Introduction
Touch is the earliest sense which is developed in human embryology and it is believed to be essential for a good clinical practice [1]. The sense of touch (haptic) is a modality that we use too often in our day to day lives and its importance is eminent. Haptic (or force-feedback) devices are an innovation in the field of art that allow users to feel and touch objects with a great degree of realism [2]. Rapid growth has occurred in the areas of distance learning, interactive telecommunications, computer-assisted instructions, and computer simulations. HAPTICS-are also known as - VIRTUAL REALITY SYSTEMS. The word ‘haptics’ is derived from the Greek word, ‘haptein’, meaning “contact or to touchTM. It is the science of applying a tactile sensation which causes mechanical stimulation to create virtual objects in a computer simulation, to enhance the remote control of machines and devices (telerobotics) [3] [Table/Fig-1]. Haptics refers to sensing and manipulating through touch, enabling the user to touch and feel virtual reality (VR) or an existing distant object indirectly. This sensation can now be added to the current computer models which have sight and sound only. Haptics also provides forced feedback to those who interact with virtual or remote environments, so that a bi-directional flow of information is created. There are special devices like joysticks, data gloves, etc. through which operators can receive feedback from computer applications in the form of sensations which are felt in any part of the body. In combination with a visual display, haptics technology can be used to train people for tasks which require hand-eye coordination, such as surgery and space ship manoeuvres [4]. Haptics allows the operator to “feelTM and work around unseen obstacles through the eminent sense of touch, which thus leads to a significant increase in productivity [5]. Commercial applications of haptics are cellular devices with touch-screen technology (Nokia, Motorola), personal computers (Mac book, Mac bookPro), arcade video games with distant joysticks (Sony), servo systems in large aircrafts. Haptic feedback is also the key to medical interventions, for example when an anaesthetist inserts an epidural needle, a surgeon makes an incision, a dental surgeon drills into a carious lesion or performs microsurgeries [6]. The potential of haptics in the field of medical procedures and acquisition of clinical skills is great and they will affect the medical profession at large.
Definitions of main terms used when describing haptics and the sense of touch [7]
| Haptic | Relating to the sense of touch |
| Proprioceptive | Relating to sensory information about the state of the body |
| Vestibular | Pertaining to the perception of head position, acceleration, and deceleration. |
| Kinesthetic | Meaning the feeling of motion. Relating to sensations originating in muscles, tendons and joints |
| Cutaneous | Pertaining to the skin itself or the skin as a sense organ. Includes sensation of pressure, temperature, and pain |
| Tactile | Pertaining to the cutaneous sense but more specifically the sensation of pressure rather than temperature or pain |
| Force Feedback | Relating to the mechanical production of information sensed by the human kinesthetic system |
Understanding the Technology
Psychomotor skill acquisition research dictates that any movement in the body is initiated by a motor program to the appropriate musculature via a series of commands. These commands identify the muscles which have to be contracted and define the nature of the movement. Once the program is selected, it is run off, and it results in the movement of that muscle [5]. Schmidt suggested that in order for the program to be run, the operator must supply the parameters of the proposed movement, such as duration, speed, force, and movement size. When these parameters are plugged into the general program, an appropriate movement can be made. Performers play a central role in the control of movements.
Haptics are enabled by actuators. Actuators are devices that apply forces for touch feedback, and controllers. Whenever an electrical stimulus is applied, there is mechanical motion in the actuator. Earlier, only electromagnetic technology was used. These electromagnetic motors typically operate at resonance and they provide strong feedback, but produce a limited range of sensations. Newer generations of actuator technologies are emerging, with more rapid response times, which include electroactive polymers, piezoelectric, electrostatic and subsonic audio wave surface actuations [Table/Fig-2]. This mechanical stimulation can be used to assist in the creation of virtual objects in a computer simulation, to control such virtual objects, and to enhance the remote control of machines and devices, thus providing visual and tactile information to the operator in real time [8]. In the fields of medicine and surgery, adding robotic precision to the skill of a clinician by obtaining real time information ensures patient safety, procedural success rate, as well as it facilitates medical and dental training [9].
