Aberrations in the root canal anatomy are a commonly occurring phenomenon. Although the mandibular second molar is commonly a bi-rooted tooth with an uncomplicated endodontic anatomy, variations have to be considered every time endodontic therapy is performed. This case report describes the non-surgical endodontic retreatment performed on a mandibular second molar with four seperate roots and canals. ProTaper Universal rotary nickel-titanium instruments (Dentsply Maillefer, Ballaigues, Switzerland) for treatment and retreatment were used to remove the old gutta percha and to clean and shape all root canals, followed by the complete obturation of root canal system. Post-operative CBCT scan was taken to confirm the quality of the performed treatment.
Mandibular second molar, Root canal morphology, Anatomical variations, Retreatment, Root canal therapy
Introduction
Many of the difficulties in root canal treatment are due to variations in root canal morphology. A thorough knowledge of the basic root canal anatomy and its variations is necessary for successful completion of the endodontic treatment [1] . An unshaped and unfilled root canal will lead to failure of the endodontic therapy in a very short time [2] . A clinician can suspect unusual morphology either when radiographs offer clue of additional roots and canals or clinically when he encounters odd shaped pulp chamber of the tooth. Extra roots are an additional challenge, which begins at case assessment and involves all operative stages, including cavity design, canal access, localization, cleaning, shaping and obturation of the root canal system[3] .
According to Vertucci [4] the mandibular second molar is similar to the first, except that the roots are shorter, the canals more curved, and the range of the variations broader. Very often (64%) the mesial root has two canals, approximately 38% incidence for Type II and 26% incidence for Type IV. In the distal root, there is almost always only one independent canal (92%) (Type I), rarely Type II (3%) or Type IV (4%). When Type I is a single canal extends from the pulp chamber to the apex; Type II are two separate canals leave the pulp chamber and join short of the apex to form one canal and the Type IV are two separate and distinct canals extend from the pulp chamber to the apex. This case report describes the orthograde endodontic retreatment performed on a mandibular second molar with four separate roots and canals, diagnosed with chronic apical periodontitis. This status resulted as a consequence of the failure of the first endodontic treatment performed, where the disto-buccal (DB) canal was undetected and untreated.
Case Report
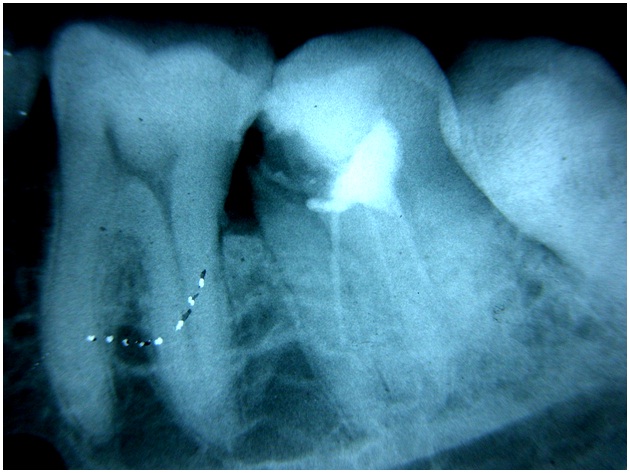
A 45-year-old male patient was referred by a general practitioner (GP) for endodontic orthograde retreatment on tooth no. 37. Intraoral periapical radiograph confirmed that the patient had a deficient previous root canal treatment on the mandibular left second molar, with incomplete root canal fillings on both mesial and distal roots, with chronic apical periodontitis, but with no clinical significant symptomatology [Table/Fig-1]. At a careful examination of the pre-operative periapical X-ray, the tooth seemed to have four separate roots and canals, where the disto-buccal (DB) canal was undetected and untreated. The patient was informed about the procedure to be done and an informed consent was obtained.
