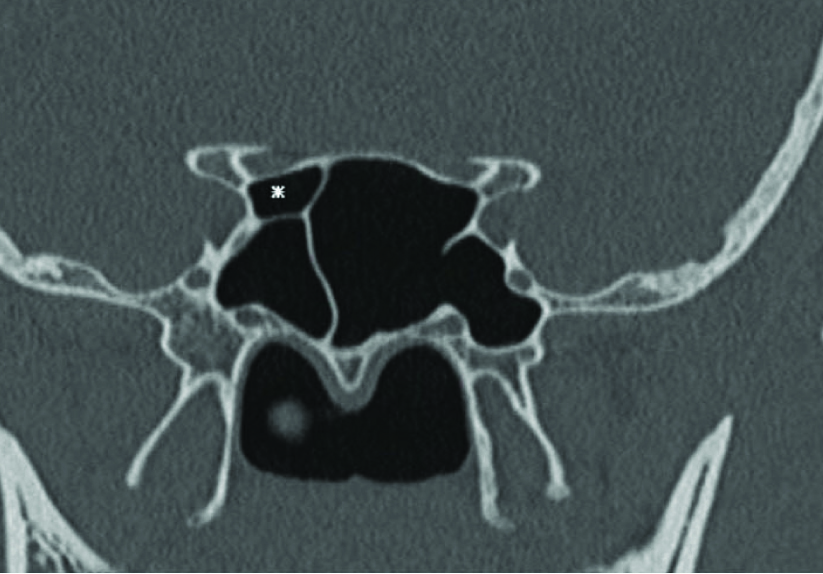
CT scan showing left sphenoid dominance and Onodi cell (*).
Dimensions of sphenoid sinus – All dimensions were recorded and ‘p’ value calculated for each dimension. ‘p’ value was significant for right side AP dimension. Un-paired ‘t’ test was used to assess the significance of correlation [Table/Fig-6].
Sphenoid dominance – Right dominance was observed in 20 persons while left dominance in 10 persons.
Relations of sphenoid sinus – Protrusion of ICA were observed in nine sinuses. Protrusion of optic nerve was observed in two sinuses. Protrusion of maxillary nerve and vidian nerve were observed in three sinuses. Dehiscent bony wall was absent. Onodi cells were observed in 1 sinus.
Discussion
The concept of normal sphenoid sinuses includes two symmetrical cavities with smooth walls and capacity of 5-7 ml, separated by a straight mid-line partition which does not encroach on any of the surrounding structures, and which in turn is not encroached upon by these elements [1].
Shape of sphenoid ostium
A pin head size sphenoid ostium was noted in 15 Percent of the material studied by Lang [3]. Shape of sphenoid sinus ostium can be round or oval. S. Elwany et al., [1] observed round ostia in 72 Percent of material and oval in 28 Percent of material. D. Sethi et al., [4] found round ostia in 47 Percent of cases and oval ostia in 40 Percent of cases. In our study we found round ostia in 53 Percent of cases and oval in 46 Percent of cases in cadavers [Table/Fig-9 and 7].
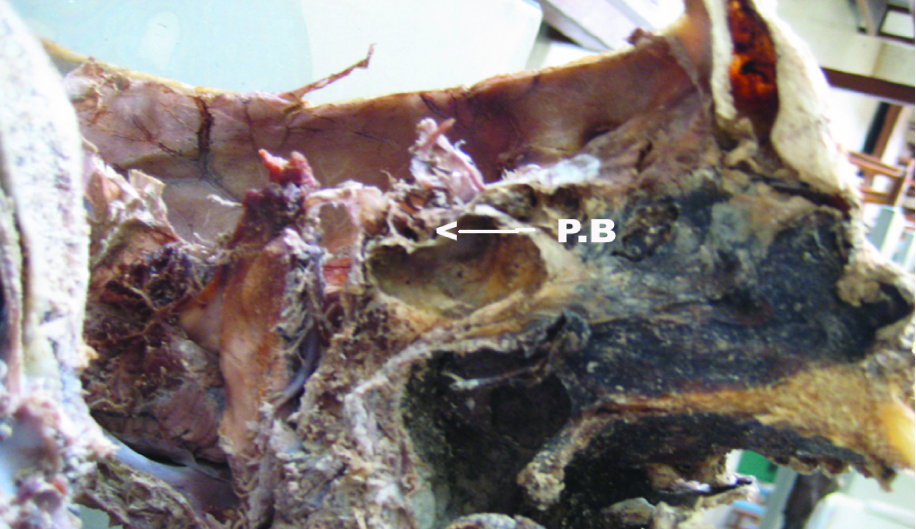
Post-sellar sinus with pituitary bulge (P.B.).