Generations of haptics [10]
| First | Actuators work on electromagnetic principle Early haptic response systems typically vibrated the whole device with in limited range. |
| Second | Actuators work on electromagnetic principle Micro Chips are used that enable location specific responses to be created. |
| Third | No actuators required. A weak current is sent from a device on the user The oscillating electric field around the skin on their finger tips creates a variable sensation of friction depending on the shape, frequency, and amplitude of the signal. (Reverse-Electrovibration) [6]. |
Haptics, A Key to Medical Interventions
Medicine, from its inception, has been about connecting clinicians with patients through the sense of touch. Technology has changed the way medical practitioners interact with their patients. As technology evolves medical solutions, the opportunity for haptics grows. The use of simulation has been proposed as the next major step in the evolution of health science education [4]. The growth of computer hardware and software has led to the development of virtual worlds that support the field of advanced simulation. Virtual reality allows users to move in the created virtual world in a way which is similar that of moving around to real life. Three-dimensional haptic technology of VR has only been recently proposed as a powerful tool for the education of health professionals. There are critical benefits in the medical space, including.
Tactile Knowledge: Haptics provides immediate and intuitive tactile feedback of relevant information to the users. Enhancement of Performance: Relevant feedback is delivered at the “right timeTM, which thus helps in avoiding distraction and in minimizing ambiguity.
Intuitive Alerts: These assist users in prioritization of important information, multisensory experience, that helps in increasing clinical proficiency and in decreasing medical errors and costs [11].
Haptics and Clinical Skill Acquisition
a. Haptics in medical and dental examinations: This includes characterization of the nature of haptic information, and its perception, e.g. haptic endoscopy [12] laparoscopy [13], sigmoidoscopy, bronchoscopy.
b. Haptics in training and evaluating clinical skills: Students traditionally devote several years to the acquisition of sufficient fine motor skills, for their preparation. Recently, haptic simulators have been introduced into the medical curriculum to address growing need of effective training and evaluation of clinical skills. Such simulators can be applied in a wide variety of medical professions and disciplines, including surgery, interventional radiology, anaesthesiology, dentistry, veterinary medicine, and the allied health professions. This technology has significant potential to complement traditional training approaches, especially in the fields in which hands-on training is not applicable or is as ethical as in dentistry. In most medical fields, plastic models have long been used as a traditional method of training. Thus, virtual reality system is a boon in the fields of medicine and dentistry e.g. virtual haptic back [14], shadow hand, periodontal training simulator (Periosim) [15,16], dental implant surgical simulators [17].
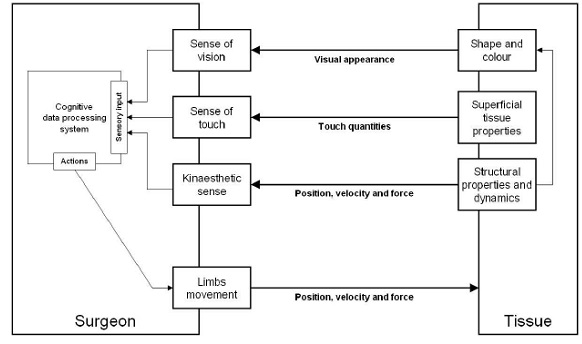
c. Haptics in the improvement of the performance of medical interventions: Current trends in interventional medicine remove direct contact between the patients and clinicians. Bilateral teleoperators and “smartTM instruments that use tactile sensing/display devices, sensory substitution systems and other methods to enhance haptic feedback to a clinician should improve the performance of interventions, e.g. interventional radiology [18], remote surgeries [19] [Table/Fig-3].
Haptic scheme for medical intervention
Haptics in Laproscopic and Endoscopic Surgeries
Haptic feedback in surgery, as an intraoperative, non-invasive, real-time diagnostic tool, turns out to be versatile [13].
Instrumentation which provides artificial tactile feedback promises to be an optional intra-operative diagnostic tool.
Due to its versatility, it may be used in any surgical situation in which the surgeon may require deeper assessment of tissue structures.
Foreign body recognition, including shape and dimensions.
Detection of arterial pulsation Tissue feature evaluation e.g elasticity, kinematics, pathological status.
It is known that in surgery, sensoric stimuli are best felt through bare hands, followed by conventional surgical instruments, and lastly, by endoscopic instruments [20,21]. The amount of sensitivity loss which is measured when using endoscopic instrumentation instead of bare fingers, varies between a factor of 8–20 [20]. The main cause of disturbance of haptic sensations is frictional forces [22]. Frictional forces are forces which are caused by the friction between the instruments and the trocar. Frictional force may be reduced when the mechanical efficiency of the endoscopic instrument is enhanced, for instance, by lubricating the shaft of the instrument. As a result, the amount of haptic feedback may be enhanced [21]. It seems that by combining several factors, such as visual feedback, haptic feedback, and endoscopic experience, performances of certain surgical tasks can be improved [23]. Video analysis of endoscopic procedures showed tissue slippage which occurred during grasping actions, which resulted in tissue damage, when haptic feedback was absent [24,25]. The concept is indeed promising. Surgeons could possibly benefit from additional feedback, but there is still much to learn about the specifics and advantages of included force feedback when it comes to prevention of surgical errors.
