Iatrogenic Stenosis of Anterior Nares: A Case Report
Arunkumar J.S.1, Santosh S. Garag2, Shibani Anchan3
1 Professor, Department of Ear, Nose and Throat, Sri Dharmastala Manjunatheswara College of Medical Sciences and Hospital, Dharwad, Karnataka, India.
2 Assistant Professor, Department of Ear, Nose and Throat, Sri Dharmastala Manjunatheswara College of Medical Sciences and Hospital, Dharwad, Karnataka, India.
3 Assistant Professor, Department of Ear, Nose and Throat, Sri Dharmastala Manjunatheswara College of Medical Sciences and Hospital, Dharwad, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Arunkumar J.S., Professor Department of Ear, Nose and Throat, Sri Dharmastala Manjunatheswara College of Medical Sciences and Hospital, Dharwad-580009, Karnataka, India.
Phone: 09448102501,
E-mail: ctaarun@gmail.com
Stenosis of anterior nares may be congenital or acquired. Acquired stenosis may be caused by the diseases which cause destruction of skin or normal cartilage. The various causes of acquired stenosis of anterior nares are burns, trauma, infections, etc. Iatrogenic stenosis of anterior nares is a rare condition. Doing simple excision of fibrosed tissue, with septoplasty and endoscopic adenoidectomy in a 5-year child, improved nasal breathing. Use of Mitomycin-C topical solution prevents recurrence of fibrosis, with good outcome.
Acquired, Mitomycin-C, Stenosis
Case History
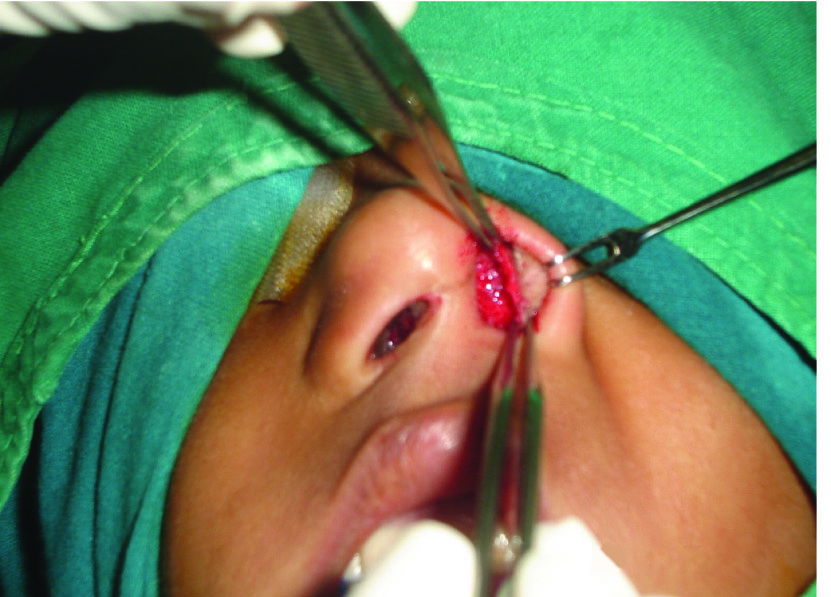
A 5-year-old child presented with bilateral nasal obstruction which was there since childhood. Parents gave a history of premature birth and patient was kept in intensive care unit. Patient was given Ryle’s tube feeding and other life supportive measures, following which child developed complete closure of right nostril and stenosis, with a small opening on left side of the nose. On examination, it was found that there was complete closure of right nostril and a small opening on left side nostril [Table/Fig-1]. There was a scar over the upper part of columella, with a bulbous tip of nose. On cold spatula test, no fogging was seen on right side of the nose and minimal fogging was seen on left side of the nose. Patient was a mouth breather with a high arched palate. Patient was not cooperative for diagnostic nasal endoscopy under local anaesthesia. CT-scan of the paranasal sinuses and nasopharynx was done. The septum was deviated to right side, with a fibrous adhesion [Table/Fig-2], with enlarged adenoids being seen in the nasopharynx. Patient was considered for repair of stenosed anterior nares and endoscopic adenoidectomy. Under general anaesthesia, 2% lignocaine with adrenaline was infiltrated over the stenosed area. On left side, edges of the small opening were freshened and skin was separated from the fibrous and inner mucosal layer circumferentially [Table/Fig-3]. The fibrous tissue was excised along with the mucosa. Outer skin was reflected back and it was sutured to the raw area by using 3-0 vicryl. On right side, the fibrous tissue was excised and septoplasty was done by removing a small piece of deviated septal cartilage anteriorly. Endoscopic adenoidectomy was done by using a microdebrider, through a transnasal approach. Complete haemostasis was maintained throughout the procedure. Then, a No.5 portex endotracheal tube was placed on both sides of the nose as a stent and it was secured to the septum for two weeks. Stent was removed under general anaesthesia and nasal cavity was visualized by using an endoscope. A cotton ball which was soaked in 0.2 mg/ml Mitomycin-C was kept for about one minute over raw area, on the septum and on adjacent parts on both sides. Patient was followed up regularly. At the end of 8 months, patient was found to have good improvement in nasal breathing, with patent anterior nares [Table/Fig-4].