Type of sphenoid sinus
The reasons for wide variation in the size of the sphenoid sinus are controversial. Pneumatisation of the sphenoid bone is a function of the sub-epithelial layer of the sphenoid sinus mucosa. If due to local infection or malfunction of the endocrine glands, the pneumatising function of this layer is impaired, then an abnormality of the sinus will develop on one or both sides.
In our cadaveric study, we found 66 Percent post-sellar, 20 Percent pre-sellar and 14 Percent sellar type of pneumatisation [Table/Fig-1]. Conchal type of pneumatisation was absent. S Elwany et al., [2] observed 30 Percent pre-sellar, 71 Percent post-sellar type of pneumatisation. In another study done by D Sethi et al., [4] they observed pre-sellar in 27 Percent and post-sellar in 73 Percent of sinuses. Sareen D et al., [5] found pre-sellar in 25 Percent and post-sellar in 75 Percent of sinuses. Renn and Rhoton [6] also have same findings. They found pre-sellar in 32 Percent and post-sellar in 68 Percent of sinuses.
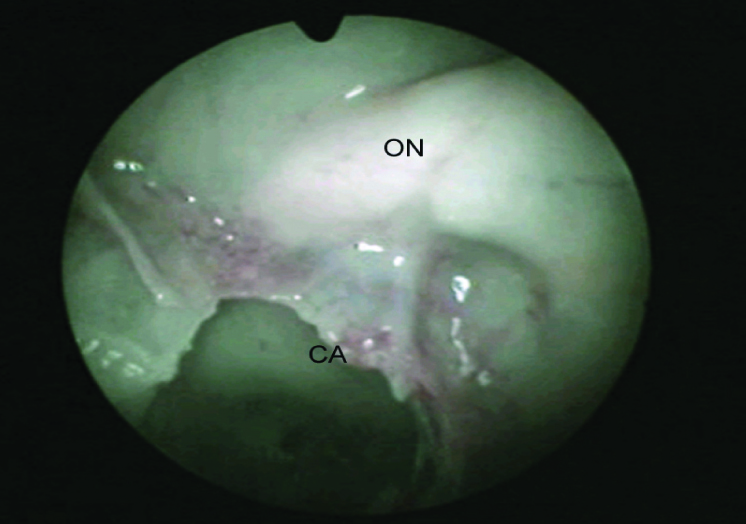
Endoscopic view showing Optic nerve (ON) and Carotid artery (CA) bulge.
Sphenoid sinus of the post-sellar type offers optimum conditions for trans-sphenoid hypophysectomy, namely; roomy sinuses, thin anterior wall and floor of sella turcica [7]. On the other hand, sphenoid sinus of the pre-sellar type frequently presents difficulties during hypophysectomy, and when the sinus is of conchal type the operation is strongly contra-indicated. However with the surgeon informed in advance, different tools can make such an approach feasible [8].
Accessory septae and its termination – Bone formed at the line of fusion of bony nuclei is denser than the bone immediately adjacent to it, and, therefore, it is more resistant to pneumatisation. This fact explains the occurrence of partial septa in, and the various forms assumed by them, in the sphenoid sinus.
In our study, we found accessory septa in 13 cadavers (43 Percent). In seven cadavers (23 Percent) it terminated on internal carotid artery, in two cadavers (6 Percent) it terminated on optic nerve and in 4 cadavers (13 Percent) it terminated either over inter-sinus septum or on the lateral wall. S. Elwany et al., [2] observed accessory septa in 76 Percent of cases. Another study by S. Elwany et al., [1] found accessory septa in 68 Percent of cadavers. In 13 Percent of cadavers it terminated over internal carotid artery and in 6 Percent of cadavers it terminated over optic nerve. Sareen D et al., [5] found inter-sinus septae in 80 Percent of cases. Findings of our study are similar to other studies.