After giving local anaesthesia with 2% lignocaine with epinephrine (1:100000), the tooth no. 37 was isolated with rubber dam and clamp (Hygenic, Coltene Whaledent, USA). The access cavity was refined with an Endo Access bur number A0164 (Dentsply Maillefer, Switzerland) and all the caries and the former composite coronal restoration material was removed. When exposing the pulp chamber floor, a lot of debris, sealer and gutta-percha were observed. The re-treatment was done after removing the gutta-purcha using protaper retreatment files. The pulp chamber was thoroughly rinsed with 3% sodium hypochlorite solution and the pulpal floor was carefully examined under magnification with Dental Operating Microscope (Seiler, St.Louis, Missouri, USA) using an endodontic probe (DG16, Hu Friedy, USA). The canal fillings were former performed with gutta-percha and sealer, with the appearance of two master cones in the mesial side (one mesio buccal and one mesio lingual), and one in the distal side. When exploring this area with a size 10 stainless steel K-files (Kerr Manufacturing Co., Romulus, MI), the presence of the second distal canal, the distobuccal, was confirmed. This canal was undetected and unshaped by the GP. Gutta-percha from the distolingual, mesiobuccal and mesiolingual canal was removed with ProTaper Universal System (Dentsply Maillefer, Ballaigues, Switzerland) rotary instruments for retreatment. These nickel-titanium rotary instruments were used in a crown-down manner in combination with a torque-controlled engine (X-SmartTM Endodontic Motor, Dentsply, UK) at 300 rpm, according to the manufacturer’s instructions. The root-filling material was gradually removed using light apical pressure, until the working length was reached with D3, size 20 instrument. The D1 instrument was first used to create a pilot hole into the filling material; then the D2 instrument was used in the middle third of the root canal and the D3 in the apical part of it. The working length was confirmed by electronic measurement with an apex locator, Root ZX II (J. Morita Corp., Tokyo, Japan) and stainless-steel K-files. Apical enlargement was then performed with ProTaper Universal instruments F1 and F2.
Root canals were intermittently and copiously irrigated with 5 mL of NaOCl 5.25% after each instrument change. Irrigation with NaOCl alternated with 17% EDTA solution during and after the instrumentation, to remove the smear layer. Patency was assured on each of the root canals with a size 10 K-file. After completing cleaning and shaping of all the four root canals, final irrigation with sodium hypochlorite, sterile saline and 2% chlorhexidine solution for 5 min in each root canal was performed. The canals were dried with sterile paper points and an interim dressing of calcium hydroxide and 2 % chlorhexidine was placed as medication in each root canal for 2 weeks.