Haptics for Neurosurgery Simulation [
26]
Convergence of political, economic, and social forces has limited, neurosurgical, resident operative exposures. There is a need to develop realistic neurosurgical simulations that reproduce the operative experience, which is unrestricted by time and patient safety constraints. A computer-based, virtual reality platform offers simulated resistance and relaxation, with passage of a virtual three-dimensional ventriculostomy catheter through the brain parenchyma into the ventricle. A dynamic, three-dimensional, graphical interface renders a changing visual perspective, as the user’s head moves, e.g. Second Generation Haptic Ventriculostomy Simulator Using the ImmersiveTouchTMSystem.
Surgical Simulation System for Cleft Lip Planning and Repair
This system allows the user to interact with a virtual patient to perform the traditional steps of cleft-lip repair. The system interfaces to force-feedback (haptic) devices to track the user’s motion and to provide feedback during the procedure, while performing real-time soft-tissue simulation. The user is prompted to select anatomical landmarks on the patient data for preoperative planning purposes and then their locations are compared against those of a “gold standardTM and a score which is derived from their deviations from that standard and time which are required, is generated [27]. The user can then move a haptic stylus and guide the motion of the virtual cutting tool. The soft tissues can thus be incised by using this virtual cutting tool, which is moved by using virtual forceps, and they can be fused, in order to perform any of the major procedures for cleft-lip repair.Simulator is a valuable training tool which provides residents with a means to practise anatomical identification for cleft lip surgery without the risks which are associated with training on a live patient. Educators can also use the simulator to examine as to which markers are consistently problematic, and modify their training to address these needs e.g Bio Digital system cleft lip palate virtual simulator – Smile train 3-D real time simulator [28].
Robotic Arm
According to the Robot Institute of America, “A robot is a reprogrammable, multifunctional manipulator which is designed to move materials, parts, tools or specialized devices through variable programmed motions, for the performance of a variety of tasksTM. This interaction of robot with environment is commonly accomplished by using some sort of arm and gripping device or end effectors. The robotic arm has a few joints which are similar to those of a human arm, in addition to shoulder, elbow, and wrist, coupled with the finger joints [29].
Haptic Robot arm is used for various applications,
To lift heavier objects.
To lift nuclear wastes without harming humans.
To use as external limbs of a surgeon during complex retinal or heart surgeries.
To use as prototype for a Bomb disposal robot.
Needle Simulation
This is an important topic and it has several applications in clinical procedures, e.g., biopsies, injections, neurosurgery, brachy therapy cancer treatment, spinal anaesthesia and regional anaesthesia. Training opportunities are limited and there is a lack of available, virtual reality-based (VR) simulators. The first anaesthesia simulator, SIM1, was described in 1969, and the progress made in computer technology led to the development of different systems, including high-fidelity simulators [30]. However, the limited numbers of virtual reality (VR)-based simulators for RA, narrow their use for training purposes. Needle simulation requires profound theoretical knowledge and repeated performances to gain sufficient manual skills for successful accomplishment of such procedures. Although there is widespread utilization of simulators for learning and improving medical skills in general and sophisticated full-scale simulators for general anaesthesia, the use of such mannequins for RA and spinal anaesthesia is limited, e.g. Chiba needles for haptic rendering. According to the Haptics Optional Surgical Training System (HOSTS) which is developed for the US Army, a training system has to fulfil several criteria These include:
Identification of the right injection site and proper injection angle.
keeping the hand position at the proper angle and stably during the injection, which requires knowledge of the appropriate hand position for each block position and proper needle placement during injection.
Ensuring that a nerve is not pierced and featuring the ability to assess nerve stimulation.
Haptic Interaction with 3D Ultrasound Data
Touch Your Baby Before He or She is Born. This system is being currently targeted for use in pre-natal imaging Parents are able to interactively feel as well as see three-dimensional imagery of the child. This has several important benefits. First of all, it allows physicians to more clearly explain the developmental process, progress of growth of foetus to parents- to- be and any existent complications. Secondly, it helps in easing parental stress and anxiety over the progress of their child. Finally, it helps the all-important parent-child bonding process. The system can further be refined in order to be used for medical diagnosis, surgical planning, and intraoperative procedures, E.g The e-Touch sonoTM system [31].
