Small Intestine Ischaemia due to Volvulus during Pregnancy
Shantajit Nameirakpam1, Shangchungla Keishing2, Jaleshwar Laishram3, Ranita Devi S.4
1 Post Graduate Trainee, Department of Surgery, Regional Institute of Medical SciencesImphal, India.
2 Post Graduate Trainee, Department of Obstetrics and Gynaecology, Regional Institute of Medical SciencesImphal, India.
3 Registrar, Department of Surgery, Regional Institute of Medical SciencesImphal, India.
4 Associate Professor, Department of Surgery, RIMSImphal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shantajit Nameirakpam, Chingamakha Irom Leirak Singjamei, Imphal, West Manipur, India.
Phone: 7308161777,
E-mail: shantajit@gmail.com
Small intestine ischaemia caused by volvulus is difficult to diagnose during pregnancy, as the signs and symptoms may be masked by pregnancy. An early diagnosis and a prompt surgical intervention is necessary, as morbidity and mortality of this disorder are significant. We are presenting a case of a 35-year-old pregnant woman with volvulus of small bowel.
Small intestine volvulus, Gangrene, Jejuno-ileal anastomosis, Surgical acute abdomen
Case Report
A 35-year-old woman who was in 32nd week of gestation, presented to our Emergency Department with severe abdominal pain and nausea. The chief complaint was periumbilical pain of 2 days duration, which was colicky in nature, which spread to the whole of the abdomen. She also reported of constipation for 1 day and she vomited semisolid particles twice after her admission. On admission, her vitals were found to be not stable and her blood pressure was not recordable. On clinical examination, her abdomen was found to be diffusely tender, with a 32 week gravid uterus and no foetal activity, which were confirmed on doing an emergency ultrasound screening.
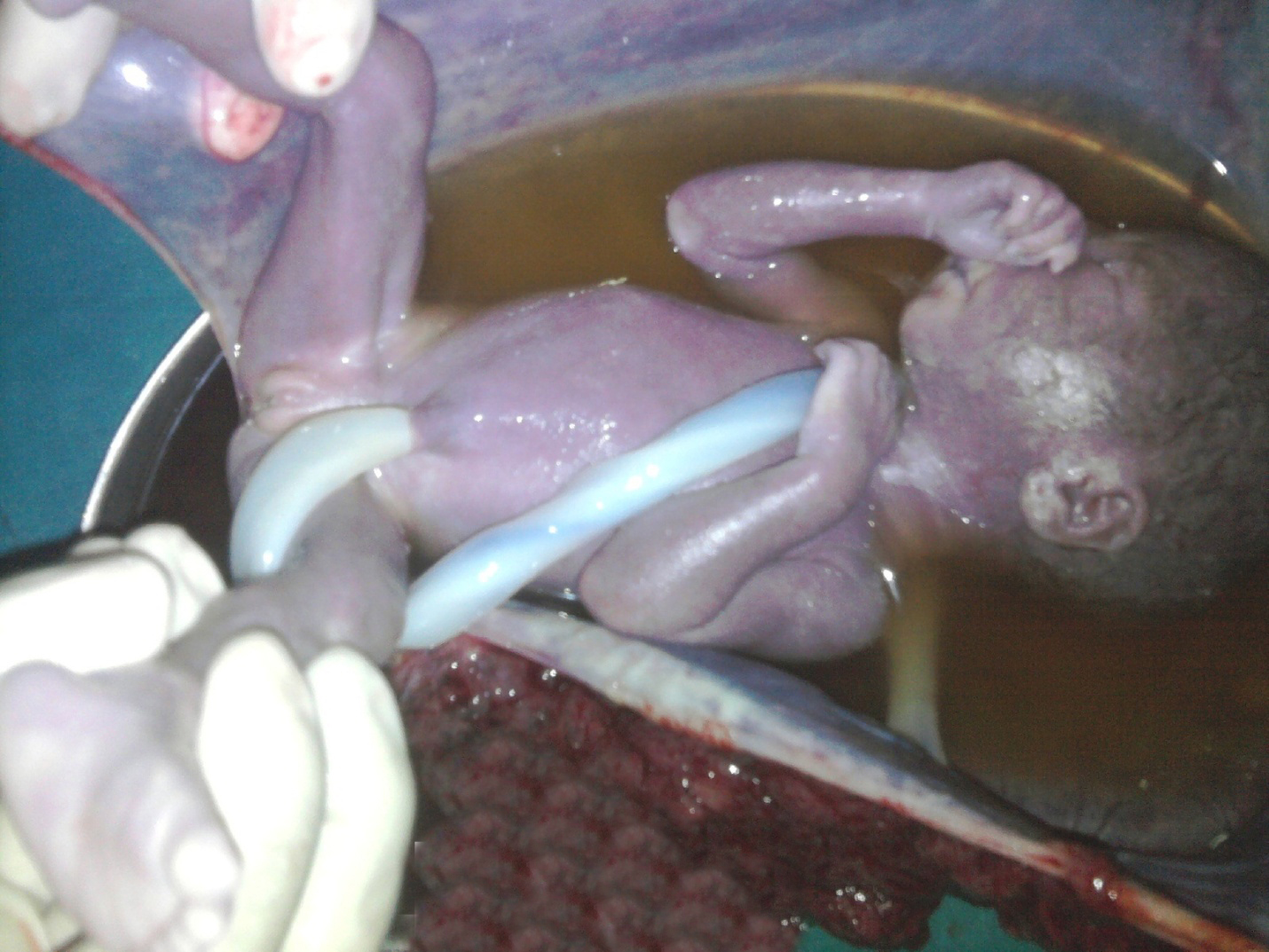
Laboratory investigations revealed increased blood urea nitrogen and creatinine levels. Patient was stabilized after giving adequate fluid and electrolyte therapy. An emergency laparotomy was done by making a midline incision. 200-300 ml of blood and clot were evacuated. A stillborn foetus was delivered .The death of the foetus was related to toxicity caused by volvulus and foetus was fresh dead at the time of surgery [Table/Fig-1]. A small intestine volvulus in anti clockwise direction, 60 cm from the Treitz ligament, which spared 10 cm of the terminal ileum, was seen. The bowel was dark and oedematous, which indicated gangrene [Table/Fig-2,3]. Resection of the gangrenous bowel and end to end jejunoileal anastomosis were done. The post-operative period was uneventful. The patient has been followed up in our Outpatients Department for the past 18 months and we have not found any features of short bowel syndrome.

Small bowel gangrene sparing 10cm of terminal ileum

Discussion