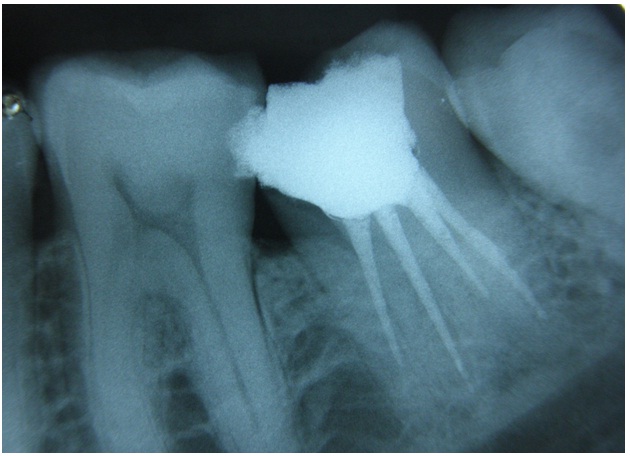
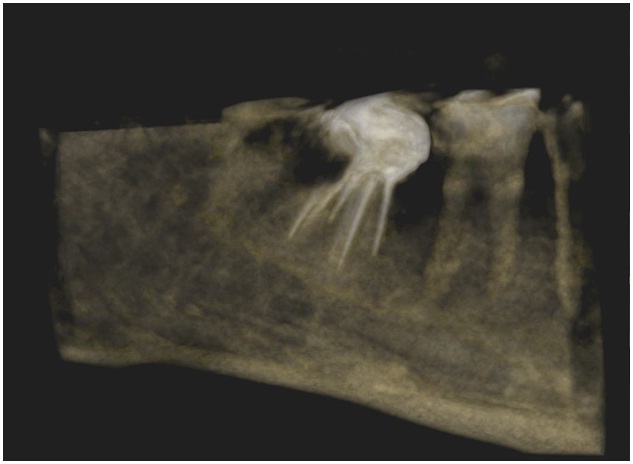
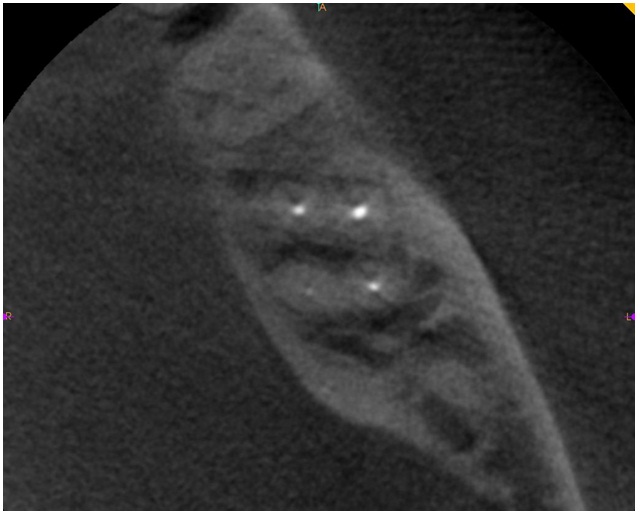
In the second appointment, the calcium hydroxide dressing was removed, the canals were rinsed, and each of the four canals was gauged using hand K-files attached to the apex locator. The canals were irrigated again, dried with sterile -paper points and the gutta-percha master cones (F2, size 25), were cut to fit at 0.5 mm of the working length for each root canal. Each selected master cone was then cemented into the corresponding root canal with AH Plus sealer (Dentsply Maillefer, Ballaigues, Switzerland). Then, a postobturation radiograph was taken [Table/Fig-2]. The permanent restoration of tooth was made with amalgam restoration. A Cone Beam Computerized Tomography (CBCT) scan was taken to evaluate the quality of the performed endodontic treatment [Table/Fig-3]. Axial section CBCT image clearly demonstrates the presence of four separate roots associated with the four canals in relation to 37 [Table/Fig-4]. When the patient was reviewed after two months, there was not any abnormality detected radiologically and clinically. Following this, a metal ceramic crown was cemented using Type I Glass ionomer cement.
Pre-operative radiograph of the tooth 37. Note the improper root canal fillings, undetected and untreated disto-buccal root
Post-obturation radiograph of tooth 37
Post-operative three-dimensional CBCT image of tooth 37
Axial section CBCT image showing the tooth 37 with four separate roots and canals
Discussion
The basic precondition for successful root canal treatment is to seal the root canal system completely through a thorough mechanical and chemical debridement of the entire root canal, followed by three-dimensional obturation with an inert filling material and a final coronal restoration, thereby preventing from reinfection of microorganisms [5] . Careful assessment of the pre-operative radiograph is a key step for root canal preparation and obturation. High quality pre-operative radiographs and their careful examination are essential for the detection of additional root canals [6] . Walton [7] recommended the use of two diagnostic radiographs. Anatomically, the teeth do not always have a normal shape. A great number of variations may occur in formation, number of roots, and their shape. However, dentists must have an awareness of the presence of rare anatomical variation; even though abnormalities are rare [8] .