Training is typically done in laboratory settings, in which students work on each other with teacher-student ratios, that make it difficult for students to get the levels of feedback that they desire, as to whether they are feeling what they are supposed to be feeling. These settings also seldom provide the ranges of ages and conditions which are typical of patient populations that the students will eventually be treating.The development of the virtual haptic back (VHB) was undertaken to address these limitations. It is a simulation of the contours and the tissue textures of human backs and is presented to users both haptically and graphically, i.e., by feeling and by sight. The simulation is based on measurements of real backs, with the contours being captured by 3D photography and the tissue texture being measured as tissue compliance (the inverse of stiffness), e.g. PHANToM 3.0 haptic interface (SensAble Technologies, Woburn, MA).
Haptic Surgical Correction of Dento-Facial Deformities [
32]
Research is focused on conducting projects to improve the diagnosis and management of dentofacial deformities. Applying the recent advances in stereophotogrammetry, haptics, enables us to Establish 3D facial characteristics of non-deformed faces.
Study the 3D soft tissue changes in response to several skeletal orthognathic procedures.
Assess the accuracy of prediction planning in orthognathic surgeries.
Build a mathematical model to measure facial scarring.
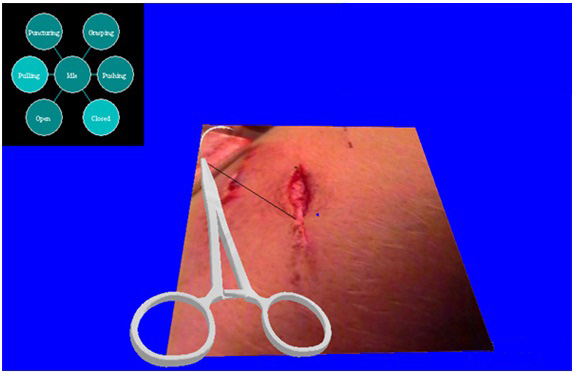
Haptic Suturing Simulator
This simulator incorporates several interesting components such as real-time modeling of deformable skin, tissue and suture material and real-time recording of state of activity during performance of the task by using a finite state model. Actual needle holders are attached to the haptic device, as the graphics of the haemostats, needles, sutures, and virtual skin are displayed and updated in real-time. But a somewhat realistic, tactile force feedback is provided to the learner. Ongoing development is focused upon providing users with a more accurate force feedback, a scoring mechanism, and added instructional functions. The goal is to provide an efficient method to learn the suturing procedure by measuring surgical skills in a simulator [33].
Review of Studies For Haptic in Medicine
| Lanfranco et al., [40] | Haptic feedback is decreased in conventional endoscopic surgery |
| Picod G [22] | The forces of interaction between organs and instrument tips during endoscopic gestures range from 0.1–10 N |
| Thole G [24] | Haptic feedback is best felt through: 1. Bare hands 2. Instruments for open surgery. 3. endoscopic instruments |
| Lemole GM [26] | Haptic feedback offers simulated resistance and relaxation with passage of a virtual three-dimensional ventriculostomy catheter through the brain parenchyma into the ventricle. |
| Cristian Luciano [26] | During the experiment, medical students improved their performance from 10%-50% to 100% in fewer than 30 trials showing the potential of the ventriculostomy simulator. |
| Strauss G [41] | VSR systems have the potential to revolutionize surgical training. All surgical experienced probands evaluated the VSR-scenario as near-to-reality. |
| Montgomery K, [42] | The simulator is a valuable training tool, giving residents a way to practice anatomical identification for cleft lip surgery without the risks associated with training on a live patient. Educators can also use the simulator to examine which markers are consistently problematic, and modify their training to address these needs. |
| Schendils [43] | Soft tissue deformation of the haptic mesh realistically simulates normal tissues when haptic-rate (>1 kHz) force-feedback is provided. |
| Rama Krishna [44] | A robotic arm with four degrees of freedom designed is able to pick the objects with a specific weight and place them in a desired location. To facilitate the lifting of the objects, Servomotors with a torque of 11 kg are used. Haptic Robot arm is used for various applications, of them few are as follows: To lift heavier objects To lift nuclear wastes without harming the humans Used as external limbs of a surgeon during a complex retinal or heart surgeries Prototype for a Bomb disposal robot |
| O.Grottke [45] | Technically, VR simulators do not consider individual patients’ anatomy and cannot be adapted to different regions such as the inguinal region, spine, neck, or arm. |
| Amir M [46] | Pilot human factor studies have demonstrated the significant potential for scientific and commercial applications of HUTS {haptic ultrasound training system). The system is portable, inexpensive and is able to demonstrate US reslicing together with other reg.istered imaging modalities simultaneously |
