A Comparison of Functional Outcomes After Metallic and Bioabsorbable Interference Screw Fixations in Arthroscopic ACL Reconstructions
Atmananda S Hegde1, Deepak K Rai2, Antony J Kannampilly3
1 Associate Professor, Department of Orthopaedics, Yenepoya Medical College, Mangalore, Karnataka, India.
2 Professor, Department of Orthopaedics, Yenepoya Medical College, Mangalore, Karnataka, India.
3 Junior Resident, Department of Orthopaedics, Yenepoya Medical College, Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Atmananda S. Hegde, 102, Dune Apartments, 1st Cross Road, Shivbagh, Mangalore-575002, Karnataka, India.
Phone: 09740557222,
E-mail: atmanandahegde@gmail.com
Introduction: Anterior Cruciate Ligament (ACL) is as one of the most frequently injured ligaments in the modern contact sports scenario. Graft fixations can be achieved during anterior cruciate ligament (ACL) reconstructions by using either bioabsorbable screws or metal screws. The objective of this study was to compare the functional outcomes after bioabsorbable and metallic interference screw fixations in arthroscopic anterior cruciate ligament reconstructions done by using hamstring grafts.
Materials and Methods: This was a prospective, randomized study. Patients in Group 1 received bioabsorbable interference screws and patients in Group 2 received metallic interference screws. Arthroscopic assisted, anterior cruciate ligament reconstructions with the use of hamstring grafts which were fixed proximally with endobuttons and distally with bioabsorbable or metallic interference screws, were undertaken. Progress in functional outcomes was assessed by using Mann Whitney U- test. Functional outcomes in the two groups were compared by using independent t-test.
Observation and Results: In each group, there were statistically significant improvements in functional outcomes over successive follow-ups, which were seen on basis on Mann-Whitney U-test. The comparison of functional outcomes between the two groups, done by using independent t-test, showed no statistically significant differences between the two groups at 3 months, 6 months and 1 year of follow-up. p-value <0.05 was considered to be significant in our study.
Conclusion: In our prospective study of comparison of functional outcomes between bioabsorbable and metallic interference screws in arthroscopic anterior cruciate ligament reconstructions, which were evaluated by using Tegner activity scale and Lysholm knee scoring scale for a period of 1 year, no statistically significant difference was found. However, further authentication is required by doing long term studies.
ACL reconstruction, Bioabsorbable and Metallic interference screws
Introduction
Anterior Cruciate Ligament (ACL) is as one of the most frequently injured ligaments in the modern contact sports scenario, which amounts to an estimated 1 in 3000 injuries in American population and approximating to 95,000 new injuries which are recorded each year [1]. This has also evoked as much controversy, thought and opinion, so as to understand as to how to optimally reconstruct an anterior cruciate ligament of the knee [2].
Many questions remain to be clarified on aspects which are related to optimal graft-fixation techniques and the properties of the materials which are used to fabricate the medical devices which are used in ACL reconstructions. Graft fixations can be achieved during anterior cruciate ligament (ACL) reconstructions with use of either bioabsorbable screws or metal screws. Over several years, fixations for ACL reconstructions have been performed by using metal interference screws [3]. This system proved to achieve strong initial fixation and to provide osseous integration in grafts with bony components [4]. However, several concerns have arisen as a consequence of its application in soft tissue grafts [5], for example, due to the risk of graft damage or of providing more fragile reconstructions. Bioabsorbable cannulated interference screws were introduced for arthroscopic ACL-reconstructions in the early 1990s [6, 7]. Polylactic acid is widely used as the main component in bioabsorbable screws. Different bioabsorbable screws are available, e.g. those with polyglycolic acid (PGA), polylactic acid (PLA), poly-l-lactic acid (PLLA), poly-d-lactic acid (PDLLA), and polyparadioxanone (PDS).
Although bioabsorbable screws and metal screws have similar fixation strengths, bioabsorbable screws eliminate the need for their removal. In addition, post-operative imaging is easier to interpret when bioabsorbable screws are used. Bioabsorbable screws may be associated with an increased inflammatory response, an increased risk of screw breakage, incomplete screw absorption, or tunnel widening [8]. Metal screws have been associated with adverse events, including MRI distortion and complications in revision surgery [4].
The objective of this study was to compare the functional outcomes after bioabsorbable and metallic interference screw fixations in arthroscopic anterior cruciate ligament reconstructions by using hamstring grafts.
Materials and Methods
This was a prospective, randomized study which included 24 patients, which was done to compare the functional outcomes between bioabsorbable and metallic interference screw fixations in arthroscopic ACL reconstructions .This study was conducted in our institution from August 2011 to July 2013. Ethical clearance was obtained from institutional ethical committee for conducting this study.
