Herbal toothpowders are available in market in a wide varieties, which consist of various ingredients. In rural areas of the developing countries, they are still used for cleansing teeth. Erythema multiforme (EM) is an acute mucocutaneous disorder that is believed to be a sequel of a cytotoxic immunologic attack on keratinocytes which express non-self-antigens. A 31-year-old male who used herbal toothpowder for oral-hygiene maintenance presented with ulcers in mouth, encrustation on lips and target lesions on both hands, suggesting Erythema multiforme. An oral biopsy confirmed the diagnosis.
To the best of our knowledge, there is no report of an association of herbal extracts and EM in the English literature. With this report, we present a rare new triggering factor of Erythema mutiforme, thus adding it to the endless list of aetiologies.
Herbal toothpowder, Erythema multiforme, Antigens, Hypersensitivity reaction
Case Report
A 31-year-old male presented to the Outpatients Department of our institute with complaints of pain and ulcers in mouth of 7 days duration. History revealed that complaints had started 7 days back. Initially, to start with, there was redness in the oral cavity and over lips. Soon, blisters developed, which ruptured to form bleeding ulcers in mouth and encrustations over lips. The ulcers were extremely painful, the pain was sharp, continuous, non-radiating and it aggravated on mastication and speech. No history of a febrile episode was present. There was no history of drug intake before the onset of these lesions. No other member of the patient’s family had similar symptoms. Only positive history was that patient had used a herbal toothpowder for teeth cleaning for 2 days before start of symptoms. On clinical examination, there was presence of “target lesions” on the extensor surfaces of both hands [Table/Fig-1]. These lesions showed central pallor, raised erythematous borders and surrounding layers of lighter erythema.. On oral examination, lips were found to be erythematous and they showed brown encrustations [Table/Fig-2]. Multiple erythematous ulcers were present on buccal mucosa bilaterally, on dorsal as well as ventral surfaces of tongue, floor of mouth, hard and soft palates [Table/Fig-3]. The ulcers were diffuse, irregular in shape, with indurated bases and everted edges. Pharyngeal and laryngeal examinations showed normal pictures. Submental, submandibular and cervical lymph nodes were non-palpable, no other mucous membranes were involved.
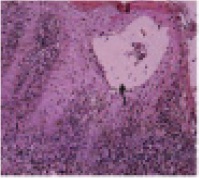
Routine haematological investigations were within normal range. Fasting ESR was 18mm in first hour by Westergren method. Liver function test and kidney function test gave normal results. Investigations done for Hepatitis B, Hepatitis C, HIV were normal. An incisional biopsy of right buccal mucosa was performed. The haematoxylin and eosin stained tissue sections showed intraepithelial vesicles. An intense chronic inflammatory cell infiltrate was found in the lamina propria [Table/Fig-4].
No acantholysis or separation of the epithelium from lamina propria was found and vesiculobullous diseases such as Pemphigus vulgaris, Cicatricial pemphigoid were ruled out. Although histopathological features were not pathognomonic, they were characteristic for diagnosis of EM. No immunofluorescence or immunohistochemistry analyses were performed, because these special procedures were unlikely to provide any useful information for final histopathological diagnosis of EM.
Patient was asked to strictly discontinue the use of the herbal toothpowder. Mouthwashes containing local anaesthetics and antiseptics were advised for symptomatic relief. He was treated with 10 mg prednisolone 3 times daily for 7 days. Within 7 days, all the oral as well as skin lesions healed [Table/Fig-5,6]. Prednisolone was then stopped after a tapering dose was given over next 7 days. Regular follow-up for a period of 1 year showed no recurrence of the lesion.

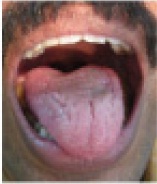
Encrustation on lips, diffuse ulceration on tongue

Diffuse ulceration on buccal mucosa and hard palate

Intraepithelial vesicle (arrow) and intense chronic inflammatory cell infiltrate
Post treatment, Healed ulcers on buccal mucosa

