Posterior Reversible Encephalopathy Syndrome in Early Postpartum Women: A Case Report
Vinod Patil S1, B.R. Dhamangaonkar2, R.C. Pattanshetti3, M.M. Patil4
1 Postgraduate, Department of Radiology, Shri BM Patil Medical College, Hospital and Research Centre, Bijapur, Karnataka, India.
2 Professor, Department of Radiology, Shri BM Patil Medical College, Hospital and Research Centre, Bijapur, Karnataka, India.
3 Professor and Head, Department of Radiology, Shri BM Patil Medical College, Hospital and Research Centre, Bijapur, Karnataka, India.
4 Senior Resident, Department of Radiology, Shri BM Patil Medical College, Hospital and Research Centre, Bijapur, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vinod S Patil, Post Graduate Student, Department of Radiology, BLDEU’s Shri BM Patil Medical College, Bijapur-586103, Karnataka, India.
Phone: 9844874076,
E-mail: aagamachaitanya@gmail.com
Posterior reversible encephalopathy syndrome (PRES) is a rare acute neurologic condition, characterized by acute neurological symptoms. The radiological findings are predominantly seen in the posterior cerebral hemispheres and are reversible with appropriate management.
We are reporting a case of a 21-year-old woman (primigravida), who presented with loss of vision, head ache and vomiting on 2nd day of post-caesarean section. Caesarean section was done due to fetal distress. On examination, patient appeared drowsy but arousable, had a blood pressure of 140/114 mmHg, rest of the examination was unremarkable. CT and MRI brain was performed to rule out cerebral venous sinus thrombosis and cortical blindness; imaging and clinical findings were suggestive of posterior reversible encephalopathy syndrome (PRES). She was treated successfully with antihypertensives and showed dramatic improvement.
Posterior reversible encephalopathy syndrome, Postpartum, Preeclampsia, Vasogenic oedema
Case Report
A 21-year-old primigravida with gestation age of 33 weeks 4 days, (according to her last menstrual period) whose first and second trimester gestation was uneventful with no history of hypertension and epilepsy before and during pregnancy. She developed sudden onset of headache, giddiness, vomiting and convulsions. She was diagnosed antepartum eclampsia and treated with antihypertensive (calcium channel blocker), and referred to our institution for further management. On admission, general physical and systemic examination was normal except her blood pressure measuring 142/94 mm of Hg. She was treated with Magnesium sulphate according to Pritchard’s regimen and antihypertensives (calcium channel blocker).Next day patient was taken into caesarean section for fetal distress. Caesarean section was uneventful, done under spinal anesthesia, delivered a live baby of 2.3 kgs.
On 2nd day of post-caesarean section she developed loss of vision, head ache and vomiting. On examination, patient appeared drowsy but arousable, had a blood pressure of 140/114 mmHg. Rest of the general physical examination were unremarkable. CNS examination revealed loss of vision in both eyes with regard to perception of hand movements. Pupillary reactions and results of a fundoscopic examination were normal and Plantar reflex was flexor. Abdominal, cardiovascular, and respiratory system examinations were unremarkable. Biochemical parameters were normal expect urine examination showed 1+ proteinuria.
CT and MRI brain was performed to rule out cerebral venous sinus thrombosis and cortical blindness. Imaging and clinical findings were suggestive of posterior reversible encephalopathy syndrome (PRES). She was treated successfully with antihypertensives (calcium channel blocker) and showed dramatic improvement, her vision improved to 6/6 after two days following commencement of the treatment. She was followed up and MRI at four weeks after initiation of treatment showed disappearance of the previous imaging findings.