Patients who were diagnosed to have complete anterior cruciate ligament injuries (Grade 3), who were in the age group of 20 – 60 years, who were admitted to our hospital, were included in this study. Patients who were above 60 years and less than 20 years of age, patients with chronic ACL insufficiency with osteoarthritis and patients with collaterals and /or PCL injuries were excluded from this study.
Patients who came to our hospital with suspected anterior cruciate ligament tears were clinically evaluated by using various tests such as Lachman, anterior drawer, valgus / varus stress test, Mcmurray and posterior drawer tests. Further evaluation was done by taking radiographs and by doing MRI. Patients were explained about the procedures in detail, their outcomes and the rehabilitation programmes which they had to undergo. Patients were randomly put in two groups. Patients of Group 1 received bioabsorbable interference screws and patients of Group 2 received metallic interference screws. After getting written informed consents from the patients, arthroscopic assisted anterior cruciate ligament reconstructions with use of hamstring grafts which were fixed proximally with endobuttons and distally with bioabsorbable or metallic interference screws were undertaken.
Surgical technique involved multiple portal arthroscopic single bundle ACL reconstructions with use of quadrupled hamstring grafts which were harvested from the same side [Table/Fig-1]. In all patients, femoral fixations were achieved by using endobuttons and tibial fixations were achieved by using either metallic or bioabsorbable interference screws, based on their randomization [Table/Fig-2].
Intraoperative picture of arthroscopic ACL reconstruction using hamstring graft
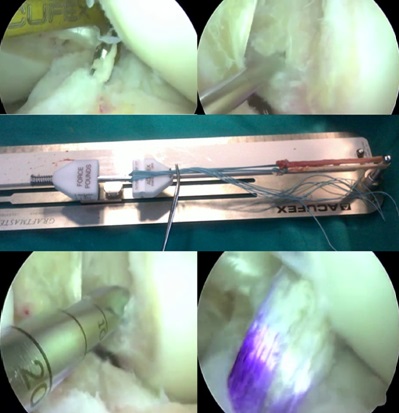
Radiographs showing metallic and bioabsorbable screws used in ACL reconstruction

Post-operatively, all patients underwent standardized rehabilitation protocols and they were regularly followed up. In addition to clinical and radiological evaluations, functional outcomes were assessed during the follow-up visits. Functional outcomes were assessed by using Lysholm score and Tegner activity level scale at 3 months, 6 months and 1 year of follow-up. Progress in functional outcome in each group was assessed by using Mann-Whitney U-test. Functional outcomes in the two groups were compared by using identity t- test. p-value of less than 0.05 was considered to be statistically significant.
Observation and Results
In this study, mean age of patients in Group 1 (bioabsorbable) was 25 years and that of patients in Group 2 (metallic) was 30.5 years. All the 24 patients were males. In Group 1, right knee was involved in 2/3rd of the cases, whereas in Group 2, left knee was involved in 2/3rd of the cases. Two patients in each of the two groups had additional lateral meniscal injuries, whereas 10 patients in Group 1 and 12 patients in Group 2 had additional medial meniscal injuries.
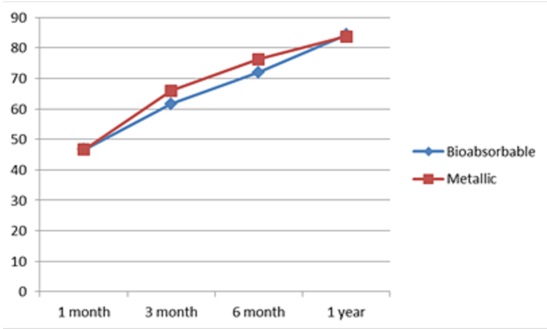
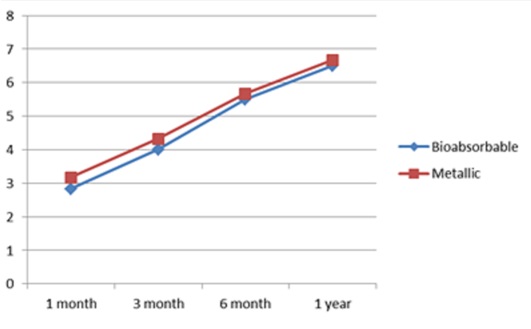
In Group 1, mean Lysholm knee scores at 3 months, 6 months and 1 year of follow-up were 61.67, 72 and 84.33 respectively and mean Tegner activity level scores at similar periods of follow-up were 4, 5.5 and 6.5 respectively. In Group 2, mean Lysholm knee scores at 3 months, 6 months and 1 year of follow-up were 61.67, 76.33 and 83.67 respectively and mean Tegner activity level scores at similar periods of follow-up were 4.33,5.67 and 6.67 respectively. Both the groups were comparable with respect to pre-operative variables with no statistically significant difference as assessed by chi-square tests.
