Assessment of fetal weight in-utero leads to improved management of high risk pregnancies. It is an independent factor to determine optimal survival of fetus; fetal weight is undoubtedly one of the most significant determinants of neonatal survival. Obstetric ultrasound with its diagnostic modality helps to predict fetal weight with a certain degree of precision. Many clinical methods substantiated by various ultrasound formulas have been used to estimate weight and growth in-utero. Recently, soft tissue markers like fetal subcutaneous tissue thickness, mid-arm circumference, thigh circumference have been used to predict fetal weight in-utero.
Fetal abdominal subcutaneous tissue thickness (FASTT) is one such ultrasound parameter which is an independent factor in predicting big babies and when substantiated with other ultrasound parameters can predict fetal weight for large for gestational age babies. Number of studies done in Asian population is few; the fetuses are likely to have less subcutaneous fat compared to developed countries. The cut off value obtained for western population may not be applicable to Asian population.
The aim of the study was to correlate fetal abdominal subcutaneous tissue thickness (FASTT) measured by ultrasound at term and birth weight measured immediately after delivery and to obtain a cut-off value of FASTT to predict large and small for gestational age babies in our population; coastal district of Southern India.
Methods
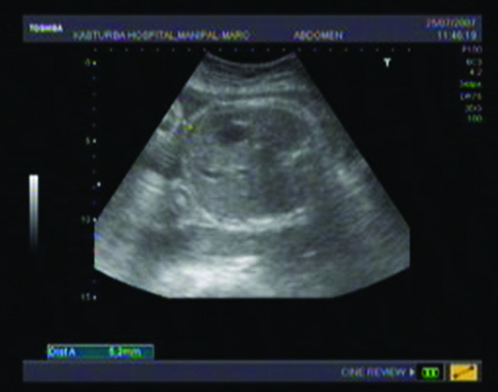
The study was conducted in a tertiary level teaching hospital, and was a prospective observational study. Fetal Abdominal Subcutaneous Tissue Thickness (FASTT) was measured at the anterior 1/3rdof abdominal circumference between outer and inner edges of abdominal wall by ultrasound (Philips HD7) at the level of measurement of abdominal circumference [Table/Fig-1]. Large for gestational age (LGA) is defined as birth weight >90th percentile in our study population and small for gestational age (SGA) as <10th percentile.
Measurement of FASTT by ultrasound
Study included singleton term pregnancies who delivered within one week of estimation of FASTT. All fetuses with ultrasound detected congenital anomalies were excluded from this study. Pearson correlation coefficient (r) was used to study the correlation between FASTT and birth weight, paired t-test was used to compare the FASTT of average for gestational age (AGA), LGA and SGA babies. ROC curve is used to obtain a cut-off of FASTT to predict LGA and SGA babies.
Results
Total of 350 antenatal women were included in the study who fulfilled the criteria during the study period, average maternal age being 27 year, 54.6% (191/350) were primigravidae.
The mean FASTT was 6 mm ± 0.94, with a range of 3.4 mm to 10 mm. Mean birth weight of babies was 2986 g ± 392.8, ranging between 1900 g and 4170 g [Table/Fig-2]. Number of babies weighed as average for gestational age (AGA, between 10th and 90th percentile) was 286 (81.7%), 25 babies (7.1%) were small for gestational age (SGA, < 10th percentile), 39 babies (11.2%) were large for gestational age (LGA, >90th percentile).