| Gottlieb R [47] | Faculty perceptions of VRS students’ abilities were higher than for non-VRS students for most abilities examined. Since ergonomic development and technical performance were positively impacted by VRS training, the results support the use of VRS in a preclinical dental curriculum. |
| Jasinevicius TR, [48] | Compared the efficacy of a virtual reality computer-assisted simulation system (VR) with a contemporary non-computer-assisted simulation system (CS). Faculty spent 44.3 hours “interactingTM with twenty-eight students, averaging 0.5 hours per VR student and 2.8 hours per CS student. Thus, CS students received five times more instructional time from faculty than did VR students. |
| Lackey MA [49] | This study completed its first year of student experience using 40 DentSim simulators, in conjunction with an 80-unit traditional simulation laboratory. The results of the first-year experience were encouraging, although certain areas proved problematic and frustrating for both students and staff. |
| Suvinen TI [50] | Student response to teaching and learning in the simulator over a 3-year evaluation period, collected via a student questionnaire was uniformly positive. Students were very enthusiastic about the learning environment and educational approach, preferring it to traditional preclinical laboratory instruction |
Robot Assisted Surgery
These systems are teleoperated with the surgeon at a console, controlling a `joystick’ and with the instruments being manipulated by robotic arms inside the patient [34], e.g. Da Vinci’-system produced by Intuitive Surgicals.
Figure: Schematic overview of a telesurgical system. Some advantages of robotic telemanipulation [35].
Limited dexterity is restored, as the surgeon no longer has to move the instruments. This can be done via a foot pedal which is used to freeze the instruments.
Surgeon can sit in a comfortable position and make a robotic.
Visualization is improved, and it can even be three-dimensional.
There is ‘tremor eradication.
The main limitation of current technology of robot assisted surgery is reduced number of degrees of freedom, which results in low manipulability of the surgical instruments, no force or tactile feedback, absence of a natural interface and the robotic hardware being expensive [36].
Haptics in Dentistry
Even though use of complex and realistic medical simulators is becoming more and more common in medical education, the use of simulators in the field of dentistry has not been well exploited as yet. Dental simulators provide an efficient means to quickly teach preclinical dental students dental procedures, while increasing their hand-skills considerably. Repetitive procedures such as proper hand and instrument usage and placement are primary targets which have to be learned on dental simulators [37]. Two kinds of dental simulators are currently available: manikin-based simulators that provide a physical model of the patient’s head and mouth, on which certain dental procedures can be performed by using real dental instruments e.g DentSimTM, which is developed by [DenX Ltd], Image Guided Implantology (IGI) which is also developed by DenX, Ltd and haptics based simulators that employ a PHANToMTM haptic device [SensAble Technologies, Inc.] and virtual models of a human tooth or mouth as a platform for facilitating dental practices e.g Virtual Reality Dental Training System (VRDTS) [Novint Technologies], Iowa Dental Surgical Simulator [IDSS] [38]. Instead of using real dental instruments, the trainee holds the haptic device stylus to manipulate a set of virtual instruments that are shown on a monitor screen. The tactile feedback reproduces clinical sensations in the hand of the operator who is using dental instruments.
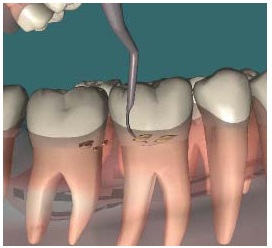
Calculi Being Removed with Haptic Scaler
Challenges Associated with Haptic Technology
Integrating haptics poses technical challenges on all fronts: haptic interface hardware design, tissue and organ model development, tool–tissue interactions, real-time graphical and haptic rendering, and haptic recording and playback [38,39].
*Haptic Devices Design
One of the constant challenges associated with integration of haptics into virtual environments is the need for haptic interface devices with the requisite DOF, range, resolution, and frequency bandwidth, both in terms of forces and displacement. With current technology, it is hard to imagine using a single universal device for all medical procedures, and it is likely that groups of similar medical procedures can be simulated with specific devices [Table/Fig-4,5and6].