Imaging Findings
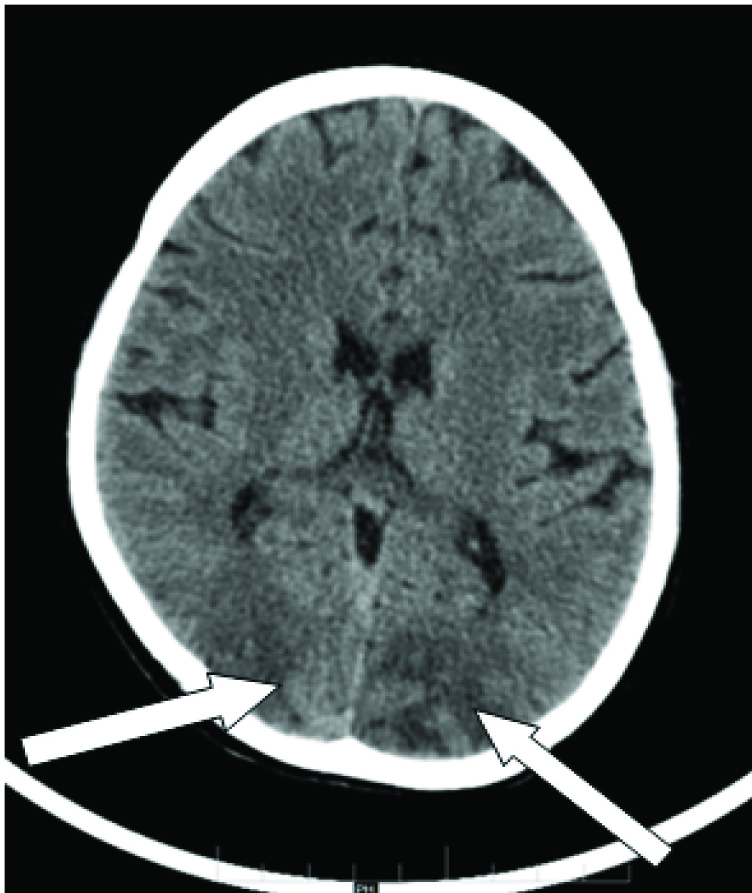
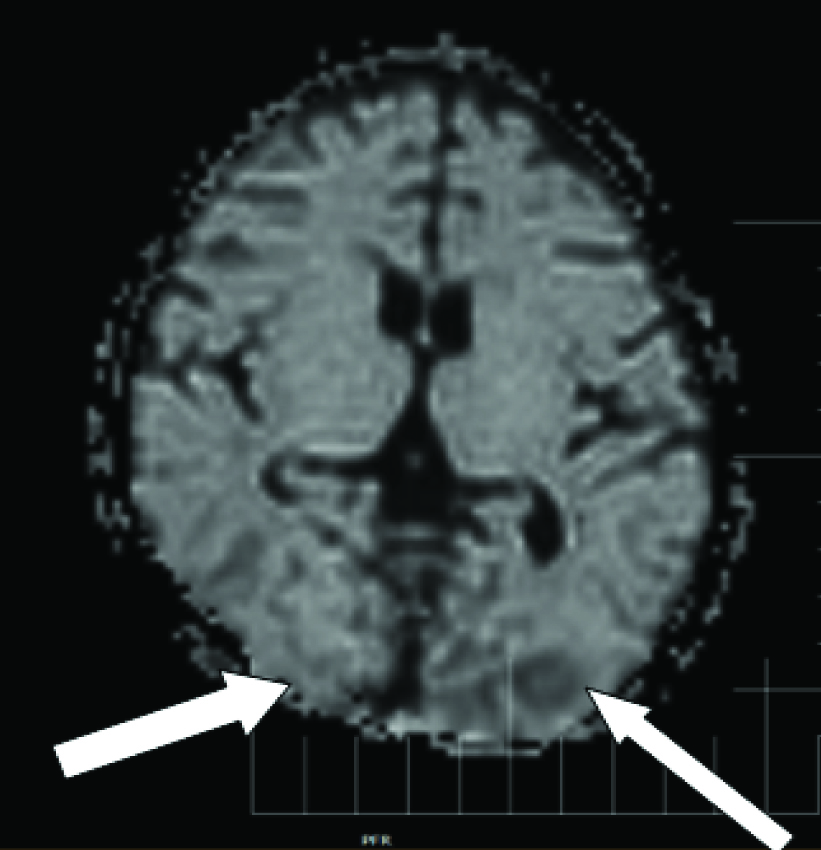
Non-enhanced computed tomography scan showed diffuse low attenuation areas in subcortical deep white matter of bilateral parieto–occipital lobes [Table/Fig-1]. MRI brain showed FLAIR hyperintensities involving predominantly subcortical deep white matter of bilateral parieto- occipital lobes with few areas showing involvement of grey matter [Table/Fig-2], with mixed areas of restriction and free Diffusion was seen in diffusion weighted images [Table/Fig-3].There was no evidence of venous sinus thrombosis or encephalitis features.