Inter-sinus septum – In our study we found termination of inter-sinus septa on bony wall covering internal carotid artery in seven cadavers (23 Percent), on bony wall covering optic nerve in three cadavers (10 Percent), in 10 Percent of the cadavers it was lying in the midline and in 80 Percent of the cadavers it was deviated on either side of the mid-line. S. Elwany et al., [2] found midline septum in 27 Percent of cases and in 73 Percent of cases it was deviated. D Sethi et al., [4] observed termination of inter-sinus septum onto the internal carotid artery in 40 Percent of cases while Renn and Rhoton [6] found it in 32 Percent of cases.
This means that the inter-sinus septum should never be used as a guide to the midline during hypophysectomy. The vomer can be used as a more accurate guide to the midline [7]. It is wise to use extreme caution while removing the terminal septum in order to prevent accidental injury to internal carotid artery or optic nerve [9].
Sphenoid dominance – In our cadaveric study we found right dominance in 16 cases (54 Percent) and in eight cases left dominance (27 Percent). D Sethi et al., observed right dominance in 27 Percent cases and left dominance in 33 Percent cases.
Dimensions of sphenoid sinus – In our study average dimensions of the sphenoid sinus were found to be: antero posterior - 2.5 cm, transverse - 2.1 cm and vertical - 2.2 cm. Average dimensions in the study by S. Elwany et al., [2] were antero posterior - 2.4 cm, transverse - 1.6 cm and vertical - 2 cm. Sareen D et al., [5] observed average dimensions in their study as follows: antero posterior - 2.5 cm, transverse - 2.8 cm and vertical - 2.2 cm.
Size of sphenoid sinus – If pneumatisation of the sinus is retarded on one side but unrestricted on other, then the mucosa of the unrestricted side encroaches over the bone of restricted portion during the process of bone absorption. This leads to disparity in size of the two sinuses.
In our study, the volume ranged between 2.2 to 9.4 ml. In other studies it ranged between 2.7 to 9.1 ml (S. Elwany et al.,) [2], 6 to 7.5 ml (Simpson et al.,) [10], 4 to 9 ml (Ballenger,) [11] and 3 to 10 ml (Sareen D et al.,) [5].
Relations of neuro-vascular structures - Pneumatisation of the sphenoid sinus was halted by the presence of softer materials such as cartilage, connective tissue or blood vessels. This explains variation in the relations of neuro-vascular structures.
S. Elwany et al., [1] observed protrusion of internal carotid artery in 18 Percent of cases and protrusion of optic nerve in 29 Percent of sinuses. They found onodi cell in 7.5 Percent of sinuses. D Sethi et al., [4] observed internal carotid artery bulge in 7 Percent of sinuses and dehiscent optic canal in 3 Percent of sinuses. They found onodi cell in 3 Percent of sinuses. Renn and Rhoton [6] reported protrusion of internal carotid artery in 71 Percent of sinuses and dehiscence in 4.8 Percent of sinuses. Kennedy et al., [12] reported dehiscence of internal carotid artery in 22 Percent of his reported cases. Fuji et al., [13] reported optic nerve bulge in 40 Percent of his specimens. In our study we found protrusion of internal carotid artery in 25 Percent of sinuses and optic nerve bulge in 10 Percent of sinuses in cadavers. Wide variations in the findings were because of multiple factors as no two studies matches with each other.
Findings in CT Scan Study
Accessory septae and their termination [Table/Fig-11] – In CT scan study we observed accessory septa in 11 cases (20 Percent) out of which in four cases they terminated on internal carotid artery (6.6 Percent) and in one case it terminated over optic nerve (1.6 Percent). In another study done by Ossama Hamid [14], they found accessory septa in 10.8 Percent of cases.
CT scan showing pneumatized pterygoid process (*).
Termination of inter-sinus septum [9] – In CT scan we found midline inter-sinus septum in 29 Percent of cases, in 20 Percent of cases it terminated on the bony wall covering the internal carotid artery and in 10 Percent of cases on bony wall covering optic nerve. Ossama Hamid et al., [14]observed that in 32 to 40 Percent of cases it deviated from the midline and terminated over the internal carotid artery.