In the present case report, the endodontic retreatment was necessary because of the presence of apical periodontitis, as a consequence of an improper former root canal therapy performed one year ago. Cases of retreatment always begin with a careful examination of the endodontic morphology of the involved tooth on pre-operative radiographs, because many times the failure of the first performed therapy is caused by a missed and untreated root canal. Endodontic retreatment is much more difficult than primary root canal treatment because of the presence in the root canal of filling materials, broken instruments or even ledges that sometimes make the renegotiation of the root canal impossible on its entire working length [9,10] . Although a lot of solvents can be used to remove the filling materials from the endodontic space, in this case only ProTaper Universal rotary instruments for retreatment were used, under copious irrigation with sodium hypochlorite and EDTA solution. Finishing of the root canal preparation was done by using ProTaper finishing files.
The retreatment was performed in this case in two appointments only because of the complexity of the endodontic anatomy. Between the two appointments, calcium hydroxide/ 2% chlorhexidine was placed as medication in the root canals for two weeks, in order to kill the micro-organisms un-destroyed by the irrigation protocol. As an intra-canal medication, calcium hydroxide/ 2% chlorhexidine combination had significantly more antibacterial activity[11] . In this case, a postoperative CBCT scan was taken to evaluate the quality of the performed endodontic treatment and to confirm the presence of four separate roots associated with the four canals in relation to mandibular left second molar [12] .
Conclusion
The main goal of this case study is to report a successful endodontic retreatment of a mandibular second molar with four separate roots and canals. Missing a supplementary canal, improper cleaningshaping- obturation will lead to endodontic failure, which sooner or later will consist in an apical periodontitis. Good knowledge of the endodontic anatomy and of its variations, careful interpretation of pre-operative periapical X-rays, magnification and illumination under the Operating Microscope, improves the predictability and the long term success of root canal treatment and retreatment.
[1]. P Krasner, HJ Rankow, Anatomy of pulp chamber floorJ Endod 2004 30:5-16. [Google Scholar]
[2]. RC Burns, LS Buchanan, Tooth morphology and access openings. In Cohen S, Burns RC (eds). Pathways of the pulp 1994 6th EditionMosbySt. Louis:243-247. [Google Scholar]
[3]. JA Soares, RT Leonardo, Root canal treatment of three rooted maxillary first and second premolars-a case reportInt Endod J 2003 36:705-10. [Google Scholar]
[4]. FJ Vertucci, Root canal anatomy of the human permanent teethOral Surg Oral Med Oral Pathol 1984 58:589-99. [Google Scholar]
[5]. FJ Vertucci, Root canal morphology and its relationship to endodontic procedures.Endodontic Topics. 2005 10:3-29. [Google Scholar]
[6]. RR Slowely, Radiographic aids in the detection of extra canalsOral Surg, Oral Med Oral Pathol. 1974 37:762-72. [Google Scholar]
[7]. RE Walton, Endodontic radiographic techniques.Dent radio Photo radio 1973 46:51-59. [Google Scholar]
[8]. G Jamileh, N Neda, Z Mina, R Ehsan, Mandibular first molar with four distalcanals. J Endod 2007 33:1481-3. [Google Scholar]
[9]. A Stabholz, S Friedman, Endodontic retreatment-case selection and technique. Part 2: treatment planning for retreatment.J Endod 1988 14:607-14. [Google Scholar]
[10]. S Friedman, A Stabholz, A Tamse, Endodontic retreatment-case selection and technique. Part 3: retreatment techniquesJ Endod 1990 16:543-49. [Google Scholar]
[11]. A DeRossi, LA Silva, MR Leonardo, Effect of rotary or manual instrumentation, with or without calcium hydroxide/1% chlorhexidine intracanal dressing, on the healing of experimentally induced chronic periapical lesions.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005 99:628-34. [Google Scholar]
[12]. WC Scarfe, AG Farman, P Sukovic, Clinical applications of cone-beam computed tomography in dental practiceJ Can Dent Assoc 2006 72:75-80. [Google Scholar]