Demography and mean FASTT
| Variable | Mean | Range | Standard deviation |
|---|
| Age | 27 year | 19 – 33 | ± 5 |
| Birth weight | 2986 g | 1900 – 4170 | ± 392.8 |
| FASTT | 6 mm | 3.4 - 10 | ± 0.94 |
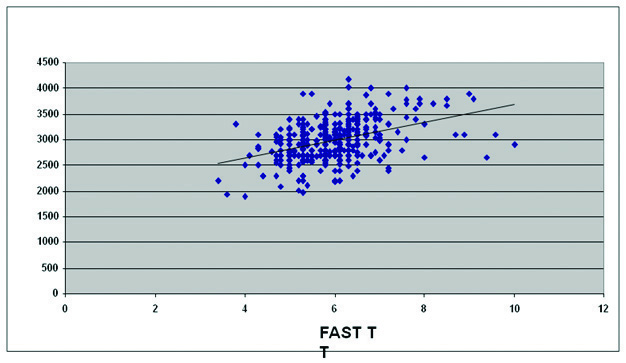
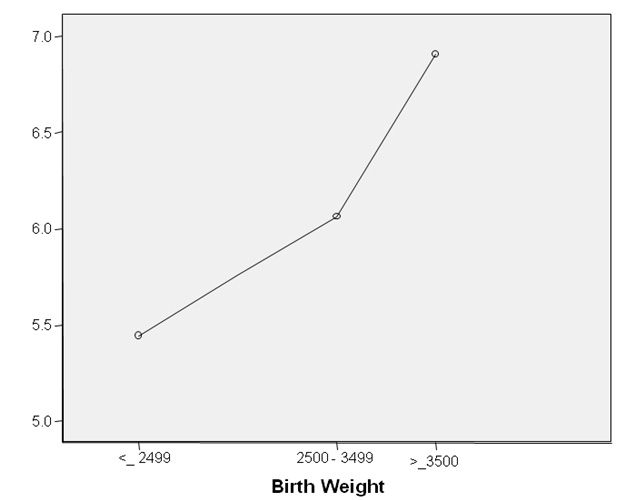
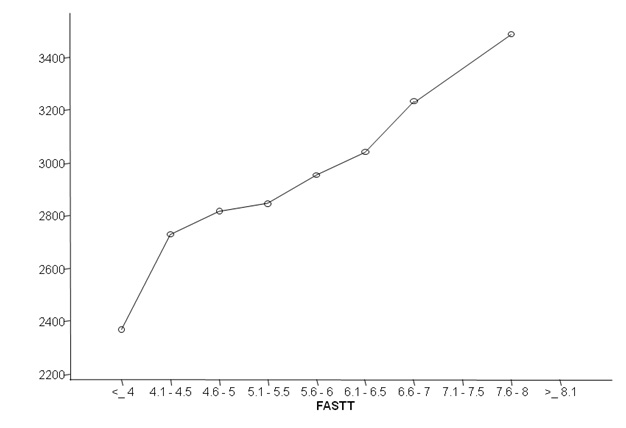
When birth weight was plotted against FASTT (scatter-plot graph), it showed positive correlation as depicted in [Table/Fig-3]. Significance between FASTT and birth weight was obtained by Pearson’s correlation co-efficient (r) which was 0.418. Correlation between FASTT and birth weight, obtained by 2-tailed test, the p-value is 0.0001 (test is significant at 0.01 level), thus confirming the positive correlation between FASTT and birth weight. The mean FASTT for small babies (<2499 g) was 5.44 mm (SD 0.98), for AGA babies 5.9 mm (SD 0.86), and for large babies (>3500 g) 6.89 mm (SD 0.94). Mean FASTT increased as the birth weight increased, vice versa also was true, that is; birth weight increased as FASTT increased. This reinforces positive correlation of mean FASTT with birth weight As depicted [Table/Fig-4a,4b].
Correlation between FASTT and birth weight
Graph showing correlation between birth weight and FASTT
Graph showing correlation between FASTT and birth weight
We studied the difference of mean FASTT between SGA, AGA and LGA babies. The difference in mean FASTT between SGA and AGA babies was statistically significant (p-value 0.032). Similarly, the difference in mean FASTT between LGA and AGA babies was also statistically significant (p-value <0.001). Significance was greater for large for gestation.
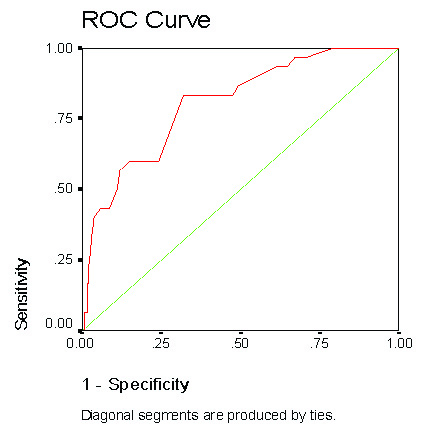
Cut-off value of FASTT for large babies obtained by using Receiver Operative Characteristics (ROC) curve was 6.25 mm [Table/Fig-5a]. Sensitivity for FASTT >6.25mm for large for gestational age babies is 79% and specificity is 70% with a Positive Predictive Value (PPV) is 24.4% and Negative Predictive Value (NPV) is 96.4%. Negative Predictive Value is high, indicating that if the FASTT is less than the cut-off value (6.25 mm in our study), baby is less likely to be large for gestational age (LGA).
ROC curve for large for gestational age fetus
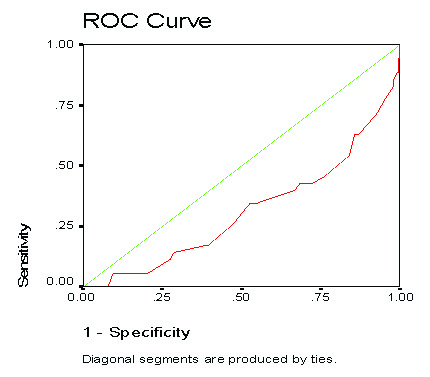
When ROC curve was drawn for small for gestational babies, the curve was towards right and below the line [Table/Fig-5b], hence area under the curve was not significant. Therefore a cut-off value of FASTT for small for gestational age babies could not be obtained.