Extent of sphenoid sinus pneumatisation [Table/Fig-6, 8 and 11] - In CT scan study, we observed one conchal (1.6 Percent), eight pre-sellar (14 Percent), 14 sellar (23 Percent) and 37 post-sellar (61 Percent) type of pneumatisation. In other study, Ossama Hamid et al., [14] observed 2 Percent conchal, 21 Percent pre-sellar, 54.7 Percent sellar and 22.3 Percent post-sellar type of pneumatisation. In our study we observed pneumatisation of anterior clinoid process in two cases (34 Percent), that of greater wing of sphenoid in two cases (34 Percent) and of pterygoid process in four cases (67 Percent). Hewaidi GH et al., [15] observed pneumatisation of anterior clinoid process in 15 Percent, of greater wing of sphenoid in 20 Percent and that of pterygoid process in 29 Percent of the patients. Bolger et al., [16] identified pneumatisation of anterior clinoid process in 13 Percent and of pterygoid process in 43 Percent patients. John Earwaker [17] found pneumatisation of greater wing of sphenoid in 20 Percent of patients. De Lano et al., [18] found anterior clinoid process pneumatisation in 4 Percent of patients. Sirikci et al.,[19] found anterior clinoid process pneumatisation in 29 Percent of patients. Birsen et al., [20] found anterior clinoid process pneumatisation in 24 Percent of patients.
Review of CT scan images for the presence of pneumatisation of anterior clinoid process, greater wing of sphenoid and pterygoid process are more sensitive than cadaveric dissection. Pterygoid process pneumatisation, when present, is an important pathway for access to the central skull base. These techniques may provide route for endoscopic repair of CSF leaks and endoscopic biopsy of skull base lesions [21].
Dimensions of sphenoid sinus – The mean and standard deviations of all dimensions for male and female were as shown in [Table/Fig-4]. We found statistically significant correlation for right antero-posterior dimension. Our findings were similar to studies done by others.
Sphenoid dominance [5] – In CT scan study we observed right dominance in 20 cases (66 Percent) and left dominance in 10 cases (33 Percent).
Relations of neuro-vascular structures [Table/Fig-6,8 and 11] – In CT scan study, we observed protrusion of internal carotid artery in 15 Percent, optic nerve in 33 Percent, vidian nerve in 5 Percent and maxillary nerve in 5 Percent of sinuses. In one case onodi cell was observed. Hewaidi GH et al., [15] in their CT scan study observed protrusion of internal carotid artery in 41 Percent of patients and dehiscence of the artery in 30 Percent. Protrusion of optic nerve was observed in 35.6 Percent and dehiscence in 30.6 Percent of patients. Maxillary nerve protrusion was observed in 24.3 Percent and dehiscence of the nerve in 13 Percent of patients. Vidian nerve protrusion was found in 27 Percent of patients. Fuji et al., [13] found 8 Percent dehiscent carotid arteries, 4 Percent dehiscent optic nerve. Kennedy et al., [12] found dehiscence of internal carotid artery in 25 Percent of patients. Birsen et al., [20] found protrusion of internal carotid artery in 30.3 Percent and dehiscence in 3.5 Percent of patients. They noticed protrusion of maxillary nerve in 24.3 Percent. Sirikci et al., [19] reported protrusion of internal carotid artery in 26.1 Percent of patients and dehiscence of the artery in 23 Percent. Lang and Keller [22] reported that the vidian canal was protruded into the sinus cavity in 18 Percent.
There is significant difference in the relations of surrounding neurovascular structures in our study as compared to other studies. These variations may be because of racial or regional difference.
Conclusion
Sphenoid sinus shows various types of pneumatisation, and when pneumatisation spreads outside the body of sphenoid sinus it creates various recesses. These place the sinus in close proximity to important structures like the maxillary nerve or the vidian nerve. Newer techniques are emerging for safety of patients due to complex and highly variable anatomy of the sphenoid sinus. Now intra-operative fluoroscopic imaging or intra-operative navigational devices are used to confirm surgical landmarks making these techniques very safe.