In each group, there were statistically significant improvements in functional outcomes over successive follow-ups, which were seen on basis of Mann Whitney U-test. The comparison of functional outcomes between the two groups with use of independent t-test showed no statistically significant differences between the two groups at 3 months, 6 months and 1 year of follow-up [Table/Fig-3,4]. p-value <0.05 was considered to be significant in our study.
Comparison of Lysholm score between two groups during the follow-up
Comparison of Tegner activity score between two groups during the follow-up
Discussion
Anterior Cruciate Ligament (ACL) repair remains one of the most frequent orthopaedic procedures,which are particularly related to sports participation at any level [9]. Several techniques are in current use, with success rates (till patients return to same level of activity) of between 65 % [10] and 95 % [4]. An ACL tear is commonly treated arthroscopically by using an autograft which is obtained from the hamstring tendons or the patellar tendon. The use of an interference screw for graft fixation is considered to provide higher fixation strength as compared with other devices such as staples or buttons [11,12].
The advantages of metallic interference screws are that they provide solid fixations and that they are generally well tolerated by the body. The disadvantage of using metallic screws are that they can cause lacerations of the grafts while they are inserted [13], their potential interferences with future surgeries which are done in the knee, such as revision ACL reconstructions [14] and their interferences with any future magnetic resonance imaging (MRI) studies of the knee, which are done [15]. In addition, there is the consideration of trying to avoid unneeded foreign material which is retained in the body. With respect to bioabsorbable interference screws, their advantage is their disappearance after they are no longer needed. They cause no interferences with imaging studies, such as future MRI studies, and also they do not interfere with any subsequent knee surgeries. There is also no long-term foreign material which is retained within the body. Concerns which are associated with the use of bioabsorbable interference screws include intraoperative screw breakage, inflammatory responses which lead to accelerated or incomplete absorptions, joint effusions, encapsulations, screw migrations with further damages (whether they are articular or not), increased costs, and the potential for bone tunnel widening [16,17].
In our prospective randomized study which was done to compare the functional outcomes after doing metallic and bioabsorbable interference screw fixations for arthroscopic ACL reconstructions, no statistically significant differences were seen between the two groups with respect to pre-operative variables like age, associated meniscal injury and pre-operative Lysholm and Tegner scores. Similar surgical procedures were done in both the groups, except for the materials and types of interference screws. Both the groups underwent standardized rehabilitation protocols.
Though statistically significant improvements in functional outcomes were noted in each group during successive follow-ups, as were found by Mann-Whitney U-test, no statistically significant difference was seen between the two groups when comparison was done by using independent t-test.
Similar studies which compared use of bioabsorbable and metallic interference screws in ACL reconstructions done with use of different grafts, which were done by C. Marti et al., [18] and Barber FA et al., [19] also did not show statistically significant differences [Table/Fig-5]. A meta-analysis which compared two types of screws, which was done by Rocco Papalia et al., [20] also didn’t show any differences between the two screw types with respect to functional outcomes.
Comparison of results of our study with similar studies
| Bioabsorbable screws | Metallic screws | Mean Lysholm scores | Mean Tegner scores | Conclusion |
|---|
| Our Series | 12 | 12 | 84.33 & 83.67 | 6.5 & 6.67 | Statistically no significant difference |
| C. Marti et al. | 20 | 20 | 82.36 & 84.12 | 6 & 6.5 | Statistically no significant difference |
| Barber FA et al. | 34 | 34 | 94 & 96 | 6.6 & 6.2 | Statistically no significant difference |
Conclusion
In our study, we prospectively compared the function outcomes after doing ACL reconstructions by using hamstring grafts which were fixed by using metallic and bioabsorbable interference screws. Functional assessment was done on basis of Lysholm score and Tegner activity scale. The two groups were compared by using independent t-test. The test revealed no statistically significant differences between two groups. However, further authentication of this result is required which poses a need of doing long term studies.