A surgically acute abdomen in pregnancy must be diagnosed early and accurately, as a prompt treatment is necessary, to prevent morbidity and mortality of the patient. It is difficult to diagnose an acute surgical abdomen in pregnancy, due to the increasing size of the uterus and the subsequent dislocations of the intra abdominal organs, high prevalence of hyperemesis gravidarum and abdominal pain in the normal obstetric population, lack of basic facilities for doing routine check ups in many rural areas of our country and awareness among the common people.
Bowel obstruction is the third most common cause of acute abdomen in pregnancy [1]. Adhesions, volvulus and intussusceptions are the major causes of intestinal obstructions in pregnancy [2]. Volvulus is the second most common cause of intestinal obstructions in pregnancy, occurring in up to 25% of cases, as compared to its involvement in only 3-5% in non-pregnant women [3].
Most cases of small bowel volvulus occur in the 3rd trimester or puerperium [4-6]. Making a pre-operative diagnosis is difficult, due to non-specific signs and symptoms, as it happened in our case. We went for a laparotomy on diagnosing it as a case of ruptured uterus with intrauterine death. It has been suggested that an increasing uterine size and its sudden decrease during puerperium may predispose to a small bowel volvulus [7, 8].
Conclusion
An early surgical intervention is necessary, to reduce gangrene and to decrease the morbidity and mortality of the patient. Less than fifteen cases of small bowel volvulus which occurred in pregnancy have been reported since the past two decades. It occurs mostly in the 3rd trimester and puerperium. A close co-operation between surgeons and obstetricians is required in such cases. A laparoscopic approach will be helpful in making a correct diagnosis and providing a prompt treatment.
[1]. Coleman MT, Trianfo VA, Rund DA, Nonobstetric emergencies in pregnancy:trauma and surgical conditionsAm J Obstet Gynecol 1997 177:497-502. [Google Scholar]
[2]. Damore LJ 2nd, Damore TH, Longo WE, Miller TA, Congenital intestinal malrotation causing gestational intestinal obstruction. A case reportJ Reprod Med 1997 42:805-08. [Google Scholar]
[3]. Gaikwad A, Ghongade D, Kittad P, Fatal midgut volvulus:a rare cause of gestational intestinal obstructionAbdominal Imaging 2010 35(3):288-90. [Google Scholar]
[4]. Huang JC, Shin JS, Huang YT, Chao CJ, Ho SC, Wu MJ, Small bowel volvulus among adultsJGastroenterol Hepatol 2005 20(12):1906-12. [Google Scholar]
[5]. Perdue PW, Johnson HW, Stafford PW, Intestinal obstruction complicating pregnancyAm J Surg 1992 164:384-88. [Google Scholar]
[6]. Sato N, Miki T, Toyonaga T, Konomi H, Ishimitsu T, Nagafuchi K, A case of herniation through a defect in the falciform ligament at latepregnancyNippon Geka Gakkai Zassh 1996 97(9):787-90. [Google Scholar]
[7]. Ventura-Braswell AM, Satin AJ, Higby K, Delayed diagnosis of bowel infarction secondary to maternal midgut volvulus at termObstet Gynecol 1998 91:808-10. [Google Scholar]
[8]. Mahdavi Atossa, Yunesi Nasim, Small bowel volvulus in a primigravida woman: Case reportJournal of Family and Reproductive Health Summer 2007 1(1):51-54. [Google Scholar]