Post treatment, Healed ulcers on tongue and lips
Discussion
Use of herbal toothpowders for oral hygiene maintenance is a common practice in India. These toothpowders contain extracts of various medicinal plants. The major ingredients include Mimusops elingi, Anacyclus pyrethrum, Syzygium aromaticum, Embelia ribes, Randi dumetorum, etc [1].
Erythema multiforme (EM) and related disorders comprise a group of mucocutaneous disorders which are characterized by variable degrees of mucosal and cutaneous blistering and ulcerations that occasionally can give rise to systemic upset and possibly, a compromised life [2].
EM has been reported to be triggered by numerous agents, particularly viruses like Herpes simplex virus, Varicella zoster virus; bacteria like Mycoplasma pneumonia; certain immune conditions; food additives and chemicals; drugs like sulphonamides, cephalosporins [3].
The aetiology of EM is unclear in most of the patients, but it appears to be an immunological hypersensitivity reaction, with the appearance of cytotoxic effector cells, CD8+ T lymphocytes in the epithelium, inducing apoptosis of scattered keratinocytes and leading to satellite cell necrosis [4].
EM has been classified into a number of variants, mainly minor and major forms. EM minor (EMm) is mainly a cutaneous disease. A mucosal involvement is uncommon and when it is present, only one site is affected, most commonly the mouth. EM major (EMM) typically involves two or more mucous membranes with a more variable skin involvement. Symmetricaly distributed typical cutaneous target lesions and/or atypical raised target lesions are the hallmark [5].
The oral lesions initially manifest with oedema, erythema, and erythematous macules of the lips and buccal mucosa, followed by the development of multiple vesicles and bullae, that quickly rupture and result in pseudomembrane formations. The lips tend to become swollen and they show diagnostically distinctive bloody excrustations [6].
EM is a disorder that reacts primarily to antigens that are induced by exposure to microbes or drugs [6]. In the present case, the triggering factors for the causation of EM were the ingredients of the herbal formulation which was used by the patient for teeth cleaning. The exact pathogenesis of EM is unknown. It has been suggested that an immunologically mediated (i.e., lymphocytic) reaction to an infectious agent or a drug leads to skin and mucosal lesions which are concentrated at the dermalepithelial junction. In Herpes associated EM, it is most likely that HSV-DNA fragments in the skin or mucosa precipitate the disease [6]. CD34+ cells transport fragments of HSV to the epithelium, and T cells accumulate in response to HSV antigens and damage cells. In contrast, drug-associated EM seems to involve CD8+ T-cell attack and expression of tumour necrosis factor alpha (TNFα) in lesional skin, in the absence of HSV-DNA [7].
In the present case, it was likely that the herbal product had induced a hypersensitivity reaction in the patient, which had resulted in EM. A complete blood count is usually not helpful, although in severe EM, there is usually a rise in the erythrocyte sedimentation rate [8].
The diagnosis is usually supported by a perilesional tissue biopsy and exclusion of other causes. A histological examination and immunostaining often show moderate to dense perivascular inflammatory infiltrates (CD4+ Lymphocytes and histocytes) within the papillary dermis and along the dermoepidermal junction, dermal oedema, intraepithelial/subepithelial vesicles and/or bullae, hydropic degeneration of basal keratinocytes and non-specific immune deposits of IgM, C3 and fibrin along basement membrane [4,9]. Direct and indirect immunofluorescence is generally unhelpful, except that it helps in excluding other vesiculobullous disorders.
The management of EM can be difficult. There are no available systematic reviews, and randomized controlled trials are scarce. Any precipitants should be removed or treated. Casual drugs should be stopped and relevant infections should be treated. Antimicrobial agents can be used. Mouthwashes which contain local anaesthetics and antiseptic compounds may help in relieving painful oral symptoms. Analgesics and a liquid diet may be necessary. In severe forms of EM, hospital and supportive care are often important. Corticosteroids which are used topically or systemically are the drugs most commonly used in the management of EM. Immunomodulatory drugs such as cyclophosphamide, dapsone, cyclosporine, levamisole, thalidomide or interferon-α may also be used [10].
Conclusion
We have reported a case of EM which was induced by a unique causative agent, i.e. a herbal formulation. The case was treated routinely, with no evidence of recurrence. It can be concluded that, inspite of several factors being implicated, the exact aetiology of EM is still uncertain. The specific pathogenic mechanisms, as well as the multifactorial development hypothesis of the lesions are still being investigated. The treatment, except for symptomatic therapy with antiseptics, analgesics and antibiotics, is still being adopted for prophylaxis, control and elimination of the possible related underlying cause.
[1]. M Gupta, M Lavhale, S Nayak, Evaluation of Herbal toothpowder for it’s piperine contentAnc Sci Life 2005 24:126-30. [Google Scholar]
[2]. PS Kohli, J Kaur, Erythema multiforme-Oral variant: case report and review of literature.Indian J Otolaryngol Head Neck Surg 2011 63:S9-s12. [Google Scholar]
[3]. P Farthing, JV Farthing, C Scully, Erythema multiforme.Oral dis 2005 11:261-7. [Google Scholar]
[4]. L Ayangco, RS Rogers, 3rd RS, Oral manifestations of erythema multiformeDermatol Clin 2003 21:195-205. [Google Scholar]
[5]. KA Al-Johani, S Fedele, SR Porter, Erythema multiforme and related disordersOral Surg Oral Med Oral Pathol Oral Radiol Endod 2007 103:642-54. [Google Scholar]
[6]. S Imafuku, H Kokuba, L Aurelian, J Burnett, Expression of herpes simplex virus DNA fragments located in epidermal keratinocytes and germinative cells is associated with the development of erythema multiforme lesionsJ Invest Dermatol 1997 109:550-6. [Google Scholar]
[7]. SR Knowles, J Uetrecht, NH Sheas, Idiosyncratic drug reactions: the reactive metabolite syndromes.Lancet. 2000 356:1587-91. [Google Scholar]
[8]. L Aurelian, F Ono, J Burnett, Herpes simplex virus (HSV)- associated erythema multiforme (HAEM): a viral disease with an autoimmune componentDermatol Online J. 2003 :9-1. [Google Scholar]
[9]. WW Howland, LE Golitz, WL Weston, JC Huff, Erythema multiforme: clinical, histopathologic, and immunologic study.J Am Acad Dermatol 1984 10:438-46. [Google Scholar]
[10]. MG Stewart, NO Duncan III, DJ Franklin, EM Friedman, M Sulek, Head and neck manifestations of erythema multiforme in children.Otolaryngol Head Neck Surg. 1994 111:236-42. [Google Scholar]