[1]. Prodromos Chadwick C, Yung Han, Rogowski Julie, Joyce Brian, Shi Kelvin, A Meta-analysis of the Incidence of Anterior Cruciate Ligament Tears as a Function of Gender, Sport, and a Knee Injury–Reduction Regimen ArthroscopyThe Journal of Arthroscopic and Related Surgery 2007 23(12):1320-5. [Google Scholar]
[2]. Frank Cyril B, The Science of Reconstruction of the Anterior Cruciate LigamentThe Journal of Bone and Joint Surgery 1997 79(A):1566-82. [Google Scholar]
[3]. Barber FA, Elrod BF, McGuire DA, Paulos LE, Preliminary results of an absorbable interference screwArthroscopy 1995 11(5):537-48. [Google Scholar]
[4]. Emond CE, Woelber EB, Kurd SK, Ciccotti MG, Cohen SB, A comparison of the results of anterior cruciate ligament reconstruction using bioabsorbable versus metal interference screws: a meta-analysisJ Bone Joint Surg Am 2011 93(6):572-80. [Google Scholar]
[5]. Halewood C, Hirschmann MT, Newman S, Hleihil J, Chaimski G, Amis AA, The fixation strength of a novel ACL soft tissue graft fixation device compared with conventional interference screws: a biomechanical study in vitroKnee Surg Sports Traumatol Arthrosc 2011 19(4):559-67. [Google Scholar]
[6]. Barber FA, Boothby MH, Bilok interference screws for anterior cruciate ligament reconstruction: clinical and radiographic outcomesArthroscopy 2007 23(5):476-81. [Google Scholar]
[7]. Barber FA, Dockery WD, Long-term absorption of poly-L-lactic Acid interference screwsArthroscopy 2006 22(8):820-6. [Google Scholar]
[8]. Shen C, Jiang SD, Jiang LS, Dai LY, Bioabsorbable versus metallic interference screw fixation in anterior cruciate ligament reconstruction: a meta-analysis of randomized controlled trialsArthroscopy 2010 26(5):705-13. [Google Scholar]
[9]. Garrett WEJ, Swiontkowski MF, Weinstein JN, Callaghan J, Rosier RN, Berry DJ, American Board of Orthopaedic Surgery Practice of the Orthopaedic Surgeon: Part-II, certification examination case mixJ Bone Joint Surg Am 2006 88(3):660-7. [Google Scholar]
[10]. Gobbi A, Francisco R, Factors affecting return to sports after anterior cruciate ligament reconstruction with patellar tendon and hamstring graft: a prospective clinical investigationKnee Surg Sports Traumatol Arthrosc 2006 14(10):1021-8. [Google Scholar]
[11]. Kurosaka M, Yoshiya S, Andrish JT, A biomechanical comparison of different surgical techniques of graft fixation in anterior cruciate ligament reconstructionAm J Sports Med 1987 15(3):225-9. [Google Scholar]
[12]. Woo SLY, Wu C, Dede O, Biomechanics and anterior cruciate ligament reconstructionJ Orthop Surg Res 2006 1:2 [Google Scholar]
[13]. Böstman OM, Pihlajamäki HK, Adverse tissue reactions to bioabsorbable fixation devicesClin Orthop Relat Res 2000 (371):216-27. [Google Scholar]
[14]. Bottoni CR, DeBerardino TM, Fester EW, Mitchell D, Penrod BJ, An intra-articular bioabsorbable interference screw mimicking an acute meniscal tears 8 months after an anterior cruciate ligament reconstructionArthroscopy 2000 16(4):395-8. [Google Scholar]
[15]. Fineberg MS, Zarins B, Sherman OH, Practical considerations in anterior cruciate ligament replacement surgeryArthroscopy 2000 16(7):715-24. [Google Scholar]
[16]. Bach FD, Carlier RY, Elis JB, Mompoint DM, Feydy A, Judet O, Anterior cruciate ligament reconstruction with bioabsorbable polyglycolic acid interference screws: MR imaging follow-upRadiology 2002 225(2):541-50. [Google Scholar]
[17]. Böstman O, Hirvensalo E, Mäkinen J, Rokkanen P, Foreign-body reactions to fracture fixation implants of biodegradable synthetic polymersJ Bone Joint Surg Br 1990 72(4):592-6. [Google Scholar]
[18]. Marti C, Imhoff AB, Bahrs C, Romero J, Metallic versus bioabsorbable interference screw for fixation of bone-patellar tendon-bone autograft in arthroscopic anterior cruciate ligament reconstruction. A preliminary reportKnee Surg Sports Traumatol Arthrosc 1997 5(4):217-21. [Google Scholar]
[19]. Barber FA, Elrod BF, McGuire DA, Paulos LE, Bioscrew fixation of patellar tendon autograftsBiomaterials 2000 21(24):2623-9. [Google Scholar]
[20]. Rocco Papalia, Sebastiano Vasta, Stefano D’Adamio, Antonino Giacalone, Nicola Maffulli, Vincenzo Denaro, Metallic or bioabsorbable interference screw for graft fixation in anterior cruciate ligament (ACL) reconstruction?British Medical Bulletin 2013 :1-11. [Google Scholar]