Diffuse low attenuation areas are seen in subcortical deep white matter of bilateral parieto – occipital lobes
FLAIR hyperintensities involving predominantly subcortical deep white matter of bilateral parieto- occipital lobes

Mixed areas of restriction and free diffusion in DWI
Four Weeks Later
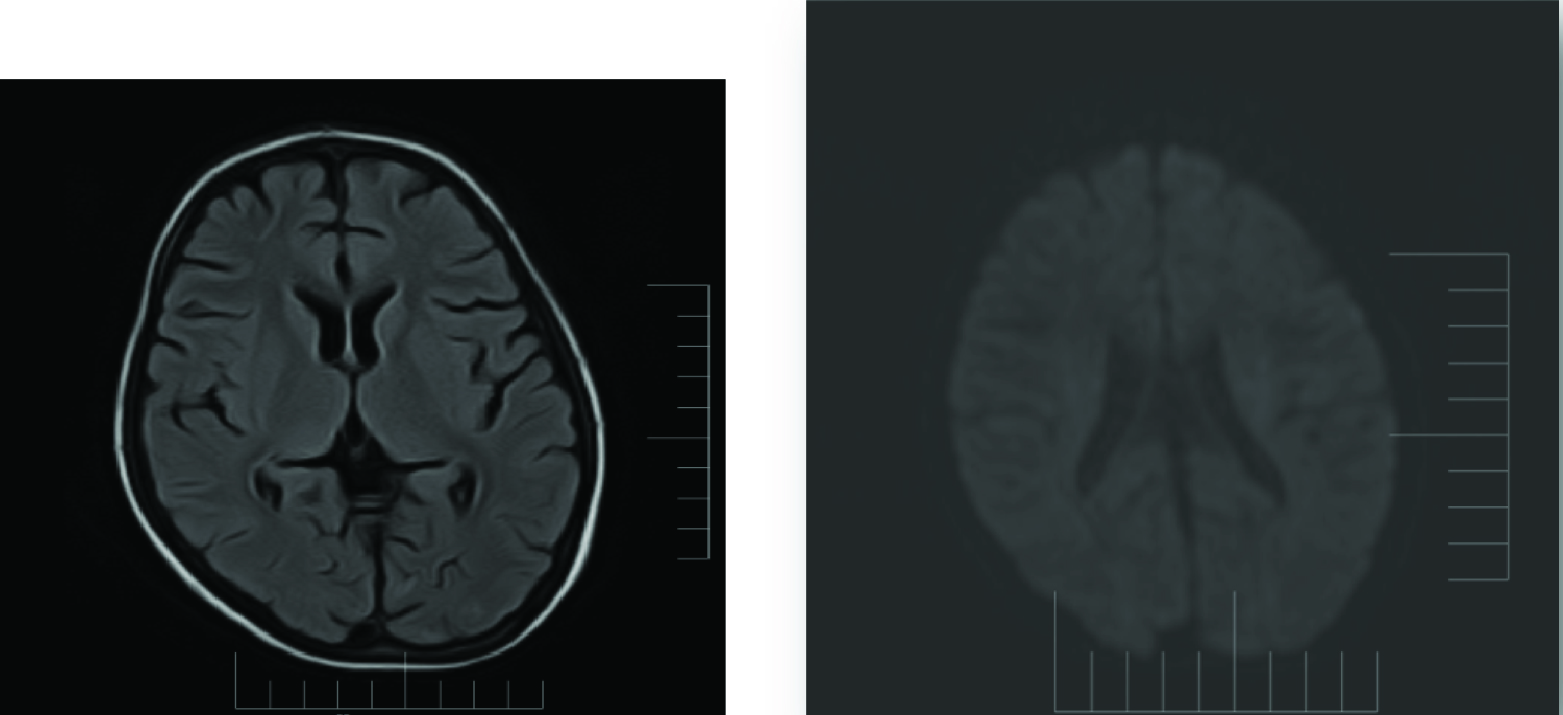
Four weeks follow-up MRI brain study showed disappearance of previous imaging findings [Table/Fig-4].