CT-scan showing fibrous adhesion

Intra-operative photograph elevating outer skin layer
Post-operative at the end of 8 months

Discussion
Any stenosis which occurs in tubular cavities tends to be resistant to treatment. Fibrous tissue has a tendency to contract concentrically, leading to constriction ring and stenosis [1]. Stenosis of anterior nares may be congenital or acquired. Acquired stenosis may be caused by diseases which cause destruction of skin or normal cartilage [1]. Congenital stenosis of anterior nares is rare condition which results from failure of canalization of epithelial plug between lateral and medial nasal processes [2]. Iatrogenic trauma caused to the nostril, which results in narrowing of the nasal aperture, can include prolonged nasal packing, chemical cauterization and poorly executed surgical maneouvers, that sacrifice the lining membrane of the vestibule [3]. Stenosis of anterior nares is an uncommon, although a difficult problem, which is faced in clinical practice. In a child in whom premature birth life supportive measures are undertaken, they may damage the mucosa of the nasal cavity, leading to a raw area with fibrosis and stenosis of anterior nares, as it had happened in our case. Taking proper care of the nose by using saline drops and regular cleaning of the nose by an otorhinolaryngologist are required to prevent stenosis of anterior nares.
Several surgical methods have been described for repair of stenosed anterior nares, like, modified Z-plasty which is done for widening the nostril, by taking a small triangular cutaneous flap from the naso-facial region, in order to obtain a long lasting patency of the nostril [4]. The width of the obstruction, the state of the surrounding lining and the degree of the external deformity, are the main factors which have to be assessed during any attempt which is taken at doing a surgical correction. On using standard surgical methods such as a mucous membrane and/or a skin graft and an intranasal local flap, the new nostril has a tendency to restenose. A para-alar crescentic subcutaneous pedicle flap, which was expected to cover the skin defects in and around the philtrum, was applied to treat severe stenosis of the nostril which was caused by scar contracture [5]. This procedure resulted in improvement of nasal obstruction, with a satisfactory postoperative appearance of the external nose. A new technique called double cross plasty has been presented, which has helped in successfully correcting severe unilateral stenosis in two children. Complete nasal stenosis was repaired by using the H-flap technique in two cases. In one case, a cartilage graft was used for creating symmetry of the alar wings. Functional and aesthetic anterior nares are obtained by this technique [6].
Conclusion
Iatrogenic stenosis of anterior nares is not an uncommon condition. Taking improper care of anterior nares in a premature child can result in stenosis. Application of Mitomycin-C solution topically, will prevent recurrence of stenosis after its correction.
[1]. Kacker SK, Sinha A, Management of stenosis of the anterior nares following smallpoxIndian Journal of Otolaryngology and Head and Neck Surgery 1967 19(3):116-20.DOI: 10.1007/BF03048264 [Google Scholar]
[2]. Hazarika P, Nayak DR, Balakrishnan R, Congenital anamolies of nose and paranasal sinusesTextbook of ENT and Head and Neck Surgery 2007 1st editionCBS Publishers and distributors:281 [Google Scholar]
[3]. Daines Steven Marc, Hamilton Grant S. III, Mobley Steven Ross, A Graded Approach to Repairing the Stenotic Nasal VestibuleArch Facial Plast Surg 2010 12(5):332-38. [Google Scholar]
[4]. Tandon DA, Opening the stenosed nostril: how I do it?Indian Journal of Otolaryngology and Head and Neck Surgery 2001 53(1):21-22. [Google Scholar]
[5]. Bozdogan MN, Demir Z, Coskunfirat OK, Velidedeoglu HV, Sahin U, Turkguven Y, H-plasty: a new modification for correction of nasal stenosisAnn Plast Surg 1996 36(1):97-100. [Google Scholar]
[6]. Yamawaki Yoshio, Para-alar crescentic subcutaneous pedicle flap for severe stenosis of anterior naresAmerican Journal of Otolaryngology - Head and Neck Medicine and Surgery 2006 27(3):211-13. [Google Scholar]