*Tool–Tissue Interaction
Interaction between instrument and an organ occur during a surgery. Realistic visual and haptic rendering of tissue cutting, bleeding, and coagulation are important components of a surgical simulator. The physics of the dynamic phenomena which underlie surgical cutting or tearing of soft tissues is extraordinarily complex. Accurately modeling the interactions between the sharp edge of a tool and the soft tissue has been proven to be rather difficult.
*Organ Models
In vivo tissue mechanics are critical for measuring material parameters which are needed for realistic simulations. In addition, current organ-force models are linear, homogeneous, and isotropic. Such models are inadequate for representing the inherent nonlinearities, anisotropy, and rate dependence of soft tissues. Complex tissue models, on the other hand, are computationally expensive. The accuracy requirements of organ models must also be investigated from the perspective of human haptic perceptions. Constructing a multilayered computational architecture is highly useful.
*Real-Time Rendering
The number of computations which are required for real-time visual and haptic rendering of organ-force models is another bottleneck in our simulations.
*Haptic recording and playback: Also important are the benefits of using the same haptic device to simultaneously record and display haptic stimuli for MISST. Although considerable interest in haptic display of compliant objects for MISST exists, the haptic recording and playback concepts require further exploration.
Future Applications of Haptics
Future applications of haptic technology cover a wide spectrum of human interactions with technology. Some other applications are Virtual Reality interfaces used for an internet shopping mall (remotely touching materials like clothes via the internet, CAD or other tangible spaces). Research focuses on the mastery of tactile interactions with distant objects, which if successful, may result in applications and advancements in gaming, movies, manufacturing, medical, and other industries. The medical industry stands to gain from virtual and telepresence surgeries, which provide new options for medical care One currently developing medical innovation is a central workstation which is used by surgeons for performing operations remotely. Local nursing staff set up the machine and prepare the patient, and rather than travelling to an operating room, the surgeon becomes only a telepresence [15]. This allows expert surgeons to operate from across the country, thus increasing availability of expert medical care. It is a useful tool for simulating surgery for training purposes. Haptic technology aids in the simulation by creating a realistic environment of touch. Yet, current trends in medical technology and training methods involve less haptic feedback to clinicians and trainees.Performances of experts and novices can be modelled by using artificial intelligence techniques, in order to provide immediate constructive feedback to trainees during clinical skill practice.
Conclusion
In the future, robots and intelligent machines should adapt themselves autonomously to the open environment, in order to realize physical support that they provide for human activities. Advanced technology simulation is on the verge of dramatically affecting health care education. Specifically, virtual reality-based technology allows a more advanced simulation, thereby setting new state-of-the-art medical and dental simulations.The science and technology of haptics thus has great potential to affect the performance of medical procedures and learning of clinical skills.
[1]. Dunkin B, Adrales GL, Apelgren K, Mellinger JD, Surgical simulation: a current reviewSurg Endosc 2007 21:357-66. [Google Scholar]
[2]. Robles de la Torre G, The importance of the sense of touch in virtual and real environmentsIEEE Multimedia 2006 [Google Scholar]
[3]. Urbankova A, Engebretson SP, The use of haptics to predict preclinic operative dentistry performance and perceptual abilityJ Dent Educ 2011 75(12):1548-57. [Google Scholar]
[4]. Buck GH, Development of simulators in medical educationGesnerus 1991 48:7-28. [Google Scholar]
[5]. Robles-De-La-Torre G, Principles of Haptic Perception in Virtual Environments. In Grunwald M (Ed.)Human Haptic Perception 2008 VerlagBirkhäuser [Google Scholar]
[6]. Smith CD, Simulation technology: a strategy for implementation in surgical education and certificationPresence Tele-Operators and Virtual Environments 2000 9:632-7. [Google Scholar]
[7]. Oakley I, McGee M, Brewster SA, Gray PD, Putting the feel in look and feelIn Proceedings of ACM CHI 2000 2000 The Hague, NetherlandsACM Press, Addison-Wesley:415-22. [Google Scholar]
[8]. Schmidt RA, Motor control and learning: a behavioural emphasis 1982 ChampaignHuman Kinetics Publishers [Google Scholar]
[9]. Freimuth Klein DH, Monkman GJ, Egersdörfer S, Meier A, Böse H. M, Electrorheological Tactile ElementsMechatronics. Pergamon 2005 15(7):883-97. [Google Scholar]
[10]. Ashwell Rob, (12/08/2011). Haptic controller chips offer low latencyEE Times Asia [Google Scholar]
[11]. Okamura MA, Basdogan C, Baillie S, Harwin WS, Haptics in Medicine and Clinical Skill AcquisitionIEEE Transactions on Haptics 2011 4(3):153-4. [Google Scholar]
[12]. Hashizume M, Shimada M, Tomikawa M, Ikeda Y, Takahashi I, Abe R, Early experiences of endoscopic procedures in general surgery assisted by a computer enhanced surgical systemSurgical Endoscopy 2002 16:1187-91. [Google Scholar]
[13]. Székely G, Modeling of Soft Tissue Deformation for Laparoscopic Surgery SimulationProc. 1st Int’l Conf. Medical Image Computing and Computer-Assisted Intervention (MICCAI), LNCS 1496 1998 Springer-Verlag:550-61. [Google Scholar]
[14]. Howell JN, Conatser RR, Williams RL II, Burns JM, Eland DC, Training for palpatory diagnosis on the Virtual Haptic Back: performance improvement and user evaluationsJ Am Osteopath Assn 2008 108(1):29-36. [Google Scholar]
[15]. Steinberg AD, Banerjee P, Drummond J, Zefran M, Progress in the Development of a Haptic/Virtual Reality Simulation Program for Scaling and Root PlanningJ Dent Edu 2003 67(2):161 [Google Scholar]
[16]. Steinberg AD, Bashook PG, Drummond J, Ashrafi S, Zefran M, Assessment of faculty perception of content validity of PerioSim, a haptic-3D virtual reality dental training simulatorJ Dent Edu 2007 71:1574-82. [Google Scholar]
[17]. Rhienmora P, Haddawy P, Dailey M, Khanal P, Suebnukarn S, Development of a dental skills training simulator using virtual reality and haptic deviceNECTEC Technical Journal 2008 8:140-7. [Google Scholar]
[18]. Suebnukarn S, Haddawy P, Dailey M, Cao DN, Interactive Segmentation and three-dimension reconstruction for cone-beam computed-tomography imagesNECTEC Technical Journal 2008 8:154-61. [Google Scholar]
[19]. Judkins TN, Oleynikov D, Stergiou N, Objective evaluation ofexpert and novice performance during robotic surgical training tasksSurg Endosc 2009 23:590-7. [Google Scholar]
[20]. Den Boer KT, Herder JL, Sjoerdsma W, Meijer DW, Gouma DJ, Stassen HG, Sensitivity of laparoscopic dissectors: what can you feel?Surg Endosc 1999 13869-873 [Google Scholar]
[21]. Lehnert M, Richter B, Beyer PA, Heller K, A prospective study comparing operative time in conventional laparoscopic and robotically assisted Thal semifundoplication in childrenJ Pediatr Surg 2006 41:1392-96. [Google Scholar]
[22]. Picod G, Jambon AC, Vinatier D, Dubois P, What can the operator actually feel when performing a laparoscopy?Surg Endosc 2005 19:95-100. [Google Scholar]
[23]. Tholey G, Desai JP, Castellanos AE, Force feedback plays a significant role in minimally invasive surgery: results and analysisAnn Surg 241 :102-109. [Google Scholar]
[24]. Sjoerdsma W, Herder JL, Horward MJ, Jansen A, Bannenberg JJG, Grimbergen CA, Force transmission of laparoscopic grasping instrumentsMinim Invasive Ther Allied Technol 1997 6:274-78. [Google Scholar]
[25]. Heijnsdijk EAM, Dankelman J, Gouma DJ, Effectiveness of grasping and duration of clamping using laparoscopic graspersSurg Endosc 2002 16:1329-31. [Google Scholar]
[26]. Lemole GM Jr, Banerjee PP, Luciano C, Neckrysh S, Charbel FT, Virtual reality in neurosurgical education: part-task ventriculostomy simulation with dynamic visual and haptic feedbackAnesth Pain Med 2011 36(1):12-6. [Google Scholar]
[27]. Ranta JF, Aviles WA. The virtual reality dental training system: simulating dental procedures for the purpose of training dental students using haptics. Presentation at Fourth Phantom Users Group Workshop, Cambridge, MA, October 9-12 [Google Scholar]
[28]. Montgomery K, Sorokin A, Lionetti G, Schendel S, A surgical simulator for cleft lip planning and repairShorten GDStud Health Technol Inform 2003 94:204-9. [Google Scholar]
[29]. Krishna Rama, Bala G. Sowmya, Sastry A.S.C.S., Sarma B. Bhanu Prakash, Alla Gokul Sai, Design and Implementation ofa Robotic Arm Based On Haptic TechnologyInternational Journal of Engineering Research and Applications 2012 2(3):3098-10. [Google Scholar]
[30]. Basdogan C, Srinivasan MA, Haptic Rendering In Virtual EnvironmentsHandbook of Virtual Environments, K. Stanney, ed 2002 :117-34. [Google Scholar]
[31]. Woo J. A short History of the development of Ultrasound in Obstetrics and Gynecology, http://www.ob-ultrasound.net/history.html [Google Scholar]
[32]. Khambay B, Nairn N, Bell A, Miller J, Bowman A, Ayoub A, Validation and reproducibility of a high resolution 3D facial imaging systemBrit J Oral Maxillofac Surg 2008 46:27-32. [Google Scholar]
[33]. O’Toole RV, Playter RR, Krummel TM, Blank WC, Cornelius NH, Roberts WR, Bell WJ, Raibert M, Measuring and developing suturing technique with a virtual reality surgical simulatorJ Am Coll Surg 1999 189:114-27. [Google Scholar]
[34]. Sastry SS, Cohn MB, Tendick F, Milli-robotics for remote, minimally invasive surgeryRobotic and Autonomous Systems 1997 21:305-16. [Google Scholar]
[35]. Okamura AM, Methods for haptic feedback in teleoperated robot-assisted surgeryIndustrial Robot 2004 31(6):499-508. [Google Scholar]
[36]. Jasinevicius TR, Landers M, Nelson S, Urbankova A, An Evaluation of Two Dental Simulation Systems: Virtual Reality versus Contemporary Non-Computer-AssistedJ Dent Educ 2004 68(11):1151-62. [Google Scholar]
[37]. Johnson L, Thomas G, Dow S, Stanford C, An initial evaluation of the Iowa dental surgical simulatorJ Dent Educ 2000 64:847-53. [Google Scholar]
[38]. Jacobus C, et al., Method and system for simulating medical procedures including virtual reality and control method and system, US Patent 5,769,640 [Google Scholar]
[39]. Brown J, “Algorithmic Tools for Real-Time Microsurgery Simulation,TMMedical Image Analysis 2002 6(3):289-300. [Google Scholar]
[40]. Lanfranco AR, Castellanos AE, Desai JP, Meyers WC, Robotic surgery: a current perspectiveAnn Surg 2004 239:14-21. [Google Scholar]
[41]. Strauss G, Trantakis C, Nowatius E, Falk V, Virtual training in head- and neurosurgeryLaryngorhinootologie 2005 May 84(5):335-44. [Google Scholar]
[42]. Montgomery K, Sorokin A, Lionetti G, Schendel S, A surgical simulator for cleft lip planning and repairStud Health Technol Inform.42 2003 94:204-9. [Google Scholar]
[43]. Schendel S, Montgomery K, Sorokin A, Lionetti G, A surgical simulator for planning and performing repair of cleft lipsJ Craniomaxillofac Surg 2005 33(4):223-8. [Google Scholar]
[44]. Krishna Rama, Bala G. Sowmya, Sastry A.S.C.S., Sarma B. Bhanu Prakash, Design And Implementation Of A Robotic Arm Based On Haptic TechnologyInternational Journal of Engineering Research and Applications (IJERA) 2012 2(3):3098-3103.:3098 [Google Scholar]
[45]. Grottke O, Ntouba A, Ullrich S, Liao W, Fried E, Prescher A, Virtual reality-based simulator for training in regional anaesthesiaBritish Journal of Anaesthesia 2009 103(4):594-600. [Google Scholar]
[46]. Tahmasebi Amir M, Abolmaesumi P, Thompson D, Hashtrudi-Zaad K, First Canadian Student Conference on Biomedical Computing [Google Scholar]
[47]. Gottlieb R, Lanning SK, Gunsolley JC, Buchanan JA, Faculty impressions of dental students’ performance with and without virtual reality simulationJ Dent Educ 2011 75(11):1443-51. [Google Scholar]
[48]. Jasinevicius TR, Landers M, Nelson S, Urbankova A, An evaluation of two dental simulation systems: virtual reality versus contemporary non-computer-assistedJ Dent Educ 2004 68(11):1151-62. [Google Scholar]
[49]. Lackey MA, One year’s experience with virtual reality preclinical laboratory simulation at the University of TennesseeInt J Comput Dent 2004 7(2):131-41. [Google Scholar]
[50]. Suvinen TI, Messer LB, Franco E, Clinical simulation in teaching preclinical dentistryEur J Dent Educ 1998 2(1):25-32. [Google Scholar]