Disappearance of the previous imaging findings in FLAIR and diffusion sequences
Discussion
Patients with PRES have an acute or subacute clinical presentation of altered mental status, encephalopathy, headache, new onset seizures, and visual disturbances in association with neuroimaging studies consistent with white matter cerebral oedema [1]. Two theories have been proposed to explain the pathophysiology. The more popular theory suggests that hypertension leads to failure of autoregulation, subsequent hyperperfusion, and vasogenic oedema. The other theory suggests that vasoconstriction and hypoperfusion leads to brain ischemia and subsequent vasogenic oedema [2]. Vasogenic oedema within the occipital and parietal regions, perhaps relating to the posterior cerebral artery supply. The oedema is usually symmetrical. Despite being termed posterior, PRES can be found in a non-posterior distribution, mainly in watershed areas, including within the frontal, inferior temporal, cerebellar and brainstem regions [3]. Many conditions exist that are commonly associated with PRES, including hypertensive encephalopathy, preeclampsia/eclampsia, immunosuppressive drugs, renal disease, fluid overload, autoimmune diseases, and sepsis [4]. PRES is characterized by high signal intensity on T2-weighted and FLAIR images, predominantly in the posterior regions, which is caused by subcortical white matter vasogenic oedema. Supplemental diffusion weighted imaging (DWI) and apparent diffusion coefficient (ADC) map images are helpful in distinguishing vasogenic from cytotoxic oedema, which represents foci of irreversible ischemia [3]. The parieto-occipital regions with sparing of the calcarine and paramedian occipital lobe structures help in differentiating it from bilateral posterior cerebral artery infarcts. Neuroradiographic abnormalities of PRES are often apparent on computed tomography (CT) scans but are best depicted by magnetic resonance imaging (MRI) [1,5]. The clinical and neuroimaging findings tend to be reversible once the underlying cause of PRES is identified and treated. Irreversible brain damage can sometimes occur due to late recognition or incorrect treatment [6]. Reversibility of the clinical and radiological findings may take between 5 days to 17 months, although there have been reports where normal function is not fully regained [7].
Conclusion
PRES is an interesting neuro-radiological entity. This condition is important to recognize and to characterize the imaging findings by radiologists, is the key to diagnosing this syndrome. Neuroradiologic imaging is a useful diagnostic tool in the setting of pre-eclampsia and eclampsia to diagnose the disease. Early neuroimaging and more aggressive control of blood pressure may have a role in the management of these patients. Delay in the diagnosis and treatment may result in permanent damage to affected part of brain tissues. The radiologist must be familiar with the imaging abnormalities of this life-threatening, but treatable condition to prevent morbidity and mortality in pregnancy and postpartum.
[1]. Hinchey J, Chaves C, Appignani B, A reversible posterior leukoencephalopathy syndromeThe New England Journal of Medicine 1996 34(8):494-500. [Google Scholar]
[2]. Bartynski WS, Posterior reversible encephalopathy syndrome, part 2: Controversies surrounding pathophysiology of vasogenic edemaAJNR Am J Neuroradiol 2008 29:1043-49. [Google Scholar]
[3]. Bartynski WS, Boardman JF, Distinct imaging patterns and lesion distribution in posterior reversible encephalopathy syndromeAJNR Am J Neuroradiol 2007 28:1320-27. [Google Scholar]
[4]. Lee V H, Wijdicks E F M, Manno EM, Rabinstein AA, Clinical spectrum of reversible posterior leukoencephalopathy syndromeArchives of Neurology 2008 65(2):205-10. [Google Scholar]
[5]. Kastrup O, Maschke M, Wanke I, Diener HC, Posterior reversible encephalopathy syndrome due to severe hypercalcemiaJNeurol 2002 249:1563-66. [Google Scholar]
[6]. Stott VL, Hurrell MA, Anderson TJ, Reversible posterior leukoencephalopathy syndrome: a misnomer reviewedIntern Med J 2005 35:83-90. [Google Scholar]
[7]. Legriel S, Pico F, Azoulay E, Understanding posterior reversible encephalopathy syndromeAnnual Update in Intensive Care and Emergency Medicine 2011 26:631-53. [Google Scholar]