ROC curve for small for gestational age fetus
Discussion
Fetal growth abnormality (IUGR and macrosomia) are associated with changes in the soft tissue mass, which is decreased in IUGR and increased in macrosomia. Estimated Fetal Weight (EFW) forms an important part of clinical decisions in the management of high-risk groups. In particular, it is important to assess EFW in infants of diabetic mothers as they are at increased risk of macrosomia and its associated complications, including labor dystocia, instrumental delivery, shoulder dystocia and perineal tears. Macrosomic infants are predisposed to childhood obesity and to further morbidity in adult life, including increased insulin resistance, hypertension and diabetes. Fetal macrosomia is associated with increased perinatal morbidity and mortality. Perinatal mortality increases from 3.5 per 1,000 births for infants weighing between 2,500 and 3,500 g to 8 per 1,000 births for infants weighing more than 4,500 g [1]. The antenatal diagnosis of fetal macrosomia is of major importance for labor and delivery management, and for the prevention of fetal and maternal trauma during childbirth.
Several studies have been conducted to find the correlation between subcutaneous tissue thickness and birth weight. Foromouzmehr et al., [2] showed a positive correlation between FASTT and a wide range of fetal weights. Immediate birth weight after delivery was correlated with FASTT measured within 11 days of delivery. Total 300 term mothers were selected. Mean birth weight of 300 newborns was 2875±564 g; out of which 6 (2%) newborns weighed more than 4000 gms and 17 babies (5.7%) weighed less than 2000 gms. The mean FASTT differed significantly between normal and macrosomic fetuses (6.6 mm vs 12 mm respectively; p<0.001). Petrikovsky et al., [3] assessed abdominal subcutaneous tissue thickness in 133 term fetuses of non-diabetic mothers in order to predict macrosomia (birth weight >4000 gms). Birth weight measured was taken of those babies delivered within 72 hours of measurement of FASTT. In this study, there was a significant difference in abdominal wall thickness between those fetuses with normal birth weight and those who were macrosomic (7 mm vs 12.4 mm, p<0.0001). The negative predictive value for a range of cut-off points between 8 and 13 mm varied between 84.3% and 100%. However, the PPV was less than 50% for cut-off values <11 mm. The Negative Predictive Value (NPV) was relatively high (≥90%) for a range of FASTT cut-off values and macrosomia prevalence rates.
Higgins et al., [4] showed that measurement of Anterior Abdominal Wall (AAW) in macrosomic fetuses was significantly increased compared to those with a birth weight <90th percentile. This study shows that a simple additional measurement, AAW, taken at time of routine measurement of Abdominal Circumference (AC), correlates significantly with birth weight. A fetal AAW measurement of >5.6 mm measured at term or an AC > 90th percentile for gestation should alert the obstetrician to the possibility of fetal macrosomia. And the sensitivity to this possibility holds good for gestation <36 weeks although sensitivity increases to almost 100% at 37-38 weeks gestation.
In another study by Bethune et al., [5], showed that fetal fat layer or subcutaneous tissue thickness >5mm was more useful than abdominal circumference as a predictor of macrosomia in 90 pregnancies affected by gestational diabetes, but only took one measurment between 28 and 34 weeks. Parretti et al., [6] investigated AAW thickness specifically in the fetuses of those with impaired glucose tolerance in pregnancy, and showed that AAW thickness increased significantly from 26 weeks compared to normal levels.
Similar results were observed in our study; there was positive correlation between FASTT and birth weight. Mean FASTT increased as the birth weight increases, vice versa also was true. When we studied the difference of mean FASTT between SGA, AGA and LGA babies; the difference in mean FASTT between SGA and AGA babies and between LGA and AGA babies were statistically significant. Significance was greater for large for gestation.
We obtained a cut-off value of FASTT for large babies; 6.25 mm. Sensitivity for FASTT >6.25 mm for large for gestational age babies is 79% and specificity is 70% with a Positive Predictive Value (PPV) is 24.4%and Negative Predictive Value (NPV) is 96.4%. Negative Predictive Value is high, indicating that if the FASTT is less than the cut-off value (6.25 mm in our study),baby is less likely to be large for gestational age (LGA).
Conclusion
There is a positive correlation between Fetal Abdominal Subcutaneous Tissue Thickness (FASTT) and birth weight. FASTT of 6.25 mm is a sensitive test to predict LGA babies and has a high negative predictive value. FASTT measurement for prediction of small babies with birth weight < 2500 g is not sensitive. FASTT can be used as an additional indicator to predict large for gestational age babies along with other known